Download as pptx, pdf, or txt
You might also like
- Example Semen Analysis ReportDocument2 pagesExample Semen Analysis Reportcupi76790% (20)
- Adult Infectious Disease Bulletpoints HandbookFrom EverandAdult Infectious Disease Bulletpoints HandbookRating: 4.5 out of 5 stars4.5/5 (9)
- Posi CaineDocument2 pagesPosi CaineArss Muhammad Budi PNo ratings yet
- Clinical Practice Guidelines Burns Physiotherapy and Occupational TherapyDocument34 pagesClinical Practice Guidelines Burns Physiotherapy and Occupational Therapyfauziafahmi95100% (2)
- NCCN CNS Guidelines Version 3.2019 PDFDocument163 pagesNCCN CNS Guidelines Version 3.2019 PDFzefri suhendarNo ratings yet
- Afib For JCU 2Document33 pagesAfib For JCU 2Sofia KusumadewiNo ratings yet
- Recognition and Management of Toxicities: Faculty BiographyDocument35 pagesRecognition and Management of Toxicities: Faculty BiographyDaniela SerbanNo ratings yet
- Ablation Pédiatrique Alice MaltretDocument36 pagesAblation Pédiatrique Alice Maltretmihalcea alinNo ratings yet
- CASTLE SubanalysisDocument4 pagesCASTLE SubanalysisIsmaelJoséGonzálezGuzmánNo ratings yet
- Fosap PedDocument17 pagesFosap PedIndranil GhoshNo ratings yet
- COVID 19 Vaccine Comparison ChartDocument2 pagesCOVID 19 Vaccine Comparison ChartNuklear AdiwenaNo ratings yet
- CCO Hematology 2022 619Document11 pagesCCO Hematology 2022 619habibe koçNo ratings yet
- ARTEMIS: First-Line Darunavir/Ritonavir Effective and Well Tolerated Irrespective of Sex, Age, or RaceDocument5 pagesARTEMIS: First-Line Darunavir/Ritonavir Effective and Well Tolerated Irrespective of Sex, Age, or RaceIsmaelJoséGonzálezGuzmánNo ratings yet
- 1 - Hodgkin's LymphomaDocument12 pages1 - Hodgkin's LymphomaDiana MitreaNo ratings yet
- Atrial Fibrillation: EpidemiologyDocument3 pagesAtrial Fibrillation: Epidemiologydacc1337No ratings yet
- Antibody Response To Mrna Sars-Cov-2 Vaccine Among Dialysis Patients-A Prospective Cohort StudyDocument3 pagesAntibody Response To Mrna Sars-Cov-2 Vaccine Among Dialysis Patients-A Prospective Cohort StudyBala MuraliNo ratings yet
- CCO 2014 AASLD Satellite DownloadableDocument43 pagesCCO 2014 AASLD Satellite DownloadableAnonymous dkH3NSvhvANo ratings yet
- CvotDocument29 pagesCvotakash kondapalliNo ratings yet
- Targeted Therapies in Hematology & Oncology: Mark B Juckett MD Section of Hematology/BMT University of WisconsinDocument61 pagesTargeted Therapies in Hematology & Oncology: Mark B Juckett MD Section of Hematology/BMT University of WisconsinihdaNo ratings yet
- YA CCO - IO - in - Urothelial - Cancer - Downloadable - 1Document27 pagesYA CCO - IO - in - Urothelial - Cancer - Downloadable - 1Yasar HammorNo ratings yet
- WP Contentuploads201805CABANA Trial Slides 05092018FINAL PDFDocument19 pagesWP Contentuploads201805CABANA Trial Slides 05092018FINAL PDFJjawo GinesNo ratings yet
- Study On Prevalence of Subclinical Hypothyroidism Inelderlyagegroup and Its Relation With Diabetes, Hypertension and Ischemic Heart DiseaseDocument4 pagesStudy On Prevalence of Subclinical Hypothyroidism Inelderlyagegroup and Its Relation With Diabetes, Hypertension and Ischemic Heart DiseaseIJAR JOURNALNo ratings yet
- AA BloodDocument10 pagesAA BloodsilviaNo ratings yet
- CCO AU 2016 HCV Plenary 1 SlidesDocument39 pagesCCO AU 2016 HCV Plenary 1 SlideshziglamNo ratings yet
- Debora Shinta Liana, Andi Cahyadi, Maria Christina Shanty Larasati, Mia Ratwita AndarsiniDocument1 pageDebora Shinta Liana, Andi Cahyadi, Maria Christina Shanty Larasati, Mia Ratwita AndarsiniBill Brenton Raynherzh MandalaNo ratings yet
- Conference PresentationDocument19 pagesConference PresentationJamil Muqtadir BhattiNo ratings yet
- Challenges in Managing Hepatitis C Virus InfectionDocument57 pagesChallenges in Managing Hepatitis C Virus InfectionAhmed ElwassiefNo ratings yet
- Similar Efficacy Demonstrated in HIV With Lopinavir QD or BIDDocument5 pagesSimilar Efficacy Demonstrated in HIV With Lopinavir QD or BIDIsmaelJoséGonzálezGuzmánNo ratings yet
