Download as pptx, pdf, or txt
You might also like
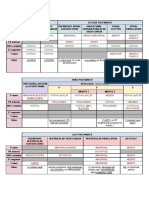
- ACLS Pocket Card PDFDocument6 pagesACLS Pocket Card PDFdang vu hoang ducNo ratings yet
- Cardiopulmonary Arrest Simulation LabDocument3 pagesCardiopulmonary Arrest Simulation LabJessica Mason100% (2)
- Atrial Fibrillation Topic DiscussionDocument23 pagesAtrial Fibrillation Topic Discussionapi-567600964No ratings yet
- CHANCE Trial AND POINT Trial EditDocument16 pagesCHANCE Trial AND POINT Trial EditnurdiansyahNo ratings yet
- Cyanotic Heart DiseaseDocument47 pagesCyanotic Heart Disease87-Saranya MNo ratings yet
- Hypercyanotic SpellDocument15 pagesHypercyanotic SpellNur Syuhada Roslan0% (1)
- Cardiovascular Physical TherapDocument7 pagesCardiovascular Physical TherapJadie Prenio100% (4)
- Tetralogy of FallotDocument26 pagesTetralogy of FallotGI SanadaNo ratings yet
- Odia Tetralogy of FallotDocument25 pagesOdia Tetralogy of Fallotvictorjonathan567No ratings yet
- Rheumatic Heart DiseaseDocument30 pagesRheumatic Heart DiseaseshariqraipkNo ratings yet
- Aortic Regurgitation by DR DilmoDocument37 pagesAortic Regurgitation by DR Dilmosinan kNo ratings yet
- Cyanotic Heart DiseaseDocument66 pagesCyanotic Heart DiseasePrasanth SankarNo ratings yet
- Tetralogy of Fallot (TOF) : Dr. Sayeedur Rahman Khan Rumi MD Final Part Student Nhfh&RiDocument49 pagesTetralogy of Fallot (TOF) : Dr. Sayeedur Rahman Khan Rumi MD Final Part Student Nhfh&RiPrazNo ratings yet
- Examination and Investigation of The Cardiovascular System (CVS)Document27 pagesExamination and Investigation of The Cardiovascular System (CVS)Jake MillerNo ratings yet
- Tof and PdaDocument47 pagesTof and PdaskerstinNo ratings yet
- Symptoms Signs Heart DiseaseDocument33 pagesSymptoms Signs Heart DiseaseEmereole FrancesNo ratings yet
- Life Threatening Congenital Heart Disease Edisi II Dr. Heny Martini, SPJP (K)Document66 pagesLife Threatening Congenital Heart Disease Edisi II Dr. Heny Martini, SPJP (K)Faruz Faruz RomadhonNo ratings yet
- K7 - Supraventricular Tachycardia (SVT)Document44 pagesK7 - Supraventricular Tachycardia (SVT)Zikri Putra Lan LubisNo ratings yet
- Cardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarDocument23 pagesCardiac Tamponade: Mrs. D.Melba Sahaya Sweety.D M.SC Nursing GimsarD. Melba S.S ChinnaNo ratings yet
- Congenital Heart DefectsDocument45 pagesCongenital Heart Defectskathylaine100% (1)
- Pulmonary EmbolismDocument5 pagesPulmonary EmbolismKian Justin HidalgoNo ratings yet
- University of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingDocument69 pagesUniversity of Saint Louis Tuguegarao City, Philippines: Maternal and Child Health NursingErica Veluz LuyunNo ratings yet
- Cardiac TamponadeDocument43 pagesCardiac TamponadeMădălina GreereNo ratings yet
- Penyakit Jantung Bawaan II - 2Document30 pagesPenyakit Jantung Bawaan II - 2ahmad syauqieNo ratings yet
- 01 Cardiovascular IDocument72 pages01 Cardiovascular IcoriezaNo ratings yet
- Acynotic Heart DiseasesDocument13 pagesAcynotic Heart DiseasesSimran JosanNo ratings yet
- ECMO Cardiopulmonary Support in Critically Ill ChildrenDocument68 pagesECMO Cardiopulmonary Support in Critically Ill Childrenapi-3831614No ratings yet
- Pediatric Heart FailureDocument34 pagesPediatric Heart FailuretoyyibNo ratings yet
- 5min Tet's SpellDocument24 pages5min Tet's SpellAsim Kumar BiswasNo ratings yet
