Download as pptx, pdf, or txt
You might also like
- Clinical Resolution of Nasal Aspergillosis Following Therapy With A Homeopathic Remedy in A DogDocument6 pagesClinical Resolution of Nasal Aspergillosis Following Therapy With A Homeopathic Remedy in A Dogcrystallynheath0% (1)
- Komposisi Sediaan ParenteralDocument1 pageKomposisi Sediaan ParenteralS Dian RNo ratings yet
- Small For Gestational Age Presentation 3rd Year MedicineDocument19 pagesSmall For Gestational Age Presentation 3rd Year MedicinedotbotNo ratings yet
- Rife FrequenciesDocument12 pagesRife Frequenciesdllabarre100% (1)
- Arterial Line Arterial LineDocument13 pagesArterial Line Arterial LineLinamaria Lozano100% (1)
- TFS Assets - MBD - Brochures - Thermo Scientific Oxoid Disks Brochure Global Non US ENDocument8 pagesTFS Assets - MBD - Brochures - Thermo Scientific Oxoid Disks Brochure Global Non US ENBrahimElkharaziNo ratings yet
- Nejmc 2214302Document3 pagesNejmc 2214302masah al haj aliNo ratings yet
- Antimicrobial / Antifungal Susceptibility TestingDocument6 pagesAntimicrobial / Antifungal Susceptibility TestingKetevan MigriauliNo ratings yet
- Acute Renal Failure: An UpdateDocument52 pagesAcute Renal Failure: An Updatepranav1512No ratings yet
- Dr. Wifanto-Management Liver Metastasis CRCDocument46 pagesDr. Wifanto-Management Liver Metastasis CRCAfkar30No ratings yet
- Amkamxamcampsamazmatmbpc Cfzfep CFM: Sensitivitas Antibiotik Di Rsud Dr. Harjono S PonorogoDocument3 pagesAmkamxamcampsamazmatmbpc Cfzfep CFM: Sensitivitas Antibiotik Di Rsud Dr. Harjono S Ponorogotresna anggaNo ratings yet
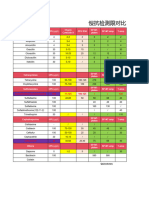
- 副本检测限对比Document7 pages副本检测限对比la9383508No ratings yet
- Saurav Pedicon FinalDocument17 pagesSaurav Pedicon FinalDrSk SamimNo ratings yet
- Ibd TreatmentDocument47 pagesIbd TreatmentM AliNo ratings yet
- Contoh Peta Pola KumanDocument1 pageContoh Peta Pola KumanAgustina Tri SetyaningtyasNo ratings yet
- 2022 Stanford ICU (E2, E29, J2 J4, K4, M4) Gram Neg RodsDocument4 pages2022 Stanford ICU (E2, E29, J2 J4, K4, M4) Gram Neg RodsSUMANT PIRANGINo ratings yet
- Arizona AF AlbersDocument30 pagesArizona AF Albersgiorgi chkholariaNo ratings yet
- Antithrombotic Therapy Stroke Prevention Atrial FibrillationDocument30 pagesAntithrombotic Therapy Stroke Prevention Atrial FibrillationChetan PataliNo ratings yet
- TM 2000-19 PDFDocument22 pagesTM 2000-19 PDFmilecsaNo ratings yet
- CAstV Biochek Slacum WVPA 2017 PDFDocument23 pagesCAstV Biochek Slacum WVPA 2017 PDFJimeno Franscisco de los pozosNo ratings yet
- Pre-Revised and Revised Procedure Charges From Jan 1, 2016Document26 pagesPre-Revised and Revised Procedure Charges From Jan 1, 2016Ashish Singh NegiNo ratings yet
- Juan PaembonanDocument2 pagesJuan Paembonanokegasssss02No ratings yet
- So JuliDocument22 pagesSo Julifarmasi alyaminNo ratings yet
- Alopez Craiva 16 Spindle Cell Tumor UBladderDocument57 pagesAlopez Craiva 16 Spindle Cell Tumor UBladderDima PathNo ratings yet
- Candida Tropicalis - ACMGDocument12 pagesCandida Tropicalis - ACMGSergio Iván López LallanaNo ratings yet
- Bien Dong RobbenDocument4 pagesBien Dong RobbenMai Văn BáchNo ratings yet
- NavelbinDocument48 pagesNavelbinanang atmojoNo ratings yet
- Camaster HRC Fuse Holders: RANGE: 30, 30, 60, and 100 Amp at 600V A.CDocument3 pagesCamaster HRC Fuse Holders: RANGE: 30, 30, 60, and 100 Amp at 600V A.CprekNo ratings yet
- Cobalt-60 Vs LinacDocument33 pagesCobalt-60 Vs LinacAnisza OkseliaNo ratings yet
- New Drugs Under Development in Cardiology: Robert L. Jesse, MD, PHDDocument15 pagesNew Drugs Under Development in Cardiology: Robert L. Jesse, MD, PHDaymenNo ratings yet