- Characteristic All Patients Saline Streptokinase P Value: Table 1. Baseline Characteristics of Patients and EffusionsDocument1 pageCharacteristic All Patients Saline Streptokinase P Value: Table 1. Baseline Characteristics of Patients and EffusionsmarkNo ratings yet
- Dr. Saut Nababan, SP - PD, PH.D: Riwayat PendidikanDocument20 pagesDr. Saut Nababan, SP - PD, PH.D: Riwayat PendidikanRini WidyantariNo ratings yet
- AF (CHADSVASC-HASbled)Document1 pageAF (CHADSVASC-HASbled)Giorgi NanetashviliNo ratings yet
- AW Diag Treat AR FinalDocument28 pagesAW Diag Treat AR FinalAnna DangNo ratings yet
- International Journal of Chemtech Research: Ade Andriany, Refli Hasan, Zainal Safri, Savita HandayaniDocument8 pagesInternational Journal of Chemtech Research: Ade Andriany, Refli Hasan, Zainal Safri, Savita HandayaniHeni PuspitasariNo ratings yet
- Supplementary AppendixDocument4 pagesSupplementary AppendixMary Joyce PlacidoNo ratings yet
- Karakteristik Faktor Siklus MenstruasiDocument7 pagesKarakteristik Faktor Siklus MenstruasiMerry NildaweniNo ratings yet
- ESMO 2016 - Abstract 719ODocument17 pagesESMO 2016 - Abstract 719ODavid OlmosNo ratings yet
- Dupilumab CSUDocument3 pagesDupilumab CSUnoviadewaniNo ratings yet
- Anticoagulation in Atrial FibrillationDocument22 pagesAnticoagulation in Atrial FibrillationprobowurNo ratings yet
- CCO 2020 WCLC Downloadable 1Document106 pagesCCO 2020 WCLC Downloadable 1Florencia GuerraNo ratings yet
- 2 HCV Pangenotipe SOHO 2021 Dr. FardahDocument30 pages2 HCV Pangenotipe SOHO 2021 Dr. FardahAnnisa Oktoviani MursidaNo ratings yet
- Actg 5353Document5 pagesActg 5353nacxit6No ratings yet
- If HP Cancer Guide BMT ManualDocument363 pagesIf HP Cancer Guide BMT ManualZardar KNo ratings yet
- RAVEL 4 AnosDocument13 pagesRAVEL 4 AnosRui FonteNo ratings yet
- Main 71Document6 pagesMain 71pokharelriwaj82No ratings yet
- CCO Boston 2016 SlidesDocument55 pagesCCO Boston 2016 SlidesPD18No ratings yet
- VirologyDocument31 pagesVirologyDonzzkie DonNo ratings yet
- 4 Current Management of Esophageal Atresia and Tracheoesophageal FistulaDocument38 pages4 Current Management of Esophageal Atresia and Tracheoesophageal FistulaTurabayo Jean LéonardNo ratings yet
- GuillainBarrE EVR CENETECDocument3 pagesGuillainBarrE EVR CENETECDavid BVNo ratings yet
- Oral Presentations: Viral Hepatitis C: TherapyDocument2 pagesOral Presentations: Viral Hepatitis C: TherapyWilson WqaNo ratings yet
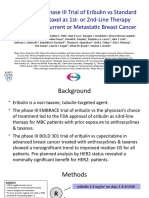
- Randomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast CancerDocument14 pagesRandomized Phase III Trial of Eribulin Vs Standard Weekly Paclitaxel As 1st-Or 2nd-Line Therapy For Locally Recurrent or Metastatic Breast Canceralberto cabelloNo ratings yet
- Target 25 Subjects Every Week: 304 Positive Patients Samples (Symptomatic & Asymptomatic) - For Self-UseDocument87 pagesTarget 25 Subjects Every Week: 304 Positive Patients Samples (Symptomatic & Asymptomatic) - For Self-Usenataniel josué alvarezNo ratings yet
- William C. Cushman, MD, FACP, FAHA: Veterans Affairs Medical Center, Memphis, TN For The ACCORD Study GroupDocument24 pagesWilliam C. Cushman, MD, FACP, FAHA: Veterans Affairs Medical Center, Memphis, TN For The ACCORD Study GroupCardiologyNetwork.comNo ratings yet
- SGLT2 Inhibitor Therapy in Type 2 DiabetesDocument25 pagesSGLT2 Inhibitor Therapy in Type 2 DiabetesMagdy GabrNo ratings yet
- Ix FinalDocument17 pagesIx FinalAyushi SinghNo ratings yet
- Clinical Preparation Form N414Document12 pagesClinical Preparation Form N414api-403419438No ratings yet
- Nejmc 2313517Document2 pagesNejmc 2313517carb0ne14rNo ratings yet
- Antiretroviral DrugsDocument26 pagesAntiretroviral DrugsAmit ShahNo ratings yet
- NEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaDocument18 pagesNEONATOLOGI - Sepsis Neonatorum + TTN + Neo PneumoniaGaluh Martin MaytasariNo ratings yet
- Liver Function Test InterpretationDocument48 pagesLiver Function Test InterpretationKiattipoom Sukkulcharoen100% (1)
