Download as pptx, pdf, or txt
You might also like
- Course, Unit, Lesson Plan B.sc.n.ii SemDocument25 pagesCourse, Unit, Lesson Plan B.sc.n.ii Semprachi jainNo ratings yet
- Case Reflection FormatDocument9 pagesCase Reflection Formatanusarannya100% (5)
- 118A - Chapter 1 - CRITICAL CARE NURSING LEC (EDITED) Handout #1Document14 pages118A - Chapter 1 - CRITICAL CARE NURSING LEC (EDITED) Handout #1Joanna Taylan100% (5)
- Club FootDocument46 pagesClub FootCarol Bruce100% (1)
- MOH Exam PaperDocument8 pagesMOH Exam PaperSubhajit SahaNo ratings yet
- Foot and Ankle BiomechanicsDocument25 pagesFoot and Ankle BiomechanicsSanh NguyễnNo ratings yet
- Chapter 5 Pediatric PodiatryDocument88 pagesChapter 5 Pediatric Podiatrypodmmgf100% (1)
- ARCHDocument63 pagesARCHDebashish Chanda100% (1)
- Arches of FootDocument75 pagesArches of Footvaibhav gowdaNo ratings yet
- Larsen Syndrome: - Dr. Kapil R JagtapDocument23 pagesLarsen Syndrome: - Dr. Kapil R JagtapKapil JagtapNo ratings yet
- Pes PlanusDocument18 pagesPes Planushacker ammerNo ratings yet
- Congenital Talipes Equino Varus (Ctev) - Nur HanisahDocument11 pagesCongenital Talipes Equino Varus (Ctev) - Nur HanisahNur HanisahNo ratings yet
- Orthopaedic Congenital Anomaly: Essy Dwi DamayanthiDocument59 pagesOrthopaedic Congenital Anomaly: Essy Dwi DamayanthiGufron MustofaNo ratings yet
- Coxa Vara and Coxa ValgaDocument34 pagesCoxa Vara and Coxa ValgaAnagha kNo ratings yet
- Congenital Talipes (Clubfoot)Document222 pagesCongenital Talipes (Clubfoot)Sampath MarasingheNo ratings yet
- CTEVDocument46 pagesCTEVjhogie afitnandriNo ratings yet
- NoemiDocument67 pagesNoemiJoshua Elli BajadaNo ratings yet
- Adult-Acquired Flatfoot DeformityDocument27 pagesAdult-Acquired Flatfoot DeformityNajeeb BsoulNo ratings yet
- Presentor-Dr. Momin Mohammad Farhan Moderator-Dr. M. A. Q. AnsariDocument48 pagesPresentor-Dr. Momin Mohammad Farhan Moderator-Dr. M. A. Q. Ansarimohammad farhanNo ratings yet
- AAOS - Clubfoot - ADCDocument17 pagesAAOS - Clubfoot - ADCMulya Imansyah100% (1)
- Knee, Ankle, and FootDocument143 pagesKnee, Ankle, and FootJackielyn C. AportaderaNo ratings yet
- Congenital Deformities: Gay G. Crisostomo-San Antonio, PTRP, MDDocument46 pagesCongenital Deformities: Gay G. Crisostomo-San Antonio, PTRP, MDJulia SalvioNo ratings yet
- CCPVDocument16 pagesCCPVdastgirrajaNo ratings yet
- Paediatric FlatfootDocument53 pagesPaediatric FlatfootAmr HassanNo ratings yet
- Club Foot-Dr J SahooDocument9 pagesClub Foot-Dr J SahooSheel Gupta100% (1)
- Acquired Deformities1 PDFDocument33 pagesAcquired Deformities1 PDFRishabh VermaNo ratings yet
- DR Chander Pal Dito, DelhiDocument87 pagesDR Chander Pal Dito, DelhiRohitChauhanNo ratings yet
- ClubfootDocument52 pagesClubfootArianto PrabowoNo ratings yet
- Achondroplasia: Orthopaedic and Traumatology Department Faculty of Medicine Hasanuddin UniversityDocument30 pagesAchondroplasia: Orthopaedic and Traumatology Department Faculty of Medicine Hasanuddin UniversityRayyan HidayatNo ratings yet
- Talar FractureDocument78 pagesTalar FractureRamin MaharjanNo ratings yet
- Cerebral Palsy: Kyaw Htet AungDocument28 pagesCerebral Palsy: Kyaw Htet AungKyaw Htet AungNo ratings yet
- CLUBFOOT, Polydactily, Spina BividaDocument39 pagesCLUBFOOT, Polydactily, Spina BividaRobertus Dwi AtmokoNo ratings yet
