Download as pptx, pdf, or txt
You might also like
- Breast Cancer Radiation TherapyDocument439 pagesBreast Cancer Radiation TherapyJuan RivasNo ratings yet
- Colorectal CancerDocument3 pagesColorectal CancerAriane May Rubio50% (2)
- Fast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeFrom EverandFast Facts for Patients and Supporters: Cholangiocarcinoma: A cancer of the bile duct and liver Information + Taking Control = Best OutcomeNo ratings yet
- Pancreaticcancer 150917114601 Lva1 App6891Document30 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- 20.MBBS Pancreatic CancerDocument52 pages20.MBBS Pancreatic Cancermrajah95No ratings yet
- Pancreaticcancer 150917114601 Lva1 App6891Document25 pagesPancreaticcancer 150917114601 Lva1 App6891enam professorNo ratings yet
- Cancer of PancreasDocument50 pagesCancer of PancreasIsaac MwangiNo ratings yet
- Case Presentation: by DR SaleemDocument61 pagesCase Presentation: by DR SaleemsandeepNo ratings yet
- PancreatitisDocument51 pagesPancreatitisMizrab NadeemNo ratings yet
- Cancer of PancreasDocument46 pagesCancer of PancreasShriram SinghNo ratings yet
- MalarDocument41 pagesMalarமணிகண்டன் ராஜேந்திரன்No ratings yet
- Gall Bladder CarcinomaDocument29 pagesGall Bladder CarcinomaUsman FarooqNo ratings yet
- Ca Pancreas 44444Document52 pagesCa Pancreas 44444Mihraban OmerNo ratings yet
- Liver CancerDocument44 pagesLiver CancerJoyce Ann CumlatNo ratings yet
- Esophageal CADocument56 pagesEsophageal CAEdwin OkonNo ratings yet
- Referat CA PancreasDocument25 pagesReferat CA PancreasPamela VasikhaNo ratings yet
- Carcinoma Rectum - Janak - NEWDocument74 pagesCarcinoma Rectum - Janak - NEWTowhidulIslamNo ratings yet
- Liver CancerDocument44 pagesLiver CancerEjay Jacob Ricamara50% (2)
- Neoplasma of PankreasDocument33 pagesNeoplasma of PankreasGina Sonia RahmahNo ratings yet
- Ovarian CA 450918 SHDocument52 pagesOvarian CA 450918 SH180045No ratings yet
- Pancreas: DR Sigid Djuniawan, SPBDocument40 pagesPancreas: DR Sigid Djuniawan, SPBditaayupNo ratings yet
- Chronic Pancreatitis 2Document37 pagesChronic Pancreatitis 2Umulkheir ahmedNo ratings yet
- Carcinoma PancreasDocument14 pagesCarcinoma PancreasVerma JiNo ratings yet
- Esophageal CarcinomaDocument34 pagesEsophageal Carcinomaapi-19916399100% (1)
- Colon and Rectal CancerDocument62 pagesColon and Rectal CancerSK TalkNo ratings yet
- Liver Cancer: Angel Maria Cibichan 3 Year BSC .Nursing StconDocument69 pagesLiver Cancer: Angel Maria Cibichan 3 Year BSC .Nursing StconSamuel LalNo ratings yet
- L1 GIT OncologyDocument99 pagesL1 GIT OncologyPrincess FNo ratings yet
- Capancreas 160907124326Document34 pagesCapancreas 160907124326Ahlam Azam, MohamedNo ratings yet
- Esophageal CancerDocument25 pagesEsophageal CancerK poojithaNo ratings yet
- Seminar On Tumor of Genito-Urinary SystemDocument33 pagesSeminar On Tumor of Genito-Urinary SystemLakshay AroraNo ratings yet
- Urinary Tract CancerDocument53 pagesUrinary Tract CancerandikaisnaeniNo ratings yet
- Urological TumoursDocument68 pagesUrological TumoursDr Anais AsimNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza HospitalDocument83 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant Surgeon European-Gaza Hospitalpt.mahmoudNo ratings yet
