Download as pptx, pdf, or txt
You might also like
- Research Paper OutlineDocument3 pagesResearch Paper OutlineShateanu' Bryant100% (1)
- Choose 2 From The Disease Below That Are Emerging in The PhilippinesDocument4 pagesChoose 2 From The Disease Below That Are Emerging in The PhilippinesMICHELLE BIANCA PATRICE CRUZNo ratings yet
- AMC Clinicals Tips and TricksDocument11 pagesAMC Clinicals Tips and TricksNayantara Nair100% (1)
- Diseases of PulpDocument81 pagesDiseases of PulpDrMohit Sharma100% (1)
- Biology Lab - Effect of ExerciseDocument3 pagesBiology Lab - Effect of Exerciseiamsotired19100% (6)
- Case Report - Complete Denture - 2Document4 pagesCase Report - Complete Denture - 2Astri Ggamjong Xiao LuNo ratings yet
- 3 Drugs Acting On The GITDocument50 pages3 Drugs Acting On The GITDagnachew kasayeNo ratings yet
- DR - Husam Git 2023Document19 pagesDR - Husam Git 2023ManWol JangNo ratings yet
- Ulcer Gastrointestinal TractDocument6 pagesUlcer Gastrointestinal TractHossam ArafaNo ratings yet
- Peptic Ulcer Healing Drugs 140420Document50 pagesPeptic Ulcer Healing Drugs 140420Tehreem NadeemNo ratings yet
- Peptic UlcerDocument48 pagesPeptic Ulcerscribd225No ratings yet
- Gi PharmacologyDocument54 pagesGi Pharmacologyyohanes fikaduNo ratings yet
- Pharmacology SGL 1 Drugs Used To Treat Acid Related Disorders DRDocument32 pagesPharmacology SGL 1 Drugs Used To Treat Acid Related Disorders DRgabi.g.wahbeNo ratings yet
- GIT Part 1Document21 pagesGIT Part 1jjf4708No ratings yet
- Drugs For Peptic UlcerDocument11 pagesDrugs For Peptic UlcerAdhithiayan ANo ratings yet
- 21 - Gastrointestinal PharmacologyDocument53 pages21 - Gastrointestinal PharmacologySuhayb CumarNo ratings yet
- 14-Drugs Use For GIT Disorders DentistryDocument4 pages14-Drugs Use For GIT Disorders DentistryLegendary 099No ratings yet
- Anti Ulcer AgentsDocument37 pagesAnti Ulcer AgentsKakai Ablanque LopozNo ratings yet
- Pharmcology IiDocument99 pagesPharmcology IiSalahadinNo ratings yet
- GIT - Part IIDocument23 pagesGIT - Part IIDiyar ArifNo ratings yet
- Pharmacology of Antiulcer DrugsDocument44 pagesPharmacology of Antiulcer DrugsSita mahalakshmi VakkapatlaNo ratings yet
- Antasida, Ah2, SitoprotektorDocument48 pagesAntasida, Ah2, SitoprotektorYulia KasihNo ratings yet
- Gi PharmacologyDocument13 pagesGi PharmacologyyeshiwasdagnewNo ratings yet
- Chapter 4 GI DrugsDocument45 pagesChapter 4 GI DrugsKIDUS YAREDNo ratings yet
- Pharmacotherapy of Gastric Acidity, Peptic UlcersDocument19 pagesPharmacotherapy of Gastric Acidity, Peptic UlcersZaid Al-KadhimiNo ratings yet
- Antacids H Antagonists Proton Pump InhibitorsDocument49 pagesAntacids H Antagonists Proton Pump Inhibitorsmelvingodric_arceNo ratings yet
- (GIT Pharm3) Mucosal Protecting Agents (13th September 2023)Document21 pages(GIT Pharm3) Mucosal Protecting Agents (13th September 2023)Muhammad TararNo ratings yet
- L-3 GIT Diseases and DrugsDocument20 pagesL-3 GIT Diseases and DrugsRafi AhmedNo ratings yet
- Gastrointestinal Drugs: Dr. Nandit P BDocument34 pagesGastrointestinal Drugs: Dr. Nandit P BNandit BanawalikarNo ratings yet
- 13.drugs For GI - Part IDocument38 pages13.drugs For GI - Part ILee BoborasNo ratings yet
- 13 Antacids and Controllers UpdDocument63 pages13 Antacids and Controllers Updone_nd_onlyuNo ratings yet
- Pharmacotherapy of Peptic UlcerDocument18 pagesPharmacotherapy of Peptic Ulceromar khanNo ratings yet