- Molecular Mimicry in Innate Immunity:: Structure of A Bacteria TIR Virulence FactorDocument13 pagesMolecular Mimicry in Innate Immunity:: Structure of A Bacteria TIR Virulence Factorjamie pascalNo ratings yet
- AMR PPRA BETHESDA 2017 (DR Hari)Document26 pagesAMR PPRA BETHESDA 2017 (DR Hari)Susi WijayantiNo ratings yet
- Antibiotic Stewardship Congress 2011Document45 pagesAntibiotic Stewardship Congress 2011Az RifkiNo ratings yet
- Bevakalp 07Document10 pagesBevakalp 07Er Prajakta TiwariNo ratings yet
- PocketCard UPDATE2013 EnglishDocument2 pagesPocketCard UPDATE2013 EnglishTowhidulIslamNo ratings yet
- Group Parameter Instrument Parameter Protection Tunnels Based On Quantity - Options Protection Tunnels Based On Concentration - EquitiesDocument10 pagesGroup Parameter Instrument Parameter Protection Tunnels Based On Quantity - Options Protection Tunnels Based On Concentration - EquitiesRodrigo Alves Oliveira Do NascimentoNo ratings yet
- All ProductDocument48 pagesAll ProductVatsavai Appala Narasimha RajuNo ratings yet
- Daftar PerencanaanDocument80 pagesDaftar Perencanaannuri iriyaniNo ratings yet
- Rotem Pocket Guide 2 Page Final cs5Document2 pagesRotem Pocket Guide 2 Page Final cs5Ronei Renato RubboNo ratings yet
- Dispensary Investigation Details - Ramakrishna Math (Yogodyan)Document9 pagesDispensary Investigation Details - Ramakrishna Math (Yogodyan)HIMANSHU KUMAR CHOUDHARYNo ratings yet
- Report - 40204702576 - P SAI TEJADocument4 pagesReport - 40204702576 - P SAI TEJASai GopiNo ratings yet
- Kepekan ICUDocument3 pagesKepekan ICUastrilianaNo ratings yet
- Peta Antibiotika Rsud Bangil Semester Ii 2018 NO. Jenis Antibiotika ResistenDocument2 pagesPeta Antibiotika Rsud Bangil Semester Ii 2018 NO. Jenis Antibiotika Resistenpkpo dktNo ratings yet
- Triatmo Budiyuwono SPJP (K), FIHA, FAPSICDocument40 pagesTriatmo Budiyuwono SPJP (K), FIHA, FAPSICganangahimsaNo ratings yet
- Effect of Silver Nanoparticles and Ions On Oxidative Stress Formation and Antioxidative Machinery of Chlorella VulgarisDocument17 pagesEffect of Silver Nanoparticles and Ions On Oxidative Stress Formation and Antioxidative Machinery of Chlorella VulgarisBrunoNo ratings yet
- Davids Project DataDocument29 pagesDavids Project Dataapi-432035312No ratings yet
- Acb / MCCB / Elcb / Ats MCB / SPD / Ms / MMS: DistributorDocument56 pagesAcb / MCCB / Elcb / Ats MCB / SPD / Ms / MMS: DistributorLUATNo ratings yet
- Acb / MCCB / Elcb / Ats MCB / SPD / Ms / MMS: DistributorDocument54 pagesAcb / MCCB / Elcb / Ats MCB / SPD / Ms / MMS: DistributorC SDNo ratings yet
- Antimicrobial Susceptibility Testing Discs Product List 2020Document2 pagesAntimicrobial Susceptibility Testing Discs Product List 2020midoNo ratings yet
- CMLDocument14 pagesCMLindahflsaragihNo ratings yet
- Mon Tue Wed Thu Fri Employee 13-Nov 14-Nov 15-Nov 16-Nov 17-NovDocument6 pagesMon Tue Wed Thu Fri Employee 13-Nov 14-Nov 15-Nov 16-Nov 17-NovKasun MadusankaNo ratings yet
- Cardiac BiomarkersDocument28 pagesCardiac BiomarkersFaryalBalochNo ratings yet
- 03 - SÀNG LOC QUÝ 2 (Tiếng Anh)Document48 pages03 - SÀNG LOC QUÝ 2 (Tiếng Anh)huyentruonghmNo ratings yet
- Testchart - ColorCardDocument2 pagesTestchart - ColorCardAndre LacerdaNo ratings yet
- Abacus 5 WebDocument4 pagesAbacus 5 WebJOHN JAIRO ANGULONo ratings yet
- Supplementary Table 1. A Full List of Cancer GenesDocument685 pagesSupplementary Table 1. A Full List of Cancer GenesFaruque HossainNo ratings yet
- Usulan Alkes ProvDocument1 pageUsulan Alkes ProvMuhammad IfrahNo ratings yet
- Systemic Therapy For Breast Cancer Adjuvant or NeoadjuvantDocument77 pagesSystemic Therapy For Breast Cancer Adjuvant or NeoadjuvantNada AbdulazizNo ratings yet
- Business PresentationDocument12 pagesBusiness PresentationJays PimentelNo ratings yet