- Examination of The Cardiovascular SystemDocument38 pagesExamination of The Cardiovascular Systemapi-19641337No ratings yet
- ACLS SubhankarDocument87 pagesACLS SubhankarMarc Andreo MalalaNo ratings yet
- Tetralogy of Fallot: DR Bhagirath S NDocument111 pagesTetralogy of Fallot: DR Bhagirath S NKunwar Sidharth SaurabhNo ratings yet
- CardiacassessmentDocument40 pagesCardiacassessmentsasNo ratings yet
- Obstructive Shock: Harrisons Principles of Internal MedicineDocument6 pagesObstructive Shock: Harrisons Principles of Internal MedicineMohammad Jofa Rachman PNo ratings yet
- Case Presentation: Congenital Heart DiseaseDocument37 pagesCase Presentation: Congenital Heart DiseaseKarin Nadia UtamiNo ratings yet
- Valvular Heart Disease To TW FinalDocument13 pagesValvular Heart Disease To TW FinalMohammed ElSayedNo ratings yet
- Cyanotic Congenital Heart DiseaseDocument22 pagesCyanotic Congenital Heart DiseaseRaviNo ratings yet
- JVP, Hs&coDocument29 pagesJVP, Hs&coVansh SinghNo ratings yet
- Valvular Heart DiseasesDocument60 pagesValvular Heart DiseasesEthiopia TekdemNo ratings yet
- Pathophysiology Congenital Heart Disease-1Document54 pagesPathophysiology Congenital Heart Disease-1single_ladyNo ratings yet
- Pemicu 6 KGD DeniseDocument95 pagesPemicu 6 KGD DeniseVincent VandestyoNo ratings yet
- Acyanotic Congenital Heart DiseaseDocument23 pagesAcyanotic Congenital Heart DiseasePernel Jose Alam MicuboNo ratings yet
- 10 Cardiology LectureDocument64 pages10 Cardiology Lectureaemy13266No ratings yet
- Pericardial EffusionDocument26 pagesPericardial EffusionjsenocNo ratings yet
- Congenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDDocument30 pagesCongenital Heart Disease: Kriti Puri, MD Hugh D. Allen, MD Athar M. Qureshi, MDhari ilman toniNo ratings yet
- Acute Arterial Occlusion and Other Arterial Diseases 2Document32 pagesAcute Arterial Occlusion and Other Arterial Diseases 2ningappaNo ratings yet
- Kardiogenik SyokDocument43 pagesKardiogenik SyokGalih Arief Harimurti WawolumajaNo ratings yet
- Cyanotic Heart LesionsDocument40 pagesCyanotic Heart LesionsRaison D'etreNo ratings yet
- Cardio-Respiratory Conditions: by DR Priscus MushiDocument73 pagesCardio-Respiratory Conditions: by DR Priscus MushiMusaNo ratings yet
- Heart FailureDocument77 pagesHeart FailureJudy Anne PatricioNo ratings yet
- Cardiovascular Physiology Case 9Document50 pagesCardiovascular Physiology Case 9Kim AcostaNo ratings yet
- Congestive Cardiac FailureDocument61 pagesCongestive Cardiac FailureYAMINIPRIYANNo ratings yet
- Cardiogenic ShockDocument49 pagesCardiogenic Shockmaibejose0% (1)
- Pulmonary Valve StenosisDocument6 pagesPulmonary Valve StenosisKobby AmoahNo ratings yet
- Decreased Pulmonary Blood Flow (CYANOTIC HEART DEFECTS)Document88 pagesDecreased Pulmonary Blood Flow (CYANOTIC HEART DEFECTS)leenaNo ratings yet
- Shock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreDocument22 pagesShock DR Sadia Hussain: Assistant Professor Pediatric Medicine King Edward Medical University LahoreTouseef Ur RehmanNo ratings yet
- Patofisiologi Shock CardiogenicDocument44 pagesPatofisiologi Shock CardiogenicGalih Arief Harimurti Wawolumaja100% (1)
- Pulmonary Embolus (PE)Document3 pagesPulmonary Embolus (PE)Heidi M FischerNo ratings yet
- Cardiac Tamponade (Suryani)Document72 pagesCardiac Tamponade (Suryani)Hamdani UsmanNo ratings yet
- Acynotic DiseaseDocument55 pagesAcynotic DiseaseTesfamichael AbathunNo ratings yet
