
Kidney Function Tests 2
Kidney Function Tests 2
You might also like
- Practice Exam-10000 SeriesDocument12 pagesPractice Exam-10000 SeriesJuan Romero86% (29)
- Ward Round ProformaDocument2 pagesWard Round ProformaAnonymous no7EOvHlNo ratings yet
- Nursing Care Plan-AscitesDocument10 pagesNursing Care Plan-AscitesKayki Louise75% (4)
- Arcipe Iccu Case 5Document98 pagesArcipe Iccu Case 5Maria Charis Anne Indanan100% (1)
- Urine AnalysisDocument69 pagesUrine Analysisvinay0717100% (3)
- Case Study 18Document5 pagesCase Study 18Natalie Meltzer0% (2)
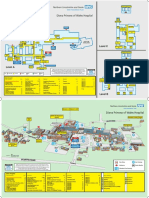
- Diana Princess of Wales Hospital: Level CDocument2 pagesDiana Princess of Wales Hospital: Level CTeamkamal FillahNo ratings yet
- Renal FunctionsDocument30 pagesRenal FunctionsJay Andrea Vea Israel100% (1)
- Renal Function TestsDocument36 pagesRenal Function TestsLawal Bello DanchadiNo ratings yet
- HTTPDocument10 pagesHTTPkasmiatiNo ratings yet
- Urine Analysis and BiuretDocument30 pagesUrine Analysis and BiuretTom Anthony TonguiaNo ratings yet
- Chronic Kidney Disease in Dogs and Cats: Joseph W. BartgesDocument24 pagesChronic Kidney Disease in Dogs and Cats: Joseph W. BartgesDany CamposNo ratings yet
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyNo ratings yet
- Integral University, Lucknow: Session:2019-2020Document6 pagesIntegral University, Lucknow: Session:2019-2020Kausal VermaNo ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
- 099 - Acute Renal Failure - Di PDFDocument2 pages099 - Acute Renal Failure - Di PDFSetiya Dini LarasatiNo ratings yet
- Final Laboratory ProceduresDocument14 pagesFinal Laboratory ProceduresJosh BlasNo ratings yet
- TABIJEdiagnosticDocument2 pagesTABIJEdiagnosticJaysellePuguonTabijeNo ratings yet
- 2012 01 Patho (CP) Kidney Function TestsDocument6 pages2012 01 Patho (CP) Kidney Function TestsJan Eric RiveraNo ratings yet
- Chronic Kidney Disease Stage 5Document21 pagesChronic Kidney Disease Stage 5Kristine Anne Soriano100% (1)
- Ren Function TestDocument10 pagesRen Function TestSankha DasNo ratings yet
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- L4 KFTsDocument4 pagesL4 KFTsRobin TikhatriNo ratings yet
- Farmakoterapi Penyakit Gangguan GinjalDocument24 pagesFarmakoterapi Penyakit Gangguan GinjaltiaraNo ratings yet
- Clinical PathologyDocument7 pagesClinical PathologyMustafa El-saeedNo ratings yet
- Renal Function TestsDocument43 pagesRenal Function TestsAbdulelah MurshidNo ratings yet
- Dipstick UrinalysisDocument9 pagesDipstick UrinalysisAbdul Ghaffar AbdullahNo ratings yet
- Proteinuria en Perros y GatosDocument16 pagesProteinuria en Perros y GatosKaren PMNo ratings yet
- Somaville University Faculty of Medicine Urology &nephrology Lecturer: DR - Osman Urine Analyze Presentation by Group ADocument49 pagesSomaville University Faculty of Medicine Urology &nephrology Lecturer: DR - Osman Urine Analyze Presentation by Group ALayla CabduqaadirNo ratings yet
- Acuterenalfailure2filesmerged 190509071023Document85 pagesAcuterenalfailure2filesmerged 190509071023ellise abundoNo ratings yet
- المحاطرة الاولة كيمياء سريريةDocument35 pagesالمحاطرة الاولة كيمياء سريريةMohamedErrmaliNo ratings yet
- UrineDocument17 pagesUrinealynne_pascua8530No ratings yet
- REVIEW 2023 AUBF Basics On Chemical Tests For UrineDocument84 pagesREVIEW 2023 AUBF Basics On Chemical Tests For UrineJheshari VinaNo ratings yet
- Introduction of CKDDocument7 pagesIntroduction of CKDAndrelyn Balangui LumingisNo ratings yet
- Acute Renal FailureDocument4 pagesAcute Renal FailurePerrilyn PereyNo ratings yet
- Medical Scenario 5Document70 pagesMedical Scenario 5murphy 1087No ratings yet
