Download as ppt, pdf, or txt
You might also like
- King, Warrior, Magician, Lover TestDocument1 pageKing, Warrior, Magician, Lover TestpuffnprovNo ratings yet
- Allen Cognitive Level ScreenDocument9 pagesAllen Cognitive Level ScreenIntan Indah Sari100% (2)
- Selection ProcessDocument3 pagesSelection Processsara24391No ratings yet
- Impact of Disability and Vulnerability On Daily Life: Learning OutcomesDocument52 pagesImpact of Disability and Vulnerability On Daily Life: Learning OutcomesAsnake Yohanis67% (6)
- Chapter 3 - Identifications of Impacts of DisabilityDocument39 pagesChapter 3 - Identifications of Impacts of Disabilityshelema lemiNo ratings yet
- Chapter 3 FINAL Identification of The Impact of Disability & DifferentiatedDocument47 pagesChapter 3 FINAL Identification of The Impact of Disability & Differentiatednikodimosmelese21No ratings yet
- Chapter 3 - Identifications of Impacts of DisabilityDocument41 pagesChapter 3 - Identifications of Impacts of DisabilityNaol Zeleke100% (1)
- Inclusiveness: Addis Ababa University College of Education and Behavioral Studies Department of Special Needs EducationDocument49 pagesInclusiveness: Addis Ababa University College of Education and Behavioral Studies Department of Special Needs EducationĒrmias Álemayehu100% (2)
- Inclusive Ch3Document49 pagesInclusive Ch3samuelaklili1122No ratings yet
- Chapter 3 InclusivenessDocument48 pagesChapter 3 InclusivenessAgezeNo ratings yet
- Chapter 3 FINAL Identification of The Impact of Disability & DifferentiatedDocument49 pagesChapter 3 FINAL Identification of The Impact of Disability & Differentiatedyohannes lemi100% (1)
- InclusivenessDocument49 pagesInclusivenessDegefa DemessieNo ratings yet
- Chapter 3Document49 pagesChapter 3Melaku Walelgne100% (1)
- Chapter 3 FINAL Identification of The Impact of Disability & DifferentiatedDocument52 pagesChapter 3 FINAL Identification of The Impact of Disability & DifferentiatedHunde Adamu100% (1)
- Identification and Differentiated ServicesDocument214 pagesIdentification and Differentiated ServicesGetahun TukaNo ratings yet
- Inclusive AssignmentDocument15 pagesInclusive AssignmentDagim AbrehamNo ratings yet
- L4 Clientele and Audiences in SW - Characteristics and NeedsDocument47 pagesL4 Clientele and Audiences in SW - Characteristics and NeedssatomiNo ratings yet
- Inclusivness AssignmentDocument17 pagesInclusivness AssignmentEphrem ChernetNo ratings yet
- People With DisabilityDocument25 pagesPeople With DisabilityBinod Raj SubediNo ratings yet
- Chapter 3 FINAL Identification of The Impact of Disability & DifferentiatedDocument59 pagesChapter 3 FINAL Identification of The Impact of Disability & DifferentiatedYohannes BogaleNo ratings yet
- Inclusiveness: Addis Ababa University College of Education and Behavioral Studies Department of Special Needs EducationDocument50 pagesInclusiveness: Addis Ababa University College of Education and Behavioral Studies Department of Special Needs Educationharoine insider100% (1)
- Care Giver CourseDocument40 pagesCare Giver CourseushaNo ratings yet
- Ch. 19 DisabilitiesDocument16 pagesCh. 19 DisabilitiesJenn StyronNo ratings yet
- Ecdp Insight: Solutions For Disabled People by Disabled PeopleDocument83 pagesEcdp Insight: Solutions For Disabled People by Disabled PeopleecdpNo ratings yet
- Inclusive Chap 3Document50 pagesInclusive Chap 3Miley GirmayNo ratings yet
- Inclusive AssignmentDocument55 pagesInclusive AssignmentIbrahim SirajNo ratings yet
- Mainstreaming Disability ManyongeDocument51 pagesMainstreaming Disability Manyongerichardsimiyu100% (2)
- Community and Family Studies Year 12 2.1Document24 pagesCommunity and Family Studies Year 12 2.1Jade LyNo ratings yet
- Special Needs Education, PPT 1, 2 & 3 Combined-1Document132 pagesSpecial Needs Education, PPT 1, 2 & 3 Combined-1wongani phiri100% (1)
