Download as pptx, pdf, or txt
You might also like
- The International Journal of Periodontics & Restorative DentistryDocument8 pagesThe International Journal of Periodontics & Restorative DentistryjonvargasNo ratings yet
- Autoimmune HepatitisDocument3 pagesAutoimmune HepatitisMohammed FaragNo ratings yet
- Chronic Liver DiseaseDocument75 pagesChronic Liver DiseasebitspurNo ratings yet
- Autoimmune Hepatitis: Dr. Andi Nadya Febriama DR - DR Am - Lutfi Parewangi, SPPD KgehDocument25 pagesAutoimmune Hepatitis: Dr. Andi Nadya Febriama DR - DR Am - Lutfi Parewangi, SPPD KgehDeddy TrimarwantoNo ratings yet
- Allergy Immunology (3) (MedicalBooksVN - Com)Document9 pagesAllergy Immunology (3) (MedicalBooksVN - Com)malbertal1No ratings yet
- Overview of Autoimmune Hepatitis - UpToDateDocument33 pagesOverview of Autoimmune Hepatitis - UpToDatebagir_dm10No ratings yet
- Autoimmune Hepatitis: Ermias Kacha (MD)Document39 pagesAutoimmune Hepatitis: Ermias Kacha (MD)kachapaxxNo ratings yet
- Autoimmune Hepatitis LectureDocument21 pagesAutoimmune Hepatitis LectureAbdul hadiNo ratings yet
- Autoimmune Hepatitis FinalDocument44 pagesAutoimmune Hepatitis FinalritzbinNo ratings yet
- Hepatitis, Autoimmune - StatPearls - NCBI BookshelfDocument4 pagesHepatitis, Autoimmune - StatPearls - NCBI BookshelfMiguel RomeroNo ratings yet
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocument36 pagesATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Autoimmune HepatitisDocument41 pagesAutoimmune HepatitisMigi Pradysta100% (1)
- Hepatitis AutoimunDocument32 pagesHepatitis AutoimunRofi IrmanNo ratings yet
- Autoimmune Hepatitis. JPGN 2009Document7 pagesAutoimmune Hepatitis. JPGN 2009Carla CANo ratings yet
- Soluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesDocument11 pagesSoluble Liver Antigen/liver-Pancreas Antigen (anti-SLA/LP) AntibodiesShiela Montances100% (1)
- Aplastic AnemiaDocument6 pagesAplastic AnemiaLargactil CpzNo ratings yet
- Autoimmune Hepatitis: Diagnostic Criteria and Serological TestingDocument4 pagesAutoimmune Hepatitis: Diagnostic Criteria and Serological TestingHernan Del CarpioNo ratings yet
- Jurnal MalariaDocument2 pagesJurnal MalariadjebrutNo ratings yet
- Acute PancreatitisDocument11 pagesAcute Pancreatitispeter_soósNo ratings yet
- 3讲义hematologyDocument96 pages3讲义hematologychongyu888xiongNo ratings yet
- College of Medicine: Thi Qar UniversityDocument30 pagesCollege of Medicine: Thi Qar Universityhussain AltaherNo ratings yet
- Acute Pancreatitis: Clinical PR ActiceDocument9 pagesAcute Pancreatitis: Clinical PR ActicesanthiagoschneiderNo ratings yet
- Celiac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcDocument59 pagesCeliac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcAjeet LohanaNo ratings yet
- 13 Acute CholangitisDocument3 pages13 Acute Cholangitischarmainemargaret.parreno.medNo ratings yet
- 25-Year-Old Woman With Anemia: Ranjini R. Roy, MD, and Matthew R. Thomas, MDDocument4 pages25-Year-Old Woman With Anemia: Ranjini R. Roy, MD, and Matthew R. Thomas, MDFredy CorreaNo ratings yet
- Cytomegalovirus Triggering Autoimmune Hepatitis: Case Report and Literature ReviewDocument3 pagesCytomegalovirus Triggering Autoimmune Hepatitis: Case Report and Literature ReviewRabiatul 'raney' AdawiyahNo ratings yet
- Perspectives in Clinical Hepatology Current and Novel Immunosuppressive Therapy For Autoimmune HepatitisDocument7 pagesPerspectives in Clinical Hepatology Current and Novel Immunosuppressive Therapy For Autoimmune HepatitisPathrecia Natalia SiagianNo ratings yet