- Renal Function Test: Red Sea University Biochemistry Dept. LabDocument21 pagesRenal Function Test: Red Sea University Biochemistry Dept. LabKhalid AbdullahNo ratings yet
- Acute Kidney DiseaseDocument2 pagesAcute Kidney DiseaseJeff CorpuzNo ratings yet
- Urinalysis Lab 2012Document4 pagesUrinalysis Lab 2012PaolodeDiosNo ratings yet
- Kidney18 407Document4 pagesKidney18 407api-240473826No ratings yet
- Acute Renal Failure & Chronic Renal FailureDocument38 pagesAcute Renal Failure & Chronic Renal FailureArti GondNo ratings yet
- Lab Policies Urinalysis - Clinetek Status and Visual Lab 1583Document17 pagesLab Policies Urinalysis - Clinetek Status and Visual Lab 1583hunnylandNo ratings yet
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocument15 pagesNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiNo ratings yet
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocument15 pagesNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiNo ratings yet
- Abeer Renal Function Testsamr Renal Function Tests Renal BlockDocument22 pagesAbeer Renal Function Testsamr Renal Function Tests Renal BlockAbeer AhmedNo ratings yet
- 6 - Clinical 2Document46 pages6 - Clinical 2levan guluaNo ratings yet
- Liver Function TestDocument17 pagesLiver Function TestKarthiyayini .S.JNo ratings yet
- Urine Analysis: Assist. Prof. Biochemistry Dep., Faculty of Medicine Asu & UqDocument21 pagesUrine Analysis: Assist. Prof. Biochemistry Dep., Faculty of Medicine Asu & UqArjunaPamungkasNo ratings yet
- Diseases of Urogenital TractDocument170 pagesDiseases of Urogenital TractMuhammadNo ratings yet
- Chronic Kidney Failure Transplant 2Document22 pagesChronic Kidney Failure Transplant 2Gail Leslie HernandezNo ratings yet
- Acute Kidney FailureDocument2 pagesAcute Kidney FailureKunjan ShahNo ratings yet
- Kidney DisorderDocument94 pagesKidney DisorderBok MatthewNo ratings yet
- UrinsryDocument10 pagesUrinsryAzizan HakimNo ratings yet
- CKDDDocument11 pagesCKDDAnaNo ratings yet
- San Pedro College: A Case Study inDocument15 pagesSan Pedro College: A Case Study inKyla ValenciaNo ratings yet
- Medical Surgical Nursing - NeuroDocument19 pagesMedical Surgical Nursing - NeuroChristian EstevesNo ratings yet
- Physiology II Lab.2Document5 pagesPhysiology II Lab.2الرضا التميميNo ratings yet
- Liver Function Tests and Their InterpretationDocument9 pagesLiver Function Tests and Their InterpretationSuresh KumarNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- WASH in SCHOOL Monitoring ToolDocument13 pagesWASH in SCHOOL Monitoring ToolHarold MercadoNo ratings yet
- Acute Management of Open Fractures: An Evidence-Based ReviewDocument23 pagesAcute Management of Open Fractures: An Evidence-Based ReviewerdiansyahzuldiNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Insulin TherapyDocument62 pagesInsulin TherapyCharisma Bimara CozyNo ratings yet
- Doctor ListDocument5 pagesDoctor ListAbhijitNo ratings yet
- Daftar Nama ObatDocument5 pagesDaftar Nama ObatGabriyah HamzahNo ratings yet
- Initial Medical Evaluation Form For JO1 ApplicantsDocument1 pageInitial Medical Evaluation Form For JO1 ApplicantsBilly Joe BaradiNo ratings yet
- The Social Psychology of Drug AbuseDocument6 pagesThe Social Psychology of Drug AbusecikumaticNo ratings yet
- Screw Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisDocument11 pagesScrew Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisMario Troncoso AndersennNo ratings yet
- A Grand Case UgibDocument84 pagesA Grand Case UgibAdrianne Kricia100% (2)
- Asthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaDocument53 pagesAsthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaCornelia CindyNo ratings yet