- Upper Limb Dislocation: Presented by Elias Godfrey Supervisor DR Swai 20 November 2017Document67 pagesUpper Limb Dislocation: Presented by Elias Godfrey Supervisor DR Swai 20 November 2017albertjosephNo ratings yet
- Approach To Pes CavusDocument52 pagesApproach To Pes CavusSubarna PaudelNo ratings yet
- Footdropkevinja 141118013605 Conversion Gate01 2Document26 pagesFootdropkevinja 141118013605 Conversion Gate01 2Musa LandeNo ratings yet
- Femur Bone FRACTUREDocument19 pagesFemur Bone FRACTUREAkshay BadoreNo ratings yet
- Orthopedics PDFDocument14 pagesOrthopedics PDFSam christenNo ratings yet
- Seminar On Ctev: Moderator-Dr - Manish Rajpoot (Assistant Professor GMC Bhopal) Presented By-Dr - Vivek Kumar (RSO 3)Document80 pagesSeminar On Ctev: Moderator-Dr - Manish Rajpoot (Assistant Professor GMC Bhopal) Presented By-Dr - Vivek Kumar (RSO 3)Sourabh AlawaNo ratings yet
- Genu Valgus Genu VarusDocument35 pagesGenu Valgus Genu VarusRatu FaniaNo ratings yet
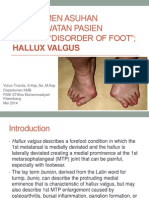
- Manajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREEDocument29 pagesManajemen Asuhan Keperawatan Pasien Dengan Disorder of Foot Hammer Toe and Hallux Valgus FREENovita DamaiyantiNo ratings yet
- 9 HipjointDocument36 pages9 HipjointBoyd benson kayomboNo ratings yet
- Shoulder and Hip DislocationsDocument48 pagesShoulder and Hip Dislocationscromwellopoku42No ratings yet
- The KneeDocument57 pagesThe Kneeniamh traceyNo ratings yet
- ClubfootDocument16 pagesClubfoothacker ammerNo ratings yet
- Arthrologi Blok 7 Tahun 2016 Edit IdaDocument59 pagesArthrologi Blok 7 Tahun 2016 Edit IdaNURHAYATUNISAHNo ratings yet
- DDHDocument174 pagesDDHVikas RaiNo ratings yet
- Cavus Foot 2015 Foot and Ankle ClinicsDocument13 pagesCavus Foot 2015 Foot and Ankle ClinicsRadu StoenescuNo ratings yet
- LL AmputationDocument119 pagesLL AmputationMpt SportsNo ratings yet
- Tuberculosis of Knee: Presented By: DR Dipendra Maharjan 2 Yr Resident, MS Orthopaedics NAMS, Bir HospitalDocument25 pagesTuberculosis of Knee: Presented By: DR Dipendra Maharjan 2 Yr Resident, MS Orthopaedics NAMS, Bir HospitalshravaniNo ratings yet
- CTEV - Congenital Club FootDocument43 pagesCTEV - Congenital Club FootIrfan Ali ShujahNo ratings yet
- CTEVDocument27 pagesCTEVandi firdha restuwatiNo ratings yet
- Club FootDocument104 pagesClub FootKittipong PoolketkitNo ratings yet
- Anterior Knee Pain Syndrome ReferatDocument28 pagesAnterior Knee Pain Syndrome ReferatnurulNo ratings yet
- Treating WristDocument71 pagesTreating WristSyahriadin SyamNo ratings yet
- Knee Sport Injuries Group 5Document102 pagesKnee Sport Injuries Group 5moshiegonNo ratings yet
- Polio Lower LimbDocument102 pagesPolio Lower Limbdr_s_ganesh100% (2)
- Common Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCDocument49 pagesCommon Lower Limb Fracture: DR Tarif Alakhras Orthopedic Surgeon KFMCahmad albab100% (1)
- Anatomy Biomechanics of AnkleDocument82 pagesAnatomy Biomechanics of AnklelypiheNo ratings yet
- Orthopedic Radiology Seth Mathus Ganz, DVM Surgery PDFDocument95 pagesOrthopedic Radiology Seth Mathus Ganz, DVM Surgery PDFViBoyViboyNo ratings yet
- CTEVDocument24 pagesCTEVwildanmalikNo ratings yet
- Congenital Talipes Equino Varus: by Mohd Amirnizam Ahmad NazariDocument54 pagesCongenital Talipes Equino Varus: by Mohd Amirnizam Ahmad NazariperrybonjoNo ratings yet