- Antiulcer Chapter 40Document9 pagesAntiulcer Chapter 40triddle1969No ratings yet
- Digestive System PharmacologyDocument57 pagesDigestive System PharmacologyAbdallah AshrafNo ratings yet
- GIT PharmacologyDocument57 pagesGIT PharmacologyCarlous Shuga ChadwickNo ratings yet
- Asd Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsDocument4 pagesAsd Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsZaky Faris MaulanaNo ratings yet
- Asc Asd Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsDocument4 pagesAsc Asd Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsZaky Faris MaulanaNo ratings yet
- SekeripDocument4 pagesSekeripZaky Faris MaulanaNo ratings yet
- Christine Drug StudyDocument4 pagesChristine Drug StudyAmari BillNo ratings yet
- Sldkjfs DKJF SDocument4 pagesSldkjfs DKJF SZaky Faris MaulanaNo ratings yet
- FarmakoDocument4 pagesFarmakoZaky Faris MaulanaNo ratings yet
- Sldkjfs DKJF SDocument4 pagesSldkjfs DKJF SZaky Faris MaulanaNo ratings yet
- Sldkjfs DKJF SDocument4 pagesSldkjfs DKJF SZaky Faris MaulanaNo ratings yet
- Asdasdasdaaaaaasdaascasasascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsDocument4 pagesAsdasdasdaaaaaasdaascasasascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsZaky Faris MaulanaNo ratings yet
- Asd Asc Asd Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsDocument4 pagesAsd Asc Asd Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsZaky Faris MaulanaNo ratings yet
- FarmakoDocument4 pagesFarmakoZaky Faris MaulanaNo ratings yet
- SekeripDocument4 pagesSekeripZaky Faris MaulanaNo ratings yet
- Asdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsDocument4 pagesAsdasdasd Ojahsk Chajshdkjah Sjda Asda Asca HGHJ GHGMJ AntacidsZaky Faris MaulanaNo ratings yet
- SekeripDocument4 pagesSekeripZaky Faris MaulanaNo ratings yet
- DF GHXDFH Cgnasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asd AntacidsDocument4 pagesDF GHXDFH Cgnasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asd AntacidsZaky Faris MaulanaNo ratings yet
- Aaaaaasdaascasasascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsDocument4 pagesAaaaaasdaascasasascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsZaky Faris MaulanaNo ratings yet
- Treatment of Peptic UlcerDocument27 pagesTreatment of Peptic Ulcerapi-3761895100% (3)
- SekeripDocument4 pagesSekeripZaky Faris MaulanaNo ratings yet
- JH GVJHVMJH VMJ, Asasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asd AntacidsDocument4 pagesJH GVJHVMJH VMJ, Asasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asd AntacidsZaky Faris MaulanaNo ratings yet
- SekeripDocument4 pagesSekeripZaky Faris MaulanaNo ratings yet
- FarmakoDocument4 pagesFarmakoZaky Faris MaulanaNo ratings yet
- Asasascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsDocument4 pagesAsasascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsZaky Faris MaulanaNo ratings yet
- Ascascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsDocument4 pagesAscascdhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asdj, Gsayratjdydutd AntacidsZaky Faris MaulanaNo ratings yet
- Dhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asd AntacidsDocument4 pagesDhkgfrqeulkgfhiowqgasasaa SK Nla SN KN Aslk La S Al JH Lash Lanlksbaasd Asd AntacidsZaky Faris MaulanaNo ratings yet
- SekeripDocument4 pagesSekeripZaky Faris MaulanaNo ratings yet
- RWHWHWDocument4 pagesRWHWHWZaky Faris MaulanaNo ratings yet