- Bladder CancerDocument43 pagesBladder CancerIsaac MwangiNo ratings yet
- Small IntestineDocument4 pagesSmall IntestineSiruNo ratings yet
- Colon: Malueth AbrahamDocument39 pagesColon: Malueth AbrahamMalueth AnguiNo ratings yet
- Tumours of The Pancreas: Dr. Saleh M. Al SalamahDocument33 pagesTumours of The Pancreas: Dr. Saleh M. Al SalamahAdil ShabbirNo ratings yet
- Carcinoma StomachDocument51 pagesCarcinoma StomachOnkar SinghNo ratings yet
- Pancreatic Cancer: Pathophysiologic EtiologyDocument2 pagesPancreatic Cancer: Pathophysiologic EtiologyCharissa Magistrado De LeonNo ratings yet
- Chronic PancreatitisDocument51 pagesChronic PancreatitisAli Nawaz khanNo ratings yet
- Endomaterial Cancer-1Document28 pagesEndomaterial Cancer-1A.H.ANo ratings yet
- G.I Tumors-1 Esophagus and StomachDocument53 pagesG.I Tumors-1 Esophagus and StomachAjeet LohanaNo ratings yet
- Colorectal CancerDocument7 pagesColorectal Cancerjames garciaNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonDocument65 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonEslam R. Almassri100% (1)
- About Pancreatic CancerDocument8 pagesAbout Pancreatic Cancersummerland_5No ratings yet
- DysphagiaDocument40 pagesDysphagiamanabdebuNo ratings yet
- Principles of Surgical OncologyDocument34 pagesPrinciples of Surgical Oncologykaukab azim100% (1)
- Upper Git TumorsDocument51 pagesUpper Git TumorsIsaac MwangiNo ratings yet
- Gastric CancerDocument126 pagesGastric Cancermwani775100% (1)
- T5 Pancreas PDFDocument19 pagesT5 Pancreas PDFAmin ZahariNo ratings yet
- Pancreatic CancerDocument29 pagesPancreatic Cancermynoidanh19No ratings yet
- Management of Rectal Cancer... by DR Kassahun GirmaDocument50 pagesManagement of Rectal Cancer... by DR Kassahun GirmaKassahun Girma Gelaw100% (1)
- Malignant Breast DiseasesDocument40 pagesMalignant Breast DiseasesDavid MarkNo ratings yet
- CarcinomarectumDocument45 pagesCarcinomarectumHuzefa MemonNo ratings yet
- Carcinoma KidneyDocument12 pagesCarcinoma KidneyFadhilla AnasNo ratings yet
- NJHKJDocument12 pagesNJHKJFadhilla AnasNo ratings yet
- Colorectal CancerDocument39 pagesColorectal CancerFernando AnibanNo ratings yet
- gr.5 Colorectal CancerDocument9 pagesgr.5 Colorectal Cancerkeithlynd100% (1)
- CasediscussionDocument30 pagesCasediscussionFernando AnibanNo ratings yet
- Renal CancerDocument34 pagesRenal CancerArya100% (1)
- Pancreatic Cancer: A Comprehensive Resource for Patients and FamiliesFrom EverandPancreatic Cancer: A Comprehensive Resource for Patients and FamiliesNo ratings yet
- Prostate SECRETSFinal PDFDocument42 pagesProstate SECRETSFinal PDFdeiko1No ratings yet
- Health Psychology An Introduction To Behavior and Health 10Th Edition Linda Brannon Full ChapterDocument67 pagesHealth Psychology An Introduction To Behavior and Health 10Th Edition Linda Brannon Full Chaptersteven.kincaid536100% (5)
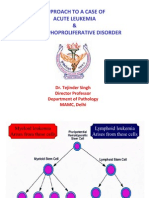
- 01 Approach To A Case Leukemia and Lymphoproliferative DisorDocument49 pages01 Approach To A Case Leukemia and Lymphoproliferative DisorcandiddreamsNo ratings yet
- Immuno2008, Vol.28, Issues 4, Intravenous Immunoglobulin Treatment of ImmunodeficiencyDocument187 pagesImmuno2008, Vol.28, Issues 4, Intravenous Immunoglobulin Treatment of ImmunodeficiencydudapaskasNo ratings yet