- ACFrOgC-pzE5RQJIbCELZhV0cdk6ioDNIaJcmCjwqiRF DrvgVB6DZwpe H0xKtsQ-azwWzcoEmilNTpD-bIlbSmB5BUuUaB1XyQtaHmg4Ko6DsOFWTXCUb6HV9ROfpC cuspVp0vX5MLV8nPIBCDocument67 pagesACFrOgC-pzE5RQJIbCELZhV0cdk6ioDNIaJcmCjwqiRF DrvgVB6DZwpe H0xKtsQ-azwWzcoEmilNTpD-bIlbSmB5BUuUaB1XyQtaHmg4Ko6DsOFWTXCUb6HV9ROfpC cuspVp0vX5MLV8nPIBCClaire GidoNo ratings yet
- CVS Important PointsDocument22 pagesCVS Important PointsSAAD MIRZANo ratings yet
- Congenital Heart DiseaseDocument60 pagesCongenital Heart DiseaseBonfaceNo ratings yet
- Kuliah 16 Cor PulmonaleDocument41 pagesKuliah 16 Cor PulmonalecaturwiraNo ratings yet
- PreviewDocument37 pagesPreviewDavid Teoh100% (1)
- Congestive Heart FailureDocument13 pagesCongestive Heart FailureAgeng BudianantiNo ratings yet
- NCM 118 MIDTERMS PG 7Document1 pageNCM 118 MIDTERMS PG 7Kai SamaNo ratings yet
- Cardiac Disease in PregnancyDocument21 pagesCardiac Disease in PregnancyRenata CilestrinaNo ratings yet
- General Expressions in Medical DiagnosisDocument6 pagesGeneral Expressions in Medical DiagnosisSergej ElekNo ratings yet
- A 53 Years Old Woman With Hypertension Grade I and Diabetes Mellitus Type 2Document8 pagesA 53 Years Old Woman With Hypertension Grade I and Diabetes Mellitus Type 2Ani WulandariNo ratings yet
- Cardiac Arrest: Signs and SymptomsDocument7 pagesCardiac Arrest: Signs and SymptomsWebster The-TechGuy LunguNo ratings yet
- Cardio 7.4Document2 pagesCardio 7.4Абдул Насер МохаммадізмаелNo ratings yet
- Cardiac Cycle & Heart Sounds Flashcards - QuizletDocument11 pagesCardiac Cycle & Heart Sounds Flashcards - QuizletRadijska Postaja KoprivnicaNo ratings yet
- Pediatric ElectrocardiographyDocument7 pagesPediatric ElectrocardiographyTri NguyenNo ratings yet
- Interpretasi EKGDocument81 pagesInterpretasi EKGGyna MarsianaNo ratings yet
- Chapter 27 - Management of Patients With Dysrhythmias and ConductionDocument8 pagesChapter 27 - Management of Patients With Dysrhythmias and ConductionMichael Boado100% (1)
- Grade 1 Pattern of LV Diastolic FillingDocument3 pagesGrade 1 Pattern of LV Diastolic FillingNicoleNo ratings yet
- Conductive Disturbances: Rhythm vs. Conduction - Your Heart's Rhythm Is Its Pace or BeatDocument3 pagesConductive Disturbances: Rhythm vs. Conduction - Your Heart's Rhythm Is Its Pace or BeatSoleNo ratings yet
- Left Bundle Branch Block - UpToDateDocument25 pagesLeft Bundle Branch Block - UpToDateKrull TTTeamNo ratings yet
- StemiDocument11 pagesStemidoubleraNo ratings yet
- Elektrokardiografi: Prof. Dr. Peter KaboDocument49 pagesElektrokardiografi: Prof. Dr. Peter KaboRey AlwiwikhNo ratings yet
- Icd10 Congestive Heart FailureDocument2 pagesIcd10 Congestive Heart FailurerizkaNo ratings yet
- 01MED1SET2017Document292 pages01MED1SET2017Elison CarvalhoNo ratings yet
- Rheumatic Heart DiseaseDocument60 pagesRheumatic Heart DiseaseannisNo ratings yet
- Cor Pulmonale - A Student To Student GuideDocument4 pagesCor Pulmonale - A Student To Student GuideVaseem ZamairNo ratings yet
- Chd. AmiDocument4 pagesChd. AmiDead shotNo ratings yet
- ElectrocardiogramDocument169 pagesElectrocardiogramjitendra magarNo ratings yet
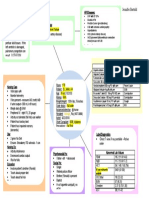
- CHF Concept MapDocument1 pageCHF Concept MapChristy Wegner Cooper100% (4)
- Clinical Spectrum of Atherosclerotic Heart DiseaseDocument50 pagesClinical Spectrum of Atherosclerotic Heart Diseaseadamu mohammadNo ratings yet