- Pediatric Systemic Lupus Erythematosus Associated With AutoimmuneDocument9 pagesPediatric Systemic Lupus Erythematosus Associated With AutoimmunegistaluvikaNo ratings yet
- Nejmcps 1808494Document6 pagesNejmcps 1808494dias100% (1)
- Autoimmune Hepatitis: Mu ViDocument68 pagesAutoimmune Hepatitis: Mu VidrsajusvNo ratings yet
- A Laboratory Diagnostic Approach To Hepatobiliary Disease in Small AnimalsDocument17 pagesA Laboratory Diagnostic Approach To Hepatobiliary Disease in Small Animalsl.fernandagonzalez97No ratings yet
- Cross Edit Neuro CelDocument3 pagesCross Edit Neuro CelMihaela MtnNo ratings yet
- Interactive Clinical Module 7ADocument13 pagesInteractive Clinical Module 7AKenedila MatetaNo ratings yet
- Kuliah Autoimune in Liver Disease 24 Agustus 2019Document40 pagesKuliah Autoimune in Liver Disease 24 Agustus 2019juslan kasmarNo ratings yet
- Immunology and Autoimmunity: IncreasedDocument6 pagesImmunology and Autoimmunity: IncreasedimperiouxxNo ratings yet
- Jaundice As A Presentation of Thyrotoxic CrisisDocument3 pagesJaundice As A Presentation of Thyrotoxic CrisisRizki AmeliaNo ratings yet
- Autoinmune LaboratorioDocument9 pagesAutoinmune LaboratorioJacob DavisNo ratings yet
- Frequency of Celiac Disease in PatientsDocument6 pagesFrequency of Celiac Disease in PatientsHantiukNo ratings yet
- 37 Aup EtalDocument8 pages37 Aup EtaleditorijmrhsNo ratings yet
- Case ReportDocument5 pagesCase ReportAlfi YatunNo ratings yet
- Renal Transplantation An OverviewDocument58 pagesRenal Transplantation An OverviewSony's TechNo ratings yet
- Autoimmune Hepatitis - Primary Biliary Cirrhosis Overlap SyndromeDocument3 pagesAutoimmune Hepatitis - Primary Biliary Cirrhosis Overlap Syndromesusanto kusumaNo ratings yet
- Abnormal Liver Function Test LGHDocument35 pagesAbnormal Liver Function Test LGHElaineNo ratings yet
- Enfermedades HepatobiliaresDocument4 pagesEnfermedades HepatobiliaresDennis J RiosNo ratings yet
- Hepatitis AutoinmuneDocument7 pagesHepatitis AutoinmuneGERALDINE JARAMILLO VARGASNo ratings yet
- Surgery - General SurgeryDocument58 pagesSurgery - General Surgeryteena6506763100% (1)
- Autoimmune Hepatitis: Robert G. Gish MDDocument53 pagesAutoimmune Hepatitis: Robert G. Gish MDRobert G. Gish, MD100% (1)
- Autoimmune HepatitisDocument13 pagesAutoimmune HepatitisVita Delfi YantiNo ratings yet
- knh411 Celiac DiseaseDocument11 pagesknh411 Celiac Diseaseapi-301897220100% (1)
- Acute Pancearitis PDFDocument15 pagesAcute Pancearitis PDFalmandoNo ratings yet
- Kole StasisDocument16 pagesKole StasisAlia SalviraNo ratings yet
- Cytochrome P450 2E1 Genotype and The Sus PDFDocument7 pagesCytochrome P450 2E1 Genotype and The Sus PDFAbhinav AggarwalNo ratings yet
- De Novo Aih After LT GuidoDocument11 pagesDe Novo Aih After LT GuidoEmma SaelensNo ratings yet
- DX TX HAIDocument23 pagesDX TX HAIJair Alexander Quintero PanucoNo ratings yet
- Liver Disease in Alpha-1 Antitrypsin Deficiency: Current Approaches and Future DirectionsDocument10 pagesLiver Disease in Alpha-1 Antitrypsin Deficiency: Current Approaches and Future DirectionsEianni Patrice De JoseNo ratings yet
- Celiac Disease: Clinical PracticeDocument8 pagesCeliac Disease: Clinical PracticeRo RojasNo ratings yet
- Adil Abood: Lec. 7 Gastrointestinal and Liver Diseases Gluten-Sensitive EnteropathyDocument6 pagesAdil Abood: Lec. 7 Gastrointestinal and Liver Diseases Gluten-Sensitive Enteropathyrania rNo ratings yet
- Amyloidosis PDFDocument8 pagesAmyloidosis PDFKarthik KoneruNo ratings yet