- Prevention of Recurrent Hepatitis B After Liver TransplantationDocument45 pagesPrevention of Recurrent Hepatitis B After Liver TransplantationtasarimkutusuNo ratings yet
- The NAFTA PerspectiveDocument26 pagesThe NAFTA PerspectiveMarcelo Ribeiro100% (1)
- HCC - CCO HepatitisNow2019 HCC SlidesDocument34 pagesHCC - CCO HepatitisNow2019 HCC SlidesMuhammad Javed GabaNo ratings yet
- Multiple Choice Questions for Haematology and Core Medical TraineesFrom EverandMultiple Choice Questions for Haematology and Core Medical TraineesNo ratings yet
- Kode ICD DiagnosaDocument123 pagesKode ICD DiagnosaShita LaubekaNo ratings yet
- Role of The Gut Microbiota in Nutrition and HealthDocument9 pagesRole of The Gut Microbiota in Nutrition and HealthAlejandra Bautista OsorioNo ratings yet
- Encyclopedia of Substance Abuse Prevention, Treatment, & RecoveryDocument3 pagesEncyclopedia of Substance Abuse Prevention, Treatment, & RecoveryAsmaa LabibNo ratings yet
- Listingempannednewlist 04052023Document27 pagesListingempannednewlist 04052023dhawalduvey95No ratings yet
- COPD Flow SheetDocument2 pagesCOPD Flow SheetSachin PillaiNo ratings yet
- 05 Paeds Drug Doses-1Document4 pages05 Paeds Drug Doses-1JunaidahMubarakAliNo ratings yet
- 03 Cutaneous MycosesDocument30 pages03 Cutaneous MycosesFelix AyornuNo ratings yet
- Ozone Ear Insufflation 2Document3 pagesOzone Ear Insufflation 2blackcat54No ratings yet
- English - AFP Investigation Form - Version - 1st - Dec - 2020Document2 pagesEnglish - AFP Investigation Form - Version - 1st - Dec - 2020Tella AdedamolaNo ratings yet
- 10 - ASD, Lord 2018Document53 pages10 - ASD, Lord 2018Grijisha ChandranNo ratings yet
- PAINWeek Journal Vol 7, Q1Document78 pagesPAINWeek Journal Vol 7, Q1Apostolos T.No ratings yet
- Specialize Immunity at Epithelial Barriers and in Immune Privilege TissuesDocument27 pagesSpecialize Immunity at Epithelial Barriers and in Immune Privilege TissuesUmar UsmanNo ratings yet
- Information MSQ KROK 2 Medicine 2007 2020 TraumatologyDocument7 pagesInformation MSQ KROK 2 Medicine 2007 2020 TraumatologyJeet JainNo ratings yet
- Priorty Indirect Inguinal Left Hernia Case PreDocument47 pagesPriorty Indirect Inguinal Left Hernia Case Prejbvaldez100% (1)
- Overview of pediatric nursing الباب الاولDocument2 pagesOverview of pediatric nursing الباب الاولmathio medhatNo ratings yet
- Manipulação 60 114Document55 pagesManipulação 60 114Zilmar OliveiraNo ratings yet
- Seldinger ModifiedseldingerDocument6 pagesSeldinger ModifiedseldingerThiago BañosNo ratings yet
- Group Collaborative Activity TaskonomyDocument2 pagesGroup Collaborative Activity TaskonomyTweeky SaureNo ratings yet
- Bhopal GasDocument22 pagesBhopal GasBijay Kumar MahatoNo ratings yet
- Controversiesin Anesthesiafororaland Maxillofacialsurgery: Brett J. King,, Adam LevineDocument9 pagesControversiesin Anesthesiafororaland Maxillofacialsurgery: Brett J. King,, Adam LevineAB MISHRANo ratings yet
- RopDocument364 pagesRopIeie MawonNo ratings yet
- Extensor Tendon Fingers Norwich Guideline 2018Document2 pagesExtensor Tendon Fingers Norwich Guideline 2018Ariana Iorga100% (1)
- (For MGH Patients Only) : IV SolutionDocument1 page(For MGH Patients Only) : IV SolutionampalNo ratings yet
- Working As A Team in Airway Surgery History Pres 2021 Seminars in PediatriDocument6 pagesWorking As A Team in Airway Surgery History Pres 2021 Seminars in PediatriSavaNo ratings yet
- 1St Experience With Robotic Thymectomy in Kauh: Iskender Algithmi, MD Ragab Shehata, McsDocument44 pages1St Experience With Robotic Thymectomy in Kauh: Iskender Algithmi, MD Ragab Shehata, Mcsopen-heart-604No ratings yet
- 1000 Plus Psychiatry MCQ Book DranilkakunjeDocument141 pages1000 Plus Psychiatry MCQ Book Dranilkakunjethelegend 20220% (1)