- Infection ControlDocument13 pagesInfection ControlSheryl Reyes100% (1)
- Strong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalDocument3 pagesStrong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalninaNo ratings yet
- Class 1.1 Intro To VMMC UpdatedDocument24 pagesClass 1.1 Intro To VMMC UpdatedTracyNo ratings yet
- Increased Plasma Bicarbonate and Growth Hormone After An Oral Glutamine LoadDocument4 pagesIncreased Plasma Bicarbonate and Growth Hormone After An Oral Glutamine LoadsackeydzidzorNo ratings yet
- Kenis Et Al 2023 A Multicenter Randomized Controlled Trial (RCT) For The Effectiveness of Comprehensive GeriatricDocument1 pageKenis Et Al 2023 A Multicenter Randomized Controlled Trial (RCT) For The Effectiveness of Comprehensive GeriatricparamitaekadevaNo ratings yet
- Reflection FinalDocument10 pagesReflection FinalRichardTangNo ratings yet
- Endometriosis GuidelineDocument44 pagesEndometriosis GuidelineHen DriNo ratings yet
- Murtagh S Patient EducationDocument3 pagesMurtagh S Patient EducationMAYNo ratings yet
- HA Lec Overall 16 23Document8 pagesHA Lec Overall 16 23Sofia Denise JoseNo ratings yet
- A Special Interview With Dr. Daniel AmenDocument19 pagesA Special Interview With Dr. Daniel Amenzapperindia100% (1)
- (PPT) CTSDocument21 pages(PPT) CTSNadya Nurbany RafmanNo ratings yet
- HemophiliaDocument60 pagesHemophiliavibhurocksNo ratings yet
- Resource Material - Day 1 Primary Register Activity - ANC Register - 0Document3 pagesResource Material - Day 1 Primary Register Activity - ANC Register - 0Ranjeet Singh KatariaNo ratings yet
- Compartment SyndromeDocument25 pagesCompartment SyndromeestyjayantiNo ratings yet
- Ziabeen ThesisDocument109 pagesZiabeen ThesisHuma Hameed DogarNo ratings yet

























































































Download as ppt, pdf, or txt
You might also like
- Practice Exam-10000 SeriesDocument12 pagesPractice Exam-10000 SeriesJuan Romero86% (29)
- Ward Round ProformaDocument2 pagesWard Round ProformaAnonymous no7EOvHlNo ratings yet
- Nursing Care Plan-AscitesDocument10 pagesNursing Care Plan-AscitesKayki Louise75% (4)
- Arcipe Iccu Case 5Document98 pagesArcipe Iccu Case 5Maria Charis Anne Indanan100% (1)
- Urine AnalysisDocument69 pagesUrine Analysisvinay0717100% (3)
- Case Study 18Document5 pagesCase Study 18Natalie Meltzer0% (2)
- Diana Princess of Wales Hospital: Level CDocument2 pagesDiana Princess of Wales Hospital: Level CTeamkamal FillahNo ratings yet
- Renal FunctionsDocument30 pagesRenal FunctionsJay Andrea Vea Israel100% (1)
- Renal Function TestsDocument36 pagesRenal Function TestsLawal Bello DanchadiNo ratings yet
- HTTPDocument10 pagesHTTPkasmiatiNo ratings yet
- Urine Analysis and BiuretDocument30 pagesUrine Analysis and BiuretTom Anthony TonguiaNo ratings yet
- Chronic Kidney Disease in Dogs and Cats: Joseph W. BartgesDocument24 pagesChronic Kidney Disease in Dogs and Cats: Joseph W. BartgesDany CamposNo ratings yet
- Renal Function Test Amcj 8Document42 pagesRenal Function Test Amcj 8Md. Saifur Rahman SunnyNo ratings yet
- Integral University, Lucknow: Session:2019-2020Document6 pagesIntegral University, Lucknow: Session:2019-2020Kausal VermaNo ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
- 099 - Acute Renal Failure - Di PDFDocument2 pages099 - Acute Renal Failure - Di PDFSetiya Dini LarasatiNo ratings yet
- Final Laboratory ProceduresDocument14 pagesFinal Laboratory ProceduresJosh BlasNo ratings yet
- TABIJEdiagnosticDocument2 pagesTABIJEdiagnosticJaysellePuguonTabijeNo ratings yet
- 2012 01 Patho (CP) Kidney Function TestsDocument6 pages2012 01 Patho (CP) Kidney Function TestsJan Eric RiveraNo ratings yet