- PSY211 Lecture 12Document17 pagesPSY211 Lecture 12Hope MashakeniNo ratings yet
- Ass 2 2602Document8 pagesAss 2 2602keatlaretse macucwaNo ratings yet
- Diass Week 8 ActivityDocument2 pagesDiass Week 8 ActivityRv BlancoNo ratings yet
- Preliminary Course Community and Family StudiesDocument21 pagesPreliminary Course Community and Family StudiesSoph RocheNo ratings yet
- Inclusiveness (Chapter 1 & 2)Document71 pagesInclusiveness (Chapter 1 & 2)ffff100% (1)
- DR - EZAZ - 4 - Clients of Community HealthcareDocument17 pagesDR - EZAZ - 4 - Clients of Community HealthcaresazNo ratings yet
- Module 2 Geriatric Social Work PDFDocument6 pagesModule 2 Geriatric Social Work PDFParvathy ManojNo ratings yet
- Psychological First Aid - CrisisDocument90 pagesPsychological First Aid - CrisisSharmine NoganNo ratings yet
- Principles of Health and Social Care Session 2Document9 pagesPrinciples of Health and Social Care Session 2Tushar GajjarNo ratings yet
- Disability Inclusion Nov2022Document24 pagesDisability Inclusion Nov2022Abdi TeyibNo ratings yet
- Sociovocational Rehabiliotation/ Socioeconomic RehabilitationDocument32 pagesSociovocational Rehabiliotation/ Socioeconomic RehabilitationSonia guptaNo ratings yet
- Lo AssignmentDocument6 pagesLo Assignmentlwandlenkambule476No ratings yet
- Presentaion On Inclusiveness Chapter 3Document50 pagesPresentaion On Inclusiveness Chapter 3Addi89% (19)
- Social Work in Humanitarian Organisations (Asw121) 2019 SlidesDocument148 pagesSocial Work in Humanitarian Organisations (Asw121) 2019 SlidesHazvinei GwazeNo ratings yet
- LessonDocument17 pagesLessonDenene GerzeyeNo ratings yet
- A Better Life: What Older People With High Support Needs ValueDocument59 pagesA Better Life: What Older People With High Support Needs ValueDHila Fadhilah YusmanNo ratings yet
- Chapter 3 InclusivenessDocument55 pagesChapter 3 InclusivenessDesta EquarNo ratings yet
- Inclusive Chapter ThreeDocument21 pagesInclusive Chapter ThreeAbazer SultanNo ratings yet
- Unit-Ii Psychology of DisabilityDocument24 pagesUnit-Ii Psychology of DisabilityShubhashri AcharyaNo ratings yet
- Uself Lesson 7 The Social SelfDocument3 pagesUself Lesson 7 The Social SelfRhisza MedinaNo ratings yet
- Equality and DiversityDocument9 pagesEquality and DiversityJames OtunNo ratings yet
- Voluntary ChildlessnessDocument8 pagesVoluntary Childlessnessravism3No ratings yet
- EssayDocument6 pagesEssaysanju.kumar9363No ratings yet
- 8.1 The Causes of PovertyDocument7 pages8.1 The Causes of PovertyShanzeh WaheedNo ratings yet
- Social Services Lecture 6Document22 pagesSocial Services Lecture 6mudassirali7711No ratings yet
- Social StratificationDocument46 pagesSocial StratificationJanee JaneNo ratings yet
- Hbsewho Spoor EsDocument30 pagesHbsewho Spoor Esscribdfor7No ratings yet
- Disability Elective 1Document9 pagesDisability Elective 1thanhlongsdbNo ratings yet
- Social Work Methods and ToolsDocument50 pagesSocial Work Methods and ToolsfrancisgalorNo ratings yet
- Clientele and Audience in Social WorkDocument42 pagesClientele and Audience in Social WorkSTRAWBERRY CHEESE CAKENo ratings yet
- EnglishDocument22 pagesEnglishanshicaNo ratings yet
- BHR CH 2Document34 pagesBHR CH 2CHINMAYA NAYAKNo ratings yet
- Unit.5 Course Cde 672 by MunawarDocument20 pagesUnit.5 Course Cde 672 by MunawarAysh AliNo ratings yet
- General Equilibrium Welfare EconomicsDocument74 pagesGeneral Equilibrium Welfare EconomicsAbuzakir IdirisNo ratings yet
- PRICING FACTORS III Year AgEC 2024Document77 pagesPRICING FACTORS III Year AgEC 2024Abuzakir IdirisNo ratings yet
- Chapter 2 InclusivenessDocument20 pagesChapter 2 InclusivenessAbuzakir IdirisNo ratings yet
- Handout of Vegetable Crop Production and ManagementDocument40 pagesHandout of Vegetable Crop Production and ManagementAbuzakir IdirisNo ratings yet