- Autoimmune Hepatitis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandAutoimmune Hepatitis, A Simple Guide To The Condition, Treatment And Related DiseasesRating: 5 out of 5 stars5/5 (1)
- Complementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderFrom EverandComplementary and Alternative Medical Lab Testing Part 6: Liver and GallbladderNo ratings yet
- Diagnosis and Management of Autoimmune Hepatitis: A Clinical GuideFrom EverandDiagnosis and Management of Autoimmune Hepatitis: A Clinical GuideMark W. RussoNo ratings yet
- MycologyDocument6 pagesMycologyAhmed AliNo ratings yet
- Fendo 12 701263Document10 pagesFendo 12 701263Ahmed AliNo ratings yet
- 5 - Beta Thalassemia SyndromesDocument9 pages5 - Beta Thalassemia SyndromesAhmed AliNo ratings yet
- KT 640Document4 pagesKT 640Ahmed AliNo ratings yet
- Febrile Antigens Package InsertDocument2 pagesFebrile Antigens Package InsertAhmed AliNo ratings yet
- Open Book Exam - Renal Dz. 2019Document2 pagesOpen Book Exam - Renal Dz. 2019Ahmed AliNo ratings yet
- SI Units For Clinical DataDocument6 pagesSI Units For Clinical DataAhmed AliNo ratings yet
- Si UnitsDocument8 pagesSi UnitsAhmed AliNo ratings yet
- GC-AASGasChromatography-AtomicAbsorptionspectrometry Advancedspectralanalysis MPHARMACYMPCTDocument9 pagesGC-AASGasChromatography-AtomicAbsorptionspectrometry Advancedspectralanalysis MPHARMACYMPCTAhmed AliNo ratings yet
- Z481upi 03Document2 pagesZ481upi 03Ahmed AliNo ratings yet
- Package-Insert-Reagent-Red-Blood-Cells-IH-Cell-I-II-III-IH-Cell I-II-IH-Cell-PoolDocument7 pagesPackage-Insert-Reagent-Red-Blood-Cells-IH-Cell-I-II-III-IH-Cell I-II-IH-Cell-PoolAhmed AliNo ratings yet
- Cortisol ELISA Kit: Item No. 500360Document21 pagesCortisol ELISA Kit: Item No. 500360Ahmed AliNo ratings yet
- ABIN6975603 ManualDocument12 pagesABIN6975603 ManualAhmed AliNo ratings yet
- Package Insert - Biotestcell A1 & B and Biotestcell A2 - 0Document2 pagesPackage Insert - Biotestcell A1 & B and Biotestcell A2 - 0Ahmed AliNo ratings yet
- 12 2014 JHOP - SympManDocument4 pages12 2014 JHOP - SympManAhmed AliNo ratings yet
- Matrix AHG (Coombs) Test Card QRGDocument1 pageMatrix AHG (Coombs) Test Card QRGAhmed AliNo ratings yet
- 0740 X 1Document1 page0740 X 1Ahmed AliNo ratings yet
- 186 FullDocument13 pages186 FullAhmed AliNo ratings yet
- 174-Potential Interaction Between Nefopam and Tramadol - RedactedDocument11 pages174-Potential Interaction Between Nefopam and Tramadol - RedactedAhmed AliNo ratings yet
- Cardiolipin Ab Igg/Igm Elisa: Product InformationDocument12 pagesCardiolipin Ab Igg/Igm Elisa: Product InformationAhmed AliNo ratings yet
- Name NameDocument1 pageName NameAhmed AliNo ratings yet
- IB05018Document15 pagesIB05018Ahmed AliNo ratings yet
- Brucella-V9-E - USDocument17 pagesBrucella-V9-E - USAhmed AliNo ratings yet
- Yadirgi2017Immuno detectionofcleavedSNAP 25fromdifferentiationmouseembryonicstemcellsprovidesasensitiveassayfordeterminationofbotulinumatoxinandantitoxinpotencyDocument11 pagesYadirgi2017Immuno detectionofcleavedSNAP 25fromdifferentiationmouseembryonicstemcellsprovidesasensitiveassayfordeterminationofbotulinumatoxinandantitoxinpotencyAhmed AliNo ratings yet
- Trematodes: SchistosomaiasisDocument5 pagesTrematodes: SchistosomaiasisAhmed AliNo ratings yet
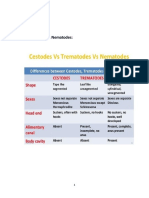
- Parasitology:: Helminthes: Platyhelminthes & NematodesDocument8 pagesParasitology:: Helminthes: Platyhelminthes & NematodesAhmed AliNo ratings yet
