Download as pptx, pdf, or txt
You might also like
- 01 - Lineberry - Propulsion Fundamentals - 2019Document95 pages01 - Lineberry - Propulsion Fundamentals - 2019Николай СидоренкоNo ratings yet
- PacemakerDocument63 pagesPacemakerMonish RautNo ratings yet
- Temporary PacemakerDocument35 pagesTemporary Pacemakerromeorobin07No ratings yet
- PacemakerDocument48 pagesPacemakersoniya josephNo ratings yet
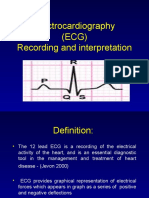
- Electrocardiography (ECG) Recording and InterpretationDocument59 pagesElectrocardiography (ECG) Recording and Interpretationkhushsandhu0% (1)
- P1 - The Particulate Nature of Matter PDFDocument17 pagesP1 - The Particulate Nature of Matter PDFEdgardo LeysaNo ratings yet
- Front View: Wire Rope DrumDocument2 pagesFront View: Wire Rope DrumDave Vendivil SambranoNo ratings yet
- PacemakersDocument69 pagesPacemakersdocjeevan89100% (1)
- PacemakerDocument24 pagesPacemakerLAWKUSH KUMARNo ratings yet
- Day 3 - APPEC 2021Document413 pagesDay 3 - APPEC 2021GaurieNo ratings yet
- Anaesthesia Management of Patient of PacemakerDocument92 pagesAnaesthesia Management of Patient of PacemakerSiva KrishnaNo ratings yet
- Introduction To Electrophysiology: What Are They DOING Over There?!Document51 pagesIntroduction To Electrophysiology: What Are They DOING Over There?!Mahendrakumar ManiNo ratings yet
- Cardiovascular Therapeutic ManagementDocument40 pagesCardiovascular Therapeutic ManagementjsksNo ratings yet
- CT Temporary PacemakersDocument61 pagesCT Temporary Pacemakersapi-229003912No ratings yet
- Cardiac Implantable Electronic DevicesDocument49 pagesCardiac Implantable Electronic DevicespriyathasanNo ratings yet
- MRI and CT Imaging With PacemakesDocument50 pagesMRI and CT Imaging With PacemakesDivyeshNo ratings yet
- Plante PacemakersDocument57 pagesPlante Pacemakersdragon66100% (1)
- Pacing NTI 2015Document35 pagesPacing NTI 2015wastionNo ratings yet
- Permanent Pacemaker: Supervisor: DR Pipin Ardhianto SPJP (K), FihaDocument67 pagesPermanent Pacemaker: Supervisor: DR Pipin Ardhianto SPJP (K), Fihapelantikan ppnirsdkNo ratings yet
- Pacemaker KGDocument61 pagesPacemaker KGSamip ThapaliyaNo ratings yet
- Unit IIIDocument44 pagesUnit IIIjadin45231No ratings yet
- Basics of Ecg InterpretationDocument76 pagesBasics of Ecg InterpretationDennis MiritiNo ratings yet
- Temporary Cardiac Pacing: Dr. Md. Mashiul Alam Phase B Resident Chairperson: Prof. F. RahmanDocument49 pagesTemporary Cardiac Pacing: Dr. Md. Mashiul Alam Phase B Resident Chairperson: Prof. F. RahmanvaishnaviNo ratings yet
- Arrhythmia Therapy: Henry Halperin, MD, MA, FAHA, FHRSDocument91 pagesArrhythmia Therapy: Henry Halperin, MD, MA, FAHA, FHRSRichard LiuNo ratings yet
- Care of Patient With TPM Slide PresentationDocument16 pagesCare of Patient With TPM Slide PresentationirzehronNo ratings yet
- Pacemaker Therapy: Prepared by Zahra A.M Ahmed Supervisor by Dr. Hassan Abdullah AthbiDocument27 pagesPacemaker Therapy: Prepared by Zahra A.M Ahmed Supervisor by Dr. Hassan Abdullah AthbiZahraa A.M AhmedNo ratings yet
- Cardiac PacingDocument89 pagesCardiac Pacingsandwhale056No ratings yet
- PacemakerDocument39 pagesPacemakerb7bkroroNo ratings yet
- N12 Cardiac DysrhythmiasDocument68 pagesN12 Cardiac Dysrhythmiaskathbondoc03No ratings yet
- IndicationsDocument3 pagesIndicationsAbubakr ElsediqqNo ratings yet