- Shahian2009 Halaman 12 DikonversiDocument1 pageShahian2009 Halaman 12 DikonversiKhairunisa SinulinggaNo ratings yet
- Moderate and Extreme HypofractionationDocument32 pagesModerate and Extreme HypofractionationsamuelfsjNo ratings yet
- Management of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative ManagementDocument12 pagesManagement of Acute Spinal Cord Injury - A Summary of The Evidence Pertaining To The Acute Management, Operative and Non-Operative Managementzee zeeNo ratings yet
- Class 12 Investigatory Project by Heymang AgarwalDocument30 pagesClass 12 Investigatory Project by Heymang AgarwalHEYMANG AGARWALNo ratings yet
- Stop Unsafe Sex: Impact On AIDS and Unwanted PregnancyDocument9 pagesStop Unsafe Sex: Impact On AIDS and Unwanted PregnancyTilahun MikiasNo ratings yet
- Aplio Platinum Series Innovation 2016Document4 pagesAplio Platinum Series Innovation 2016SikliNo ratings yet
- Model Exam For Nurse 2016E.CDocument19 pagesModel Exam For Nurse 2016E.Ctemesgen AsmamawNo ratings yet
- Lecture 4 Biliary TreeDocument31 pagesLecture 4 Biliary TreeattooNo ratings yet
- RHU Situanional ReportDocument8 pagesRHU Situanional ReportErnest AtonNo ratings yet
- PhysioEx Exercise 5Document21 pagesPhysioEx Exercise 5Sinisa Ristic100% (1)
- Tubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSDocument12 pagesTubercular Meningitis in Children: Grisda Ledivia Lay, S.Ked 1508010038 Pembimbing: DR - Donny Argie, SP - BSAulia PuspitaNo ratings yet
- Preventive Dentistry 1Document19 pagesPreventive Dentistry 1blue nNo ratings yet
- I Notes Ophthalmology PDFDocument690 pagesI Notes Ophthalmology PDFpriya arrachman0% (1)
- DCLRXLFHG PDFDocument144 pagesDCLRXLFHG PDFtoniledoNo ratings yet
- Perth Sunday Times - Week 1 - 18/4/2010Document1 pagePerth Sunday Times - Week 1 - 18/4/2010John_Bishop_3317No ratings yet
- De Thi de Xuat Tieng Anh 10Document16 pagesDe Thi de Xuat Tieng Anh 10Alin NguyenNo ratings yet
- Kindle Hamad 28 MarcDocument1,646 pagesKindle Hamad 28 MarczozNo ratings yet
- Anaesthetic Challenges and Management of Myelomeningocele RepairDocument6 pagesAnaesthetic Challenges and Management of Myelomeningocele RepairprastiaNo ratings yet
- Councelling and History TakingDocument5 pagesCouncelling and History TakingbashingarNo ratings yet
- Effects and Costs of Real-Time Cardiac Telerehabilitation - Randomised Controlled Non - Inferiority TrialDocument8 pagesEffects and Costs of Real-Time Cardiac Telerehabilitation - Randomised Controlled Non - Inferiority TrialarwitarahayuNo ratings yet
- Gastrointestinal - Mucosal.repair - And.experimental - Therapeutics Ublog - TKDocument261 pagesGastrointestinal - Mucosal.repair - And.experimental - Therapeutics Ublog - TKpotaiskiNo ratings yet
- Essay PovertyDocument5 pagesEssay Povertyrbafdvwhd100% (2)
- Cues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationDocument2 pagesCues Nursing Diagnosis Analysis Goals & Objectives Intervention Rationale EvaluationMiggy SikatNo ratings yet
- IB Biology Revision Spreadsheet - EvolutionDocument8 pagesIB Biology Revision Spreadsheet - Evolutionpari meharunkarNo ratings yet
- Anti Nutritional FactorsDocument17 pagesAnti Nutritional FactorsMalvika Shah JainNo ratings yet
- Results of Postoperative Hallux Valgus Correction After Middle Shaft (Scarf & Meyer) and The Proximal (Juvara) Osteotomies of I Metatarsal BoneDocument5 pagesResults of Postoperative Hallux Valgus Correction After Middle Shaft (Scarf & Meyer) and The Proximal (Juvara) Osteotomies of I Metatarsal BoneMonika Diaz KristyanindaNo ratings yet
- Being A Medical Student and Locomotor SystemDocument22 pagesBeing A Medical Student and Locomotor SystemSamuel YudhistiraNo ratings yet
- Paeds Notes2Document126 pagesPaeds Notes2Ashley LewisNo ratings yet
- Diabetes in Pregnancy: DR Omar Abu-AzzamDocument36 pagesDiabetes in Pregnancy: DR Omar Abu-AzzamRoba Mohmed AlamroNo ratings yet