- Shoulder Pain OverviewDocument37 pagesShoulder Pain Overvieweddie bechillNo ratings yet
- Clase 22 D-NavicularDocument84 pagesClase 22 D-Naviculardavid1007sg David Gomez GomezNo ratings yet
- Roche Fact SheetDocument2 pagesRoche Fact SheetabhijitkumtakarNo ratings yet
- Drugs Acting On The Blood and The BloodDocument26 pagesDrugs Acting On The Blood and The BloodHealthy7No ratings yet
- Crucible Catalog Herbal GuideDocument24 pagesCrucible Catalog Herbal GuideFrancesca AckumburNo ratings yet
- Erceflora Is A Preparation Consisting of Suspension of Bacillus Clausii SporesDocument3 pagesErceflora Is A Preparation Consisting of Suspension of Bacillus Clausii Sporesbingl_073No ratings yet
- Innocent Heart Murmur: 6 Grades of Heart MurmursDocument11 pagesInnocent Heart Murmur: 6 Grades of Heart MurmursMohammad KatatoNo ratings yet
- List of Network Hospital of Medi AssistDocument519 pagesList of Network Hospital of Medi AssistANMOL GOYALNo ratings yet
- LP UapDocument18 pagesLP UapHat MutisalNo ratings yet
- Stricture Urethra in Children: An Indian Perspective: Original ArticleDocument6 pagesStricture Urethra in Children: An Indian Perspective: Original ArticleLilis Endah SulistiyawatiNo ratings yet
- Seminar Presentation On The Topic Rehabilitation CentersDocument13 pagesSeminar Presentation On The Topic Rehabilitation CentersIrshad HussainNo ratings yet
- The Real Effects of Alcohol On The BodyDocument3 pagesThe Real Effects of Alcohol On The BodyJulio AlvesNo ratings yet
- Pinda Thailam Benefits, How To Use, IngredientsDocument2 pagesPinda Thailam Benefits, How To Use, IngredientsRock YasinNo ratings yet
- SEPTICARTHRITISDocument2 pagesSEPTICARTHRITISapi-3822433No ratings yet
- Lower Extremity Arterial Protocol 14 1Document2 pagesLower Extremity Arterial Protocol 14 1api-3494022400% (1)
- Locked in SyndromeDocument52 pagesLocked in SyndromeFarrukh Ali KhanNo ratings yet
- Portfolio Clinical Case Study 3 Lymphoma FinalDocument27 pagesPortfolio Clinical Case Study 3 Lymphoma Finalapi-277136509No ratings yet
- Ultrasonix Sonix Touch BG0526-FDocument4 pagesUltrasonix Sonix Touch BG0526-FvanessaNo ratings yet
- 1NUR8 ABRIO Summative AssessmentDocument3 pages1NUR8 ABRIO Summative AssessmentKYRA CHEYENNE NICHOLLE ABRIO100% (1)
- Lumie Vitamin L User ManualDocument56 pagesLumie Vitamin L User ManualsighsighsighNo ratings yet
- 2021 - NEJM - The Evolving Challenge of Infections in CirrhosisDocument14 pages2021 - NEJM - The Evolving Challenge of Infections in CirrhosisHồ Huy HoàngNo ratings yet
- Special Chemistry: Test Name Current Result Previous Result Unit Normal RangeDocument1 pageSpecial Chemistry: Test Name Current Result Previous Result Unit Normal RangeSyed Muhammad Rafay AhmedNo ratings yet
- Nursing Care in Plastic SurgeryDocument36 pagesNursing Care in Plastic Surgeryjengyee7186No ratings yet
- Afina Fitra Firdaus Ppds Ipd 50Document30 pagesAfina Fitra Firdaus Ppds Ipd 5050Afina Fitra FirdausNo ratings yet
- Triase Nusantara SehatDocument14 pagesTriase Nusantara SehatWidia Nurul AnisaNo ratings yet
- Pregnancy With Prolapse Utery PDFDocument2 pagesPregnancy With Prolapse Utery PDFAnwar Mahnan QomariNo ratings yet
- Curs Hematologie An Feripriva EN Martie 2023 POSTATDocument55 pagesCurs Hematologie An Feripriva EN Martie 2023 POSTATErland BordNo ratings yet
- Garcia NGT NCPDocument1 pageGarcia NGT NCPFrances Katherine GarciaNo ratings yet