Download as pptx, pdf, or txt
You might also like
- Can Ovulation InduCan Ovulation Induction Be Accelerated in Women Who Have PCOS-related Infertility?Document3 pagesCan Ovulation InduCan Ovulation Induction Be Accelerated in Women Who Have PCOS-related Infertility?James FlanneryNo ratings yet
- Impact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesDocument8 pagesImpact of Endometrial Preparation Protocols For Frozen Embryo Transfer On Live Birth RatesSri HariNo ratings yet
- Prenatal CareDocument33 pagesPrenatal CareJemi LoriNo ratings yet
- Fertility Preservation LectureDocument33 pagesFertility Preservation LectureDr. Abha MajumdarNo ratings yet
- 2015 Ovulation-InductionDocument11 pages2015 Ovulation-InductionMARIAPAULACASTILLO1No ratings yet
- Induction of LabourDocument45 pagesInduction of LabourVidya RamanathanNo ratings yet
- MonitoringDocument5 pagesMonitoringDessyNo ratings yet
- Dr. Ni Made Indri - CC For Ovulation InductionDocument26 pagesDr. Ni Made Indri - CC For Ovulation InductionAPOTEK Sarah FarmaNo ratings yet
- Assisted Reproductive Technology: Shanty Olivia F.JDocument41 pagesAssisted Reproductive Technology: Shanty Olivia F.Jshanty Olivia jasirwan100% (1)
- 1 Gestational-Trophoblastic-DiseasesDocument32 pages1 Gestational-Trophoblastic-Diseasespecolaa3No ratings yet
- Can Serum Progesterone Concentration Direct A FresDocument8 pagesCan Serum Progesterone Concentration Direct A FresashrafmogyNo ratings yet
- Thatcher2002 PDFDocument12 pagesThatcher2002 PDFAh MagdyNo ratings yet
- Hypothyroidism and InfertilityDocument19 pagesHypothyroidism and Infertilitysandeepdogra5357No ratings yet
- Review: Treatment of Necrotizing Enterocolitis: Cynthia D. Downard, Elizabeth Renaud, & Gudrun AspelundDocument58 pagesReview: Treatment of Necrotizing Enterocolitis: Cynthia D. Downard, Elizabeth Renaud, & Gudrun AspelundFarica Armane AquinoNo ratings yet
- Can Serum Progesterone Concentration Direct A FresDocument7 pagesCan Serum Progesterone Concentration Direct A FresashrafmogyNo ratings yet
- IVF-recent Research and Clinical Guideline-2007Document9 pagesIVF-recent Research and Clinical Guideline-2007QuackeryNo ratings yet
- EINCDocument69 pagesEINCNicole GadrinabNo ratings yet
- Jurnal FERDocument38 pagesJurnal FERAgus WijayaNo ratings yet
- Induction of LabourDocument59 pagesInduction of LabourFadiaislamiNo ratings yet
- Single Versus Double Intrauterine Insemination in Controlled Ovarian Stimulation Cycles For Subfertile MalesDocument6 pagesSingle Versus Double Intrauterine Insemination in Controlled Ovarian Stimulation Cycles For Subfertile MalesmasdipoNo ratings yet
- Ovarian Ageing and Management SASOG 2018Document57 pagesOvarian Ageing and Management SASOG 2018Sagie NaiduNo ratings yet
- 2.5 Preterm Labour: 2 Complications of PregnancyDocument8 pages2.5 Preterm Labour: 2 Complications of PregnancykukadiyaNo ratings yet
- Lawrenz 2019Document6 pagesLawrenz 2019angelNo ratings yet
- Female Sub FertilityDocument75 pagesFemale Sub FertilityIshaThapaNo ratings yet
- Ectopic PregDocument6 pagesEctopic PregYwagar Ywagar0% (1)
- A. Introduction: 1. BackgroundDocument4 pagesA. Introduction: 1. BackgroundAndi NurhidayahNo ratings yet
- Beta HCG Facts: Progesterone) Which Is Necessary For Implantation of The EmbryoDocument8 pagesBeta HCG Facts: Progesterone) Which Is Necessary For Implantation of The EmbryopawchanNo ratings yet
- The Clinical Content of Pre Conceptional Care Reproductive HistoryDocument3 pagesThe Clinical Content of Pre Conceptional Care Reproductive Historyarkanthos77No ratings yet
- Infertility Investigation: Roll - No.19058Document23 pagesInfertility Investigation: Roll - No.19058kushalNo ratings yet
