Download as pptx, pdf, or txt
You might also like
- Ebook PDF Current Medical Diagnosis and Treatment Study Guide 2nd PDFDocument41 pagesEbook PDF Current Medical Diagnosis and Treatment Study Guide 2nd PDFcecil.slocum194100% (49)
- 101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinDocument17 pages101 Things I Wish I'd Known When I Started Using Hypnosis: Dabney EwinFilipeCarvalho100% (7)
- 11 DermatitisDocument39 pages11 DermatitisLQYNo ratings yet
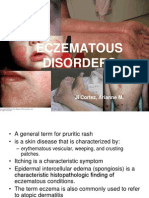
- Eczematous Disorders CFM REPORT 2Document32 pagesEczematous Disorders CFM REPORT 2Arianne CortezNo ratings yet
- WEEK 6 Skin DisorderDocument37 pagesWEEK 6 Skin DisorderRaghad NaifNo ratings yet
- Skin Diseases Presentation2Document40 pagesSkin Diseases Presentation2DaniTadeNo ratings yet
- DermatitisDocument46 pagesDermatitisAaditya IndoliaNo ratings yet
- DermatitisDocument46 pagesDermatitisHadi AbdulhadiNo ratings yet
- 2 EczemaDocument5 pages2 Eczemaحسين طاهر حاتم طاهرNo ratings yet
- Skin DisordersDocument202 pagesSkin DisordersMj Briones100% (1)
- Skin Conditions Part II-1Document54 pagesSkin Conditions Part II-1mohamedkallon1996No ratings yet
- Scabies and ImpetigoDocument13 pagesScabies and ImpetigoValabhoju Bindu MadhaviNo ratings yet
- Eczema & Psoriasis: Dr. MburuDocument69 pagesEczema & Psoriasis: Dr. MburuKeith OmwoyoNo ratings yet
- EczemaDocument19 pagesEczemaAiman TymerNo ratings yet
- Dermatitis: Maria Soleil Bernadette M. MalonzoDocument29 pagesDermatitis: Maria Soleil Bernadette M. MalonzoMacey MalonzoNo ratings yet
- Atopic Dermatitis: Aaron Justin D. TingzonDocument23 pagesAtopic Dermatitis: Aaron Justin D. TingzonChi SamaniegoNo ratings yet
- Inflammatory Skin DiseaseDocument32 pagesInflammatory Skin Diseaseragnarok meroNo ratings yet
- Atopic DermatitisDocument43 pagesAtopic DermatitisSaurav Arora100% (2)
- Overview of Skin InfectionsDocument53 pagesOverview of Skin Infectionsadamu mohammadNo ratings yet
- Eczema, UrticariaDocument72 pagesEczema, Urticariaamberwinthrop100% (1)
- Dermatology Cutaneous Bacterial InfectionsDocument139 pagesDermatology Cutaneous Bacterial InfectionsArianne Joy C. TamarayNo ratings yet
- Dermatology 3Document24 pagesDermatology 3حسين طاهر حاتم طاهرNo ratings yet
- Overview Common Dermatologic Problems in ChildrenDocument26 pagesOverview Common Dermatologic Problems in Childrenokwadha simionNo ratings yet
- Dermatology ReVIsION.Document8 pagesDermatology ReVIsION.Aadan BilowNo ratings yet
- Eczema: Pathogenesis. Atopic Dermatitis Depends On A Complex Interaction BetweenDocument5 pagesEczema: Pathogenesis. Atopic Dermatitis Depends On A Complex Interaction BetweenSuhas IngaleNo ratings yet
- Bacterial - Viral InfectionsDocument61 pagesBacterial - Viral InfectionsMoayad NawaflehNo ratings yet
- Dermatology 2Document22 pagesDermatology 2Md. Golam MostofaNo ratings yet
- Dermatitis: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocument30 pagesDermatitis: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityMuhammad mukramNo ratings yet
- Skin Diseases: Acne Vulgaris Allergic DermatitisDocument32 pagesSkin Diseases: Acne Vulgaris Allergic DermatitisJuma SammyNo ratings yet
- l9 - Neoplastic - Non-Neoplastic Skin DisordersDocument69 pagesl9 - Neoplastic - Non-Neoplastic Skin DisordersVenniilaaSaravananNo ratings yet
- Session 21 EczemaDocument23 pagesSession 21 Eczemadreampurpose97No ratings yet
- Dermatitis 1-2023Document20 pagesDermatitis 1-2023Maryam ElammaryNo ratings yet
- Dermatology Primer: Selected Skin Diseases and Treatment Tailored For The Athletic TrainerDocument64 pagesDermatology Primer: Selected Skin Diseases and Treatment Tailored For The Athletic TrainerSilviu100% (1)
- Bullous Disorders, Bacterial and Fungal Skin InfectionsDocument95 pagesBullous Disorders, Bacterial and Fungal Skin InfectionsDeborah ChemutaiNo ratings yet
- Dermatitis DR Citra 260907Document56 pagesDermatitis DR Citra 260907Adam AriwibawaNo ratings yet
- Dermatitis Numularis and NeurodermatitisDocument22 pagesDermatitis Numularis and NeurodermatitisNura ReefaNo ratings yet
- Reactive Disorders of The SkinDocument46 pagesReactive Disorders of The SkinhaniNo ratings yet
- Dermatitis and Eczema: Ailing Zou (邹爱玲) 2021.10.18Document31 pagesDermatitis and Eczema: Ailing Zou (邹爱玲) 2021.10.18AmeliaNo ratings yet
- Jurnal Tinea CorporisDocument19 pagesJurnal Tinea CorporisRahma TomuNo ratings yet
- Dermatitis Eksematosa