Download as pptx, pdf, or txt
You might also like
- Physical Biology of The Cell - ContentDocument12 pagesPhysical Biology of The Cell - ContentkonjNo ratings yet
- EMRCS Abdomin AnatomyDocument54 pagesEMRCS Abdomin AnatomyShakirNo ratings yet
- Schwartz UrologyDocument10 pagesSchwartz UrologyRem Alfelor100% (1)
- 4 Peritoneum PDFDocument64 pages4 Peritoneum PDFN ANo ratings yet
- LeukemiaDocument47 pagesLeukemiaRaghav Oberoi100% (1)
- HemodialysisDocument19 pagesHemodialysisK.R.Raguram88% (26)
- Pancreas DetailsDocument13 pagesPancreas DetailsrishistudyzNo ratings yet
- Pancreas: Anatomy of The PancreasDocument11 pagesPancreas: Anatomy of The PancreasHart ElettNo ratings yet
- Yusi - Anatomy of The Urinary Tract 2009 12-7Document129 pagesYusi - Anatomy of The Urinary Tract 2009 12-7abstabsNo ratings yet
- Phy Project-Pages-Deleted-MergedDocument16 pagesPhy Project-Pages-Deleted-MergedrishistudyzNo ratings yet
- Chapter Summary - PANCREAS Final (Schwartz) PDFDocument19 pagesChapter Summary - PANCREAS Final (Schwartz) PDFMiguel Cuevas DolotNo ratings yet
- Pancreas Biology ProjectDocument16 pagesPancreas Biology ProjectrishistudyzNo ratings yet
- Abdomen 9: DR - Bushra Haseeb BDS, Rds Demonstrator in Dental Section Azra Naheed Medical CollegeDocument14 pagesAbdomen 9: DR - Bushra Haseeb BDS, Rds Demonstrator in Dental Section Azra Naheed Medical CollegeTanveer AhmadNo ratings yet
- PancreaDocument21 pagesPancreasiddharth.roy26587No ratings yet
- Anatomy of GALL BLADDER PANCREAS 2016Document32 pagesAnatomy of GALL BLADDER PANCREAS 2016Omar Ali AyoubkhanNo ratings yet
- Development of GIT - IDocument69 pagesDevelopment of GIT - IAarushi JainNo ratings yet
- Development of Alimentary System Part 1Document52 pagesDevelopment of Alimentary System Part 1Aarushi JainNo ratings yet
- Abdomen (Repaired)Document174 pagesAbdomen (Repaired)Merellyn Hurtado PachecoNo ratings yet
- Abdomen (Repaired)Document172 pagesAbdomen (Repaired)OstazNo ratings yet
- RectumDocument43 pagesRectummidhunramesh007100% (4)
- L6 - OmentumDocument12 pagesL6 - OmentumGoodone OneNo ratings yet
- Pancreas - Endocrine and Exocrine Functions - Medical LibraryDocument16 pagesPancreas - Endocrine and Exocrine Functions - Medical Libraryjean PiedraNo ratings yet
- M1207 GIT E2 ForegutDocument29 pagesM1207 GIT E2 Foregutkavinduherath2000No ratings yet
- Seminar Cs 15 NovDocument24 pagesSeminar Cs 15 Novzeenatn1995No ratings yet
- DIgestive System EmbDocument85 pagesDIgestive System EmbDanish GujjarNo ratings yet
- Anatomy (Compatibility Mode)Document34 pagesAnatomy (Compatibility Mode)your babysurgeonNo ratings yet
- KidneysDocument6 pagesKidneysAmbg GhalyNo ratings yet
- Anterior Posterior: o Posterior Renal Fascia Is Also Known As Zuckerkandl's Fascia)Document4 pagesAnterior Posterior: o Posterior Renal Fascia Is Also Known As Zuckerkandl's Fascia)Lester AldridgeNo ratings yet
- UT AnatomyDocument35 pagesUT AnatomyAngel SaraNo ratings yet
- Anatomy of Urinary Tract BaruDocument68 pagesAnatomy of Urinary Tract BaruAdya ArradikhaNo ratings yet
- Abdomen #7: DR - Bushra Haseeb BDS, Rds Demonstrator in Dental Section Azra Naheed Medical CollegeDocument21 pagesAbdomen #7: DR - Bushra Haseeb BDS, Rds Demonstrator in Dental Section Azra Naheed Medical CollegeTanveer AhmadNo ratings yet