- The Influence of Body Weight On Response To Ovulation Induction With Gonadotrophins in 335 Women With World Health Organization Group II Anovulatory InfertilityDocument8 pagesThe Influence of Body Weight On Response To Ovulation Induction With Gonadotrophins in 335 Women With World Health Organization Group II Anovulatory InfertilityCarlos ParraNo ratings yet
- Jurnal Riza T1A-1Document17 pagesJurnal Riza T1A-1Riza RsNo ratings yet
- Gestational AgeDocument34 pagesGestational AgeAaliyaan KhanNo ratings yet
- 2018 Article 432Document8 pages2018 Article 432Hartanto LieNo ratings yet
- Ectopic PregnancyDocument46 pagesEctopic PregnancyNoegi AkasNo ratings yet
- Management of Fetal Distress: Julian N. Robinson Brigham & Women's HospitalDocument78 pagesManagement of Fetal Distress: Julian N. Robinson Brigham & Women's HospitalLynda Ayu Prantika IINo ratings yet
- TestosteronDocument8 pagesTestosteronAndrea VargaNo ratings yet
- Evaluation of The Efficacy and Safety of Foley Catheter Pre-Induction of LaborDocument2 pagesEvaluation of The Efficacy and Safety of Foley Catheter Pre-Induction of LaborLauren RenNo ratings yet
- Diagnosis of PregnancyDocument23 pagesDiagnosis of PregnancyNeelesh BhandariNo ratings yet
- Failed of LaborDocument12 pagesFailed of LaborStéphanieNo ratings yet
- Out PDFDocument7 pagesOut PDFYuli HdyNo ratings yet
- External VersonDocument23 pagesExternal VersonNishaThakuriNo ratings yet
- Weight Loss InterventionDocument21 pagesWeight Loss InterventionsamuelionardiNo ratings yet
- Failure To Progress During Labor (35 Percent) : There Are No Absolute Contraindications To Cesarean DeliveryDocument20 pagesFailure To Progress During Labor (35 Percent) : There Are No Absolute Contraindications To Cesarean DeliveryHiba AliNo ratings yet
- Induction of Labor Using Foley Catheter With Weight Attached Vs Without WeightDocument14 pagesInduction of Labor Using Foley Catheter With Weight Attached Vs Without Weightgrace liwantoNo ratings yet
- Lab Session 3 - InfertilityDocument28 pagesLab Session 3 - InfertilityMeme 1234No ratings yet
- Oxitocina Vs Pgf2aDocument3 pagesOxitocina Vs Pgf2aRebecaNo ratings yet
- Frozen Embryo Transfer Cycles-SarhanDocument39 pagesFrozen Embryo Transfer Cycles-SarhanMaged BedeawyNo ratings yet
- Fertility and Sterility Treating Hydrosalpinx With A Manual Physical TherapyDocument1 pageFertility and Sterility Treating Hydrosalpinx With A Manual Physical TherapyClearPassageNo ratings yet
- Humanities-Low Dose Gonadotropin Protocol For Ovulation Induction in Low Resource Centre-Dr A. I. IsawumiDocument8 pagesHumanities-Low Dose Gonadotropin Protocol For Ovulation Induction in Low Resource Centre-Dr A. I. IsawumiBESTJournalsNo ratings yet
- Endoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokDocument37 pagesEndoscopy and Sedation: DR - Malavan Habeeb Internist & GI Endoscopist Lecturer - College of Medicine University of DuhokMalavan MohammedNo ratings yet
- Infertility Management RafiqDocument56 pagesInfertility Management RafiqratujelitaNo ratings yet
- Basic Infertility EvaluationDocument13 pagesBasic Infertility EvaluationRosu GeorgeNo ratings yet
- Jbra1117 PDFDocument4 pagesJbra1117 PDFAgusNo ratings yet
- Testing During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, UtDocument54 pagesTesting During Pregnancy: David G. Grenache, PHD University of Utah & Arup Laboratories Salt Lake City, Utمحمد عمران راناNo ratings yet
- Assessment of Fetal WellbeingDocument42 pagesAssessment of Fetal WellbeingMLV AbayNo ratings yet
- Randomised Controlled Trial: 2020 John Wiley & Sons LTDDocument8 pagesRandomised Controlled Trial: 2020 John Wiley & Sons LTDGuruh PanjiNo ratings yet