- Basic ECG Lecture - NewDocument148 pagesBasic ECG Lecture - NewAradhanaRamchandaniNo ratings yet
- PacemakersDocument38 pagesPacemakersrebebravoiniguez642No ratings yet
- Heart BlockDocument30 pagesHeart BlockM Farhad KhaniNo ratings yet
- Cardiac PeacemakerDocument19 pagesCardiac Peacemakerrana.said2018No ratings yet
- ECGDocument44 pagesECGJay ItaliyaNo ratings yet
- Mechanisme ArrhythmiaDocument38 pagesMechanisme ArrhythmiarskdemergencyNo ratings yet
- Pacemaker 180508042454Document86 pagesPacemaker 180508042454padmaNo ratings yet
- Pacemaker MalfunctionDocument23 pagesPacemaker MalfunctionsshansraNo ratings yet
- Pacemaker Therapy: Attila Kónyi M.D., PH.D Heart Institute University of PécsDocument42 pagesPacemaker Therapy: Attila Kónyi M.D., PH.D Heart Institute University of PécsIbrahim Kimymaru ZuzuranNo ratings yet
- Ventricular Arrhythmias EP Overview MedtronicDocument44 pagesVentricular Arrhythmias EP Overview Medtronicinu_upNo ratings yet
- TurpDocument99 pagesTurpakanksha singhNo ratings yet
- Ekg PsikDocument69 pagesEkg PsikZEISVA APRILIANINGRUMNo ratings yet
- Sinus Node Blocks DiagnosticDocument48 pagesSinus Node Blocks DiagnosticOlga GoryachevaNo ratings yet
- PacemakerDocument5 pagesPacemakerMuhammad Umer SaeedNo ratings yet
- Electro Cardiograph yDocument94 pagesElectro Cardiograph ykajonasfoodproductsNo ratings yet
- Cardiac Arrest: April B. Perez, RN, Man, PHD, FpchaDocument50 pagesCardiac Arrest: April B. Perez, RN, Man, PHD, Fpchayuuki konnoNo ratings yet
- Defibrillation and Electrical CardioversionDocument27 pagesDefibrillation and Electrical CardioversionYui Hirasawa100% (1)
- ECG Intro With Ref To QT Interval FinalDocument59 pagesECG Intro With Ref To QT Interval FinalGeorge VergheseNo ratings yet
- Rough Guide To Pacing 2009Document4 pagesRough Guide To Pacing 2009Ruba RizikNo ratings yet
- Defibrillation and Cardioversion: Dr. Asim BiswasDocument32 pagesDefibrillation and Cardioversion: Dr. Asim BiswasAsim Kumar BiswasNo ratings yet
- Cardiac MonitoringDocument138 pagesCardiac Monitoringanjanar26No ratings yet
- Medical Electronics Unit 3Document64 pagesMedical Electronics Unit 3TamilselvanNo ratings yet
- Pacemaker Invasive Cardiac PacingDocument57 pagesPacemaker Invasive Cardiac PacingAhmad Khalil Ahmad Al-SadiNo ratings yet
- Tomasz WikarekDocument95 pagesTomasz Wikareknamar13766No ratings yet
- Temporary Pacemakers-SICU's 101 PrimerDocument51 pagesTemporary Pacemakers-SICU's 101 Primerwaqas_xsNo ratings yet
- Ecg in ExDocument70 pagesEcg in ExLakshmi PrasannaNo ratings yet
- Curs Engl S Preexcit Corect Nic MPDocument72 pagesCurs Engl S Preexcit Corect Nic MPErland BordNo ratings yet
- Supraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, MysoreDocument81 pagesSupraventricular Arrhythmias: Dr. Arun Srinivas Chief Cardiologist Vikram Hospital, Mysorerobinjohn06No ratings yet
- Chapter 23 Management of Patients With Dysrhythmias and Conduction ProblemsDocument64 pagesChapter 23 Management of Patients With Dysrhythmias and Conduction Problemsسلطان محمد فوزي سلمانNo ratings yet
- Pacemaker: by Azaz KhanDocument76 pagesPacemaker: by Azaz KhanRitaLakhaniNo ratings yet
- DefibrillatorsDocument54 pagesDefibrillatorsAli Al-AhmedyNo ratings yet
- Pradheep ProjectDocument20 pagesPradheep ProjectHaribabuBabuNo ratings yet