- Peritoneum and Gastro-Intestinal TractDocument108 pagesPeritoneum and Gastro-Intestinal TractKAYISIRE EMERYNo ratings yet
- Mahadevan 2019Document5 pagesMahadevan 2019Andreea BuftiaNo ratings yet
- The Concise Medical Encyclopedia - AnnDocument520 pagesThe Concise Medical Encyclopedia - AnnANIL KUMARNo ratings yet
- Urinary Sytem - Gross Anatomy Jan 2023Document153 pagesUrinary Sytem - Gross Anatomy Jan 2023bschaliyath.mnlNo ratings yet
- DR Laxman Khanal Bpkihs 07-06-2013Document86 pagesDR Laxman Khanal Bpkihs 07-06-2013Bilal YimamNo ratings yet
- Anatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 JanDocument6 pagesAnatomy, Abdomen and Pelvis, Kidneys: Statpearls (Internet) - Treasure Island (FL) : Statpearls Publishing 2022 Janvenus ohNo ratings yet
- PancreasDocument21 pagesPancreasshivamnamdeo758No ratings yet
- The Kidneys (Nephros) : FunctionsDocument6 pagesThe Kidneys (Nephros) : FunctionsOjambo FlaviaNo ratings yet
- 3.abdomen and Thorax - OSPEDocument16 pages3.abdomen and Thorax - OSPEArjun KumarNo ratings yet
- 4Document9 pages4Marielle Anne TuazonNo ratings yet
- PeritoneumDocument29 pagesPeritoneumpariyahajihosseinzadeh4No ratings yet
- M1207: Gastrointestinal System Embryology Lecture 01: Dr. Sampath PaththinigeDocument30 pagesM1207: Gastrointestinal System Embryology Lecture 01: Dr. Sampath Paththinigekavinduherath2000No ratings yet
- Duodenum, Pancreas, Liver, and Gallbladder Practice QuizDocument5 pagesDuodenum, Pancreas, Liver, and Gallbladder Practice QuizMr .Hacker xDNo ratings yet
- 7) Anatomy of OMENTUMDocument22 pages7) Anatomy of OMENTUMGoodone OneNo ratings yet
- Anatomy StomachDocument2 pagesAnatomy StomachtristineNo ratings yet
- Peritoneum 2022Document86 pagesPeritoneum 2022Tayyib KhanNo ratings yet
- PancreasDocument1 pagePancreasJulia IshakNo ratings yet
- Anatomy of The Kidney and UreterDocument6 pagesAnatomy of The Kidney and UreterMario Ivan De la Cruz LaraNo ratings yet
- Anatomy of Hepatobiliary SystemDocument54 pagesAnatomy of Hepatobiliary SystemM.GANESHNo ratings yet
- Lecture 12Document4 pagesLecture 12A-Naeem To'mah Al-sawaieNo ratings yet
- Anatomy MCQ SBA eMRCSDocument121 pagesAnatomy MCQ SBA eMRCSTowhid HasanNo ratings yet
- Peritonem A ND Peritonealcavity PDFDocument62 pagesPeritonem A ND Peritonealcavity PDFKarem MaaliNo ratings yet
- The Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityDocument44 pagesThe Urinary System: Muh - Iqbal Basri Anatomy Department Hasanuddin UniversityRahmawati HamudiNo ratings yet
- L31 - Renal SystemDocument30 pagesL31 - Renal SystemsairahhannahNo ratings yet
- Esphagus Stomach Duodenum Gross AnatomyDocument9 pagesEsphagus Stomach Duodenum Gross AnatomyWinchester LoapedNo ratings yet
- Lecture 10Document26 pagesLecture 10zahraaNo ratings yet
- Abdomen 2Document4 pagesAbdomen 2hieu.pNo ratings yet
- KidneyDocument40 pagesKidneyOlaifa victorNo ratings yet
- Gallblader AnatomyDocument5 pagesGallblader AnatomyAnonymous gYpFy0No ratings yet
- Histology and Gross Pancreas 2019Document59 pagesHistology and Gross Pancreas 2019Azwaah Hassan100% (1)
- Anatomy of The Peritoneal Cavity & OrgansDocument264 pagesAnatomy of The Peritoneal Cavity & OrgansmataNo ratings yet