- Minimal Stimulation and Natural Cycle in Vitro Fertilization by Gautam N. Allahbadia, Markus Nitzschke (Eds.)Document114 pagesMinimal Stimulation and Natural Cycle in Vitro Fertilization by Gautam N. Allahbadia, Markus Nitzschke (Eds.)Quản Anh DũngNo ratings yet
- Malpresentation: Presented By: Dr. Nico Poundra Mulia Moderator: Dr. Fatmah Oktaviani, SpogDocument28 pagesMalpresentation: Presented By: Dr. Nico Poundra Mulia Moderator: Dr. Fatmah Oktaviani, SpogaispoundraNo ratings yet
- Ellenbogen 2020Document17 pagesEllenbogen 2020MD LarasatiNo ratings yet
- Recurrent Pregnancy LossFrom EverandRecurrent Pregnancy LossOle Bjarne ChristiansenNo ratings yet
- Individual Performance Commitment and Review (Ipcr)Document2 pagesIndividual Performance Commitment and Review (Ipcr)Reuben Jr UmallaNo ratings yet
- OB HX and PEDocument37 pagesOB HX and PEdenekeNo ratings yet
- Times Leader 05-05-2013Document75 pagesTimes Leader 05-05-2013The Times LeaderNo ratings yet
- Hydatidiform MoleDocument2 pagesHydatidiform MoleIrfan HardiNo ratings yet
- Immediate Postpartum Insertion of IUDDocument7 pagesImmediate Postpartum Insertion of IUDBmpNo ratings yet
- Aristo Ch.32 Textbook AnswersDocument9 pagesAristo Ch.32 Textbook AnswersyanaaNo ratings yet
- Piette YBEOG 2020 The Pharmacodynamics and Safety of ProgesteroneDocument17 pagesPiette YBEOG 2020 The Pharmacodynamics and Safety of ProgesteronePaul PIETTENo ratings yet
- Abnormal Uterine BleedingDocument34 pagesAbnormal Uterine BleedingMohmmadRjab SederNo ratings yet
- Thinking About Having A Baby?: Most People Want To Become Parents One DayDocument2 pagesThinking About Having A Baby?: Most People Want To Become Parents One DayMaria Darve GuditoNo ratings yet
- Causes of Maternal Mortality and MorbidityDocument20 pagesCauses of Maternal Mortality and MorbidityRaNa MaYaaNo ratings yet
- Fertility and The Abortion-Crime DebateDocument43 pagesFertility and The Abortion-Crime Debateearl100% (1)
- Menstrual Cycle PhasesDocument2 pagesMenstrual Cycle PhasesPatricia G ChiuNo ratings yet
- Biology Investigatory Project: TopicDocument13 pagesBiology Investigatory Project: TopicRaj SahuNo ratings yet
- Abortion Final DraftDocument7 pagesAbortion Final DraftKaleo Regalmuto0% (1)
- Pharm C Exam 10 Drug ListDocument2 pagesPharm C Exam 10 Drug ListVokdadaNo ratings yet
- Et 2011 Edhs PDFDocument450 pagesEt 2011 Edhs PDFhilegge7491No ratings yet
- Theories of LabourDocument22 pagesTheories of LaboursubashikNo ratings yet
- Pediatric Clinics June2012Document203 pagesPediatric Clinics June2012RIcardo Guerrero KananNo ratings yet
- RH LawDocument30 pagesRH LawElizar Vince Cruz100% (1)
- PB 110Document13 pagesPB 110Mona HelouNo ratings yet
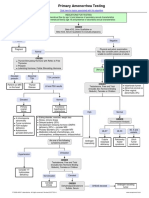
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Population Explosion WorksheetDocument6 pagesPopulation Explosion Worksheetapi-23660145No ratings yet
- A Position Paper On Giving of Condoms To Senior High School StudentsDocument2 pagesA Position Paper On Giving of Condoms To Senior High School StudentsHerschel Sophia NogueraNo ratings yet
- Drugs Affecting The Female Reproductive SystemDocument11 pagesDrugs Affecting The Female Reproductive Systemskz19914No ratings yet
- CF433 Medical Management of An Ectopic Pregnancy Using MethotrexateDocument11 pagesCF433 Medical Management of An Ectopic Pregnancy Using MethotrexateponekNo ratings yet
- Sex Education in Schools Argumentative EssayDocument2 pagesSex Education in Schools Argumentative EssayJameyza Garay DaytocNo ratings yet
- PapsmearDocument3 pagesPapsmearalmayasa2002No ratings yet
- Villafuerte For RevisionDocument19 pagesVillafuerte For RevisionqwertyNo ratings yet
- Sex Education IntroDocument6 pagesSex Education IntroJazmin CrisostomoNo ratings yet
- National HIV/STI Prevention ProgramDocument9 pagesNational HIV/STI Prevention ProgramJoezerk Jhon BielNo ratings yet