- Colon Cancer Overview: ElectrolytesDocument6 pagesColon Cancer Overview: ElectrolytesPranaliNo ratings yet
- ISOPP Standards of Practice - Safe Handling of CytotoxicsDocument104 pagesISOPP Standards of Practice - Safe Handling of CytotoxicsprovaoralNo ratings yet
- Hpeb 470 Healthcare and Culture Research Presentation Sabah BhamaniDocument14 pagesHpeb 470 Healthcare and Culture Research Presentation Sabah Bhamaniapi-543176372No ratings yet
- Grade 7 QuestionnaireDocument5 pagesGrade 7 QuestionnaireMarc T Montefalcon100% (2)
- Naprod Kaleidoscope Issue 2 - Naprod Life SciencesDocument5 pagesNaprod Kaleidoscope Issue 2 - Naprod Life SciencesNaprod Life Sciences Pvt. Ltd.No ratings yet
- Jurnal Ebm Kanker ServiksDocument12 pagesJurnal Ebm Kanker ServiksKarina UtariNo ratings yet
- Association Between Mir Let-7g Gene Expression and The Risk of Cervical Cancer in Human Papilloma Virus-Infected PatientsDocument8 pagesAssociation Between Mir Let-7g Gene Expression and The Risk of Cervical Cancer in Human Papilloma Virus-Infected PatientsGICELANo ratings yet
- Health Benefits of PomegranateDocument11 pagesHealth Benefits of PomegranateMaheshMaheNo ratings yet
- A Guide To Aim Global Business - TanzaniaDocument37 pagesA Guide To Aim Global Business - TanzaniaWa Tu LeeNo ratings yet
- Diet and HealthDocument4 pagesDiet and HealthR VNo ratings yet
- Hubungan Motivasi Deteksi Dini Kanker Serviks Dengan Tindakan Pap Smear Pada Wanita Usia Subur Di Wilayah GonilanDocument7 pagesHubungan Motivasi Deteksi Dini Kanker Serviks Dengan Tindakan Pap Smear Pada Wanita Usia Subur Di Wilayah Gonilanevi yulia arvensiNo ratings yet
- PBHRF Homeopathy of The 21st CenturyDocument60 pagesPBHRF Homeopathy of The 21st CenturyGeorge MontoyaNo ratings yet
- PRESENTIADocument14 pagesPRESENTIARabar Mohsin Abdulrahman MantikNo ratings yet
- Healthcare & Life Sciences ReviewDocument47 pagesHealthcare & Life Sciences Reviewmercadia59970% (1)
- Breast: Kurt'S NotesDocument4 pagesBreast: Kurt'S NotesfadoNo ratings yet
- Prostate Acinar Adenocarcinoma Gleason Grading: Often Disqualifies From Active SurveillanceDocument2 pagesProstate Acinar Adenocarcinoma Gleason Grading: Often Disqualifies From Active SurveillancePankaj DubeyNo ratings yet
- Madeline Bernard Resume May 2019Document4 pagesMadeline Bernard Resume May 2019api-455425299No ratings yet
- Francis E. Peters-Termenii Filozofiei Grecesti-Humanitas (1997)Document4 pagesFrancis E. Peters-Termenii Filozofiei Grecesti-Humanitas (1997)Iustinuan BlakyNo ratings yet
- Nursing Management of Stomach CancerDocument4 pagesNursing Management of Stomach CancerKian Herrera100% (2)
- Case Study For LeukemiaDocument5 pagesCase Study For LeukemiaGabbii CincoNo ratings yet
- Brain TumorsDocument19 pagesBrain TumorsMehjabin mohammedNo ratings yet
- Nejmoa1113162 AppendixDocument35 pagesNejmoa1113162 AppendixayuannisahusnaNo ratings yet
- MS Ii MT2Document11 pagesMS Ii MT2Rika MaeNo ratings yet
- Procedure 1 Brest Examination Self ExaminationDocument4 pagesProcedure 1 Brest Examination Self ExaminationPriyanka SheoranNo ratings yet
- Oncogenic VirusDocument74 pagesOncogenic VirusMike Serge RazafiNo ratings yet