- Comparison of Gel Column, Card, Cartridge, Slide and Tube Techniques For AB Blood Typing of CatsDocument15 pagesComparison of Gel Column, Card, Cartridge, Slide and Tube Techniques For AB Blood Typing of CatsAhmed AliNo ratings yet
- Se 120151 BulDocument3 pagesSe 120151 BulAhmed AliNo ratings yet
- Blood Banking Procedures Notes Final PDFDocument7 pagesBlood Banking Procedures Notes Final PDFAhmed AliNo ratings yet
- Trematodes: SchistosomaiasisDocument8 pagesTrematodes: SchistosomaiasisAhmed AliNo ratings yet
- Combination PsychotherapyDocument37 pagesCombination PsychotherapyElija MansonNo ratings yet
- Diabetes InsipidusDocument10 pagesDiabetes InsipidussoniaNo ratings yet
- Chapter 8 and 9 Slides (Part 2) Bipolar Mood Disorders 2023Document24 pagesChapter 8 and 9 Slides (Part 2) Bipolar Mood Disorders 2023Phoebe LauNo ratings yet
- NCM 117 - Psychiatric Nursing (MODULE 4)Document7 pagesNCM 117 - Psychiatric Nursing (MODULE 4)Meryville JacildoNo ratings yet
- Gingival and Periodontal Diseases in Children and AdolescentsDocument4 pagesGingival and Periodontal Diseases in Children and AdolescentsYuniarPratiwyPanjaitanNo ratings yet
- Usmle ExamDocument13 pagesUsmle ExamAmal Alameen67% (3)
- Week1 - NAILCARE (Sek)Document2 pagesWeek1 - NAILCARE (Sek)rhyzeneNo ratings yet
- NCM112 RSHF LSHF DD SDDocument3 pagesNCM112 RSHF LSHF DD SDKryffa DegayNo ratings yet
- Question Text Question Type PointsDocument25 pagesQuestion Text Question Type PointsMagda Tvildiani100% (1)
- Veterinary Diagnostics TechniquesDocument5 pagesVeterinary Diagnostics Techniquesmarcus ciceroNo ratings yet
- Order 26634Document7 pagesOrder 26634Best EssaysNo ratings yet
- PneumoniaDocument12 pagesPneumoniaadolfrc9200No ratings yet
- 3 CFTDocument9 pages3 CFTMunir AhmedNo ratings yet
- Bhopal CGHS Rate List 2014Document84 pagesBhopal CGHS Rate List 2014EsolNo ratings yet
- MD3 Peer TutoringDocument3 pagesMD3 Peer Tutoringdragtoss2No ratings yet
- SA Psych MAY 2016 FIn Final WebDocument82 pagesSA Psych MAY 2016 FIn Final WebAKNTAI002No ratings yet
- MS1 Summer Opportunities ListDocument6 pagesMS1 Summer Opportunities Listimaina17No ratings yet
- Preparation Support Pack 180515Document69 pagesPreparation Support Pack 180515sinbad200No ratings yet
- Pracetamol Guaifene Fenilefrina DiaDocument13 pagesPracetamol Guaifene Fenilefrina DiaFranklin Basurco MaqueraNo ratings yet
- Roux 2015Document5 pagesRoux 2015ocramusNo ratings yet
- ICHROMA IgG-IgMDocument5 pagesICHROMA IgG-IgMAlfonso RamosNo ratings yet
- Lumbar Facet Syndrome - BogdukDocument8 pagesLumbar Facet Syndrome - BogdukSamSchroetkeNo ratings yet
- Corynebacterium Diphtheriae Listeria Monocytogenes Erysipelothrix Rhusopathiae Lactobacillus Spp. Streptomycetes Spp. Nocardia SPPDocument1 pageCorynebacterium Diphtheriae Listeria Monocytogenes Erysipelothrix Rhusopathiae Lactobacillus Spp. Streptomycetes Spp. Nocardia SPPAbcd ReyesNo ratings yet
- Stable Pasca Resusitasi TransportDocument76 pagesStable Pasca Resusitasi TransportDian KusumaNo ratings yet
- Technical Skills ChecklistDocument4 pagesTechnical Skills Checklistctissot03No ratings yet
- Anorexia & Lethargy in A Dog With Presumed GiardiasisDocument4 pagesAnorexia & Lethargy in A Dog With Presumed GiardiasisMiruna ChiriacNo ratings yet
- Vaccine IngredientsDocument4 pagesVaccine IngredientsJulie BinghamNo ratings yet
- Chapter 6-Clove Oil (Eugenol)Document47 pagesChapter 6-Clove Oil (Eugenol)jimmyboy111No ratings yet
- Integrated Management of Neonatal & Childhood Illness (Imnci)Document5 pagesIntegrated Management of Neonatal & Childhood Illness (Imnci)J Ta RaNo ratings yet