- Chronic Kidney Disease Stage 5Document21 pagesChronic Kidney Disease Stage 5Kristine Anne Soriano100% (1)
- Ren Function TestDocument10 pagesRen Function TestSankha DasNo ratings yet
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- L4 KFTsDocument4 pagesL4 KFTsRobin TikhatriNo ratings yet
- Farmakoterapi Penyakit Gangguan GinjalDocument24 pagesFarmakoterapi Penyakit Gangguan GinjaltiaraNo ratings yet
- Clinical PathologyDocument7 pagesClinical PathologyMustafa El-saeedNo ratings yet
- Renal Function TestsDocument43 pagesRenal Function TestsAbdulelah MurshidNo ratings yet
- Dipstick UrinalysisDocument9 pagesDipstick UrinalysisAbdul Ghaffar AbdullahNo ratings yet
- Proteinuria en Perros y GatosDocument16 pagesProteinuria en Perros y GatosKaren PMNo ratings yet
- Somaville University Faculty of Medicine Urology &nephrology Lecturer: DR - Osman Urine Analyze Presentation by Group ADocument49 pagesSomaville University Faculty of Medicine Urology &nephrology Lecturer: DR - Osman Urine Analyze Presentation by Group ALayla CabduqaadirNo ratings yet
- Acuterenalfailure2filesmerged 190509071023Document85 pagesAcuterenalfailure2filesmerged 190509071023ellise abundoNo ratings yet
- المحاطرة الاولة كيمياء سريريةDocument35 pagesالمحاطرة الاولة كيمياء سريريةMohamedErrmaliNo ratings yet
- UrineDocument17 pagesUrinealynne_pascua8530No ratings yet
- REVIEW 2023 AUBF Basics On Chemical Tests For UrineDocument84 pagesREVIEW 2023 AUBF Basics On Chemical Tests For UrineJheshari VinaNo ratings yet
- Introduction of CKDDocument7 pagesIntroduction of CKDAndrelyn Balangui LumingisNo ratings yet
- Acute Renal FailureDocument4 pagesAcute Renal FailurePerrilyn PereyNo ratings yet
- Medical Scenario 5Document70 pagesMedical Scenario 5murphy 1087No ratings yet
- Renal Function Test: Red Sea University Biochemistry Dept. LabDocument21 pagesRenal Function Test: Red Sea University Biochemistry Dept. LabKhalid AbdullahNo ratings yet
- Acute Kidney DiseaseDocument2 pagesAcute Kidney DiseaseJeff CorpuzNo ratings yet
- Urinalysis Lab 2012Document4 pagesUrinalysis Lab 2012PaolodeDiosNo ratings yet
- Kidney18 407Document4 pagesKidney18 407api-240473826No ratings yet
- Acute Renal Failure & Chronic Renal FailureDocument38 pagesAcute Renal Failure & Chronic Renal FailureArti GondNo ratings yet
- Lab Policies Urinalysis - Clinetek Status and Visual Lab 1583Document17 pagesLab Policies Urinalysis - Clinetek Status and Visual Lab 1583hunnylandNo ratings yet
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocument15 pagesNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiNo ratings yet
- Nusing Assessment Guide: Kidney Failure (CKD) Area: CCUDocument15 pagesNusing Assessment Guide: Kidney Failure (CKD) Area: CCUAbbas AwfiNo ratings yet
- Abeer Renal Function Testsamr Renal Function Tests Renal BlockDocument22 pagesAbeer Renal Function Testsamr Renal Function Tests Renal BlockAbeer AhmedNo ratings yet
- 6 - Clinical 2Document46 pages6 - Clinical 2levan guluaNo ratings yet
- Liver Function TestDocument17 pagesLiver Function TestKarthiyayini .S.JNo ratings yet
- Urine Analysis: Assist. Prof. Biochemistry Dep., Faculty of Medicine Asu & UqDocument21 pagesUrine Analysis: Assist. Prof. Biochemistry Dep., Faculty of Medicine Asu & UqArjunaPamungkasNo ratings yet
- Diseases of Urogenital TractDocument170 pagesDiseases of Urogenital TractMuhammadNo ratings yet
- Chronic Kidney Failure Transplant 2Document22 pagesChronic Kidney Failure Transplant 2Gail Leslie HernandezNo ratings yet
- Acute Kidney FailureDocument2 pagesAcute Kidney FailureKunjan ShahNo ratings yet
- Kidney DisorderDocument94 pagesKidney DisorderBok MatthewNo ratings yet