- Cambridge IGCSE: Biology 0610/22Document16 pagesCambridge IGCSE: Biology 0610/22SAFFANAH NURNo ratings yet
- EBE Training QuestionsDocument12 pagesEBE Training Questionserichamilt0nNo ratings yet
- Biology SPM Chapter 6 Form 4Document157 pagesBiology SPM Chapter 6 Form 4Eeshvari Aom100% (4)
- Overview of RENAL: Dr. Wilson Arthur Zein, M. BiomedDocument34 pagesOverview of RENAL: Dr. Wilson Arthur Zein, M. BiomedAnnisNo ratings yet
- High-Intensity Interval Training, Solutions To The Programming Puzzle: Part I: Cardiopulmonary EmphasisDocument29 pagesHigh-Intensity Interval Training, Solutions To The Programming Puzzle: Part I: Cardiopulmonary EmphasisОстојић СтрахињаNo ratings yet
- Biology Revision Essay Questions and Answers For Secondary Kusoma - Co - .KeDocument48 pagesBiology Revision Essay Questions and Answers For Secondary Kusoma - Co - .Kestevewanji0% (1)
- Genetics and Probability Practice ProblemsDocument2 pagesGenetics and Probability Practice ProblemsMarcos Valdez Jr.0% (1)
- Methods of Physical ExaminationDocument41 pagesMethods of Physical ExaminationAbhishiktaAbhi100% (1)
- ArticuloDocument3 pagesArticuloJose Manuel OrtizNo ratings yet
- Wushu Training RoutinesDocument3 pagesWushu Training Routinessagor sagorNo ratings yet
- The Path To Mindfulness-Part 2 The 3-Part BreathDocument3 pagesThe Path To Mindfulness-Part 2 The 3-Part BreathDeiana RanisavNo ratings yet
- Histology of Esophagus For 2nd Year by DR SUNDUSDocument21 pagesHistology of Esophagus For 2nd Year by DR SUNDUSMudassar RoomiNo ratings yet
- Formulir Surat Pengantar Pemeriksaan Kesehatan (SPPK)Document2 pagesFormulir Surat Pengantar Pemeriksaan Kesehatan (SPPK)rachreinaldi49No ratings yet
- Anatomy Phys Vol2aDocument540 pagesAnatomy Phys Vol2asanjay bareliyaNo ratings yet
- Textbook of Kinesiology 1St Edition V D Bindal Online Ebook Texxtbook Full Chapter PDFDocument69 pagesTextbook of Kinesiology 1St Edition V D Bindal Online Ebook Texxtbook Full Chapter PDFronald.martinez398100% (8)
- Acid-Base - Ppt-How To ReadDocument22 pagesAcid-Base - Ppt-How To ReadnursaidahNo ratings yet
- Permanent TissuesDocument16 pagesPermanent TissuesRiyashika RNo ratings yet
- MeconiumDocument53 pagesMeconiumAsherrie Bernardo100% (1)
- Respiration PDFDocument3 pagesRespiration PDFSOm KAntaNo ratings yet
- Blood GroupDocument44 pagesBlood Groupmujtaba100% (2)
- Chapter 21 Intro To CNS PharmaDocument8 pagesChapter 21 Intro To CNS PharmaChristine Annmarie TapawanNo ratings yet
- Name: Ellaine Jhane T. Domede Bsn1VDocument9 pagesName: Ellaine Jhane T. Domede Bsn1VNeil Floyd VenturaNo ratings yet
- Milk - Experiment 11Document16 pagesMilk - Experiment 11Joshuel MontecilloNo ratings yet
- Common Course Outline For: EXSC 2305 Exercise Physiology A. Course DescriptionDocument2 pagesCommon Course Outline For: EXSC 2305 Exercise Physiology A. Course DescriptionZedy GullesNo ratings yet
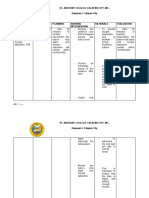
- St. Anthony College Calapan City, Inc. Bayanan I, Calapan CityDocument3 pagesSt. Anthony College Calapan City, Inc. Bayanan I, Calapan CityMike Faustino SolangonNo ratings yet
- Mrcog Part1Document7 pagesMrcog Part1Yogeshwari Pardeshi100% (4)
- Regulation of Respiration PDFDocument30 pagesRegulation of Respiration PDFRashmi DhunganaNo ratings yet