- Micro II Chapter 1Document31 pagesMicro II Chapter 1Abuzakir IdirisNo ratings yet
- Filipino Identity and Moral StandardsDocument19 pagesFilipino Identity and Moral Standardsclarence33% (3)
- Human Resource ManagementDocument22 pagesHuman Resource ManagementRohit ChaudharyNo ratings yet
- The Reliability of A Child As An Eyewitness in CourtDocument4 pagesThe Reliability of A Child As An Eyewitness in CourttriptirathoreNo ratings yet
- Essay About HappinessDocument1 pageEssay About HappinessxioanaxNo ratings yet
- Consumer Behavior SyllabusDocument23 pagesConsumer Behavior SyllabusAhana BatabyalNo ratings yet
- NEW Micah Research Chapter 1 5Document52 pagesNEW Micah Research Chapter 1 5paulinemicahdelacruz15No ratings yet
- E-Book 3 Easy Steps To Turn Screen Time Into Academic Success (PhoneFreedom - Co)Document13 pagesE-Book 3 Easy Steps To Turn Screen Time Into Academic Success (PhoneFreedom - Co)Shahrukh2687No ratings yet
- A Passion Fo ExcellenceDocument22 pagesA Passion Fo ExcellenceDhwani_panickerNo ratings yet
- Video 3 GTK Team MotivationDocument2 pagesVideo 3 GTK Team MotivationfedorNo ratings yet
- Setting Boundaries WebDocument4 pagesSetting Boundaries WebInterfaith CarePartnersNo ratings yet
- Fe 2 Report - CaitlinDocument2 pagesFe 2 Report - Caitlinapi-438771871No ratings yet
- Directions: Each Item Below Contains A Question Followed by Suggested Responses. Select The One Best ResponseDocument7 pagesDirections: Each Item Below Contains A Question Followed by Suggested Responses. Select The One Best ResponseEsmareldah Henry SirueNo ratings yet
- Evaluating Effect of Anxiety On Eye Hand Coordination Using Jenga Game in Female Nursing Professionals An Observational StudyDocument6 pagesEvaluating Effect of Anxiety On Eye Hand Coordination Using Jenga Game in Female Nursing Professionals An Observational StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CH 7 Factors That Influence Communiction Draftv2Document44 pagesCH 7 Factors That Influence Communiction Draftv2Freddy Orlando MeloNo ratings yet
- Nur300 Final Paper 1Document6 pagesNur300 Final Paper 1api-570381186No ratings yet
- Module 2 Local NetworksDocument49 pagesModule 2 Local NetworksSarah SulitNo ratings yet
- Resume Carla Browning 072121Document2 pagesResume Carla Browning 072121api-558817903No ratings yet
- Table 5 SSRV Template Shell Mental Health Function Mild V4Document2 pagesTable 5 SSRV Template Shell Mental Health Function Mild V4fNo ratings yet
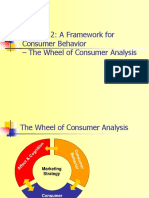
- Chapter 2: A Framework For Consumer Behavior - The Wheel of Consumer AnalysisDocument23 pagesChapter 2: A Framework For Consumer Behavior - The Wheel of Consumer AnalysisFlores GeraldNo ratings yet
- RRL FinalDocument6 pagesRRL FinalMaricel Palmes Encabo PalomilloNo ratings yet
- Unit 2 - Toward A Liberation PsychologyDocument4 pagesUnit 2 - Toward A Liberation PsychologyJoan FranciscoNo ratings yet
- Mental Health Services Awareness Night Where Can People Turn For Help?Document1 pageMental Health Services Awareness Night Where Can People Turn For Help?Hailey SpencerNo ratings yet
- Strategies in Teaching Mathematics Output TemplateDocument13 pagesStrategies in Teaching Mathematics Output TemplateGia RaldNo ratings yet
- Leadership StylesDocument8 pagesLeadership StylesSusan BvochoraNo ratings yet
- Short & Rinehart 1992-Conc Empoderamiento PDFDocument17 pagesShort & Rinehart 1992-Conc Empoderamiento PDFTF YhoanhyNo ratings yet
- Parenting in A Concrete Jungle - Guiding Principles and Action Plan - Year 10-13Document36 pagesParenting in A Concrete Jungle - Guiding Principles and Action Plan - Year 10-13NISTSecCounselingNo ratings yet
- 2 - Perception TheoryDocument34 pages2 - Perception Theoryswishrick1818No ratings yet