- Sentiment Analysis With NLP Deep LearningDocument8 pagesSentiment Analysis With NLP Deep LearningAnkush ChajgotraNo ratings yet
- Phalogenics - Phalogenics Male Enhancement Reviews - Phalogenics Male Enhancement - Official Site !Document2 pagesPhalogenics - Phalogenics Male Enhancement Reviews - Phalogenics Male Enhancement - Official Site !Phalogenics Male EnhancementNo ratings yet
- Earth and Life ScienceDocument4 pagesEarth and Life SciencePinky PardilladaNo ratings yet
- Vertu Reader Instruction ManualDocument4 pagesVertu Reader Instruction ManualRodrigo PossariNo ratings yet
- Oral SummaryDocument3 pagesOral SummaryNatasha ParkNo ratings yet
- Price - The Fun Palace Cedric PriceDocument20 pagesPrice - The Fun Palace Cedric PricewhatsinausernameNo ratings yet
- Experiment N 5: Surface RoughnessDocument3 pagesExperiment N 5: Surface RoughnessG. Dancer GhNo ratings yet
- 10 MCQDocument40 pages10 MCQPragnesh Parmar0% (1)
- Ethical Theories: The Arthur W. Page Center Public Relations EthicsDocument7 pagesEthical Theories: The Arthur W. Page Center Public Relations EthicsBlessing FishNo ratings yet
- Stritt & Priebe Inc. Stritt & Priebe Inc. Stritt & Priebe Inc. Stritt & Priebe IncDocument1 pageStritt & Priebe Inc. Stritt & Priebe Inc. Stritt & Priebe Inc. Stritt & Priebe IncPeerunthorn WongcharoenchaichanaNo ratings yet
- 1VOCABDocument11 pages1VOCABmary anne malasagaNo ratings yet
- Chemical Recycling of Postconsumer Poly (Ethylene-Terephthalate) Bottles - Depolymerization StudyDocument8 pagesChemical Recycling of Postconsumer Poly (Ethylene-Terephthalate) Bottles - Depolymerization StudyKhaledAhmedNo ratings yet
- DGA Comparison Between Ester and Mineral Oils: C. Perrier, M. Marugan, M. Saravolac A. BeroualDocument4 pagesDGA Comparison Between Ester and Mineral Oils: C. Perrier, M. Marugan, M. Saravolac A. BeroualJhon Fredy Vallejo GiraldoNo ratings yet
- Mates Orals SyllabusDocument3 pagesMates Orals SyllabusmahmutNo ratings yet
- Gibberellins: Regulators of Plant HeightDocument17 pagesGibberellins: Regulators of Plant HeightPratiwi DwiNo ratings yet
- Compass NotesDocument55 pagesCompass NotesEngr XsadNo ratings yet
- Taboo Game 02Document6 pagesTaboo Game 02Sorin FluturNo ratings yet
- Abie Construction Limited: Retaining Wall Analysis (Bs 8002:1994)Document12 pagesAbie Construction Limited: Retaining Wall Analysis (Bs 8002:1994)Eric OwusuNo ratings yet
- Stepan Formulation 1201Document2 pagesStepan Formulation 1201Mohamed AdelNo ratings yet
- Three Phase Induction Motors: List of FormulaeDocument9 pagesThree Phase Induction Motors: List of FormulaekkkNo ratings yet
- Surface Area and VolumeDocument45 pagesSurface Area and Volumeapi-283229700No ratings yet
- Solar Hybrid Cold StorageDocument24 pagesSolar Hybrid Cold Storagerohan introNo ratings yet
- Latihan SoalDocument5 pagesLatihan SoalWizka Mulya JayaNo ratings yet
- High Altitude Aeronautical Platform Systems (Presentation)Document30 pagesHigh Altitude Aeronautical Platform Systems (Presentation)Mahenoor SiddiquiNo ratings yet
- LELO - TOR 3 - Online Manual - ENGDocument20 pagesLELO - TOR 3 - Online Manual - ENGebercueNo ratings yet
- l4 Control Survey TraverseDocument23 pagesl4 Control Survey TraverseSerinaaNo ratings yet
- Shell Rimula Oils: High Ash Level Oils For Diesel EnginesDocument2 pagesShell Rimula Oils: High Ash Level Oils For Diesel EnginesYeesvaran NarayanasamyNo ratings yet