- Sldkjfs DKJF SDocument4 pagesSldkjfs DKJF SZaky Faris MaulanaNo ratings yet
- Pharmacotherapy of Peptic Ulcer: DR ZareenDocument50 pagesPharmacotherapy of Peptic Ulcer: DR ZareenGareth BaleNo ratings yet
- Pharmacotherapy of Peptic Ulcer: DR ZareenDocument50 pagesPharmacotherapy of Peptic Ulcer: DR ZareenGareth BaleNo ratings yet
- Basic Pharmacology And Drug Calculations [Practice Questions And Answers]From EverandBasic Pharmacology And Drug Calculations [Practice Questions And Answers]Rating: 4 out of 5 stars4/5 (1)
- Resume Esmaeil ImaniDocument2 pagesResume Esmaeil ImaniSepideh MirzaeiNo ratings yet
- Navdeep Madheshiya Report - 2022-01-15t183422.725Document1 pageNavdeep Madheshiya Report - 2022-01-15t183422.725navdeep madheshiyaNo ratings yet
- Exercise12 PDFDocument17 pagesExercise12 PDFHayna RoseNo ratings yet
- Orofacial Complications of Non Surgical Cancer TherapyDocument59 pagesOrofacial Complications of Non Surgical Cancer TherapyKassim OboghenaNo ratings yet
- Choose The Correct Answer?: A-Cloven Hooved AnmalsDocument17 pagesChoose The Correct Answer?: A-Cloven Hooved AnmalsAhmed El MorsyNo ratings yet
- Gen Med Revision PDF 5Document107 pagesGen Med Revision PDF 5sharen100% (3)
- Laerdal Infant Airway Management TrainerDocument7 pagesLaerdal Infant Airway Management TrainerConrad WaluddeNo ratings yet
- PHYS THER-2006-Jette-726-34Document11 pagesPHYS THER-2006-Jette-726-34Mariana HernandezNo ratings yet
- Benefits of Vitamin E NotesDocument9 pagesBenefits of Vitamin E NotesAsdar DaraNo ratings yet
- NSG 506 - Cmo 10 Series 1998Document69 pagesNSG 506 - Cmo 10 Series 1998mvfigueroaNo ratings yet
- 1129 - Health and Wellbeing - tcm143-663582Document4 pages1129 - Health and Wellbeing - tcm143-663582Eugen CrivceanschiNo ratings yet
- Copy of EnterobiasisDocument1 pageCopy of EnterobiasisCelina GonzalesNo ratings yet
- For Private Circulation OnlyDocument40 pagesFor Private Circulation OnlyDOMINIC EDUAHNo ratings yet
- PCV 13Document2 pagesPCV 13api-237098034No ratings yet
- Awareness of Risk Factors and Warning Symptoms of Stroke in General Population JournalDocument13 pagesAwareness of Risk Factors and Warning Symptoms of Stroke in General Population JournalaryaNo ratings yet
- Oxygen Delivery and Consumption - UpToDateDocument15 pagesOxygen Delivery and Consumption - UpToDateValerie ZimmermannNo ratings yet
- Final Resume 1Document3 pagesFinal Resume 1api-430931351No ratings yet
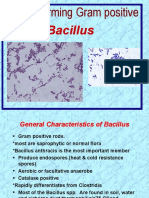
- Bacillus: Spore-Forming Gram PositiveDocument24 pagesBacillus: Spore-Forming Gram Positiveعلي عبد الكريم عاصيNo ratings yet
- Moh ExamsDocument12 pagesMoh ExamsYusuf SiddiquiNo ratings yet
- Systemic Lupus ErythematosusDocument40 pagesSystemic Lupus ErythematosusAkshan SentinelNo ratings yet
- CH 21Document19 pagesCH 21Lisa Evitt CoxNo ratings yet
- Pap SmearDocument75 pagesPap SmearRaine BowNo ratings yet
- Ahmed Et Al IAA Journal of Biological Sciences 8 (1) :228-238,2022. ISSN: 2636-7254 ©iaajournalsDocument11 pagesAhmed Et Al IAA Journal of Biological Sciences 8 (1) :228-238,2022. ISSN: 2636-7254 ©iaajournalsKIU PUBLICATION AND EXTENSIONNo ratings yet
































































![Basic Pharmacology And Drug Calculations [Practice Questions And Answers]](https://imgv2-1-f.scribdassets.com/img/word_document/475660044/149x198/2c7fc45015/1691161640?v=1)