- UrinsryDocument10 pagesUrinsryAzizan HakimNo ratings yet
- CKDDDocument11 pagesCKDDAnaNo ratings yet
- San Pedro College: A Case Study inDocument15 pagesSan Pedro College: A Case Study inKyla ValenciaNo ratings yet
- Medical Surgical Nursing - NeuroDocument19 pagesMedical Surgical Nursing - NeuroChristian EstevesNo ratings yet
- Physiology II Lab.2Document5 pagesPhysiology II Lab.2الرضا التميميNo ratings yet
- Liver Function Tests and Their InterpretationDocument9 pagesLiver Function Tests and Their InterpretationSuresh KumarNo ratings yet
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- WASH in SCHOOL Monitoring ToolDocument13 pagesWASH in SCHOOL Monitoring ToolHarold MercadoNo ratings yet
- Acute Management of Open Fractures: An Evidence-Based ReviewDocument23 pagesAcute Management of Open Fractures: An Evidence-Based ReviewerdiansyahzuldiNo ratings yet
- De Quervain's TendinosisDocument19 pagesDe Quervain's TendinosisSze Wing LeeNo ratings yet
- Insulin TherapyDocument62 pagesInsulin TherapyCharisma Bimara CozyNo ratings yet
- Doctor ListDocument5 pagesDoctor ListAbhijitNo ratings yet
- Daftar Nama ObatDocument5 pagesDaftar Nama ObatGabriyah HamzahNo ratings yet
- Initial Medical Evaluation Form For JO1 ApplicantsDocument1 pageInitial Medical Evaluation Form For JO1 ApplicantsBilly Joe BaradiNo ratings yet
- The Social Psychology of Drug AbuseDocument6 pagesThe Social Psychology of Drug AbusecikumaticNo ratings yet
- Screw Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisDocument11 pagesScrew Retained Vs Cement Retained Implant-Supported Fixed Dental ProsthesisMario Troncoso AndersennNo ratings yet
- A Grand Case UgibDocument84 pagesA Grand Case UgibAdrianne Kricia100% (2)
- Asthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaDocument53 pagesAsthma Bronchiale: Dr. Ramelan Navy Hospital SurabayaCornelia CindyNo ratings yet
- Infection ControlDocument13 pagesInfection ControlSheryl Reyes100% (1)
- Strong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalDocument3 pagesStrong: Nutritional Risk Screening Tool For Children Aged Month - 18 Years On Admission To The HospitalninaNo ratings yet
- Class 1.1 Intro To VMMC UpdatedDocument24 pagesClass 1.1 Intro To VMMC UpdatedTracyNo ratings yet
- Increased Plasma Bicarbonate and Growth Hormone After An Oral Glutamine LoadDocument4 pagesIncreased Plasma Bicarbonate and Growth Hormone After An Oral Glutamine LoadsackeydzidzorNo ratings yet
- Kenis Et Al 2023 A Multicenter Randomized Controlled Trial (RCT) For The Effectiveness of Comprehensive GeriatricDocument1 pageKenis Et Al 2023 A Multicenter Randomized Controlled Trial (RCT) For The Effectiveness of Comprehensive GeriatricparamitaekadevaNo ratings yet
- Reflection FinalDocument10 pagesReflection FinalRichardTangNo ratings yet
- Endometriosis GuidelineDocument44 pagesEndometriosis GuidelineHen DriNo ratings yet
- Murtagh S Patient EducationDocument3 pagesMurtagh S Patient EducationMAYNo ratings yet
- HA Lec Overall 16 23Document8 pagesHA Lec Overall 16 23Sofia Denise JoseNo ratings yet
- A Special Interview With Dr. Daniel AmenDocument19 pagesA Special Interview With Dr. Daniel Amenzapperindia100% (1)
- (PPT) CTSDocument21 pages(PPT) CTSNadya Nurbany RafmanNo ratings yet
- HemophiliaDocument60 pagesHemophiliavibhurocksNo ratings yet
- Resource Material - Day 1 Primary Register Activity - ANC Register - 0Document3 pagesResource Material - Day 1 Primary Register Activity - ANC Register - 0Ranjeet Singh KatariaNo ratings yet
- Compartment SyndromeDocument25 pagesCompartment SyndromeestyjayantiNo ratings yet
- Ziabeen ThesisDocument109 pagesZiabeen ThesisHuma Hameed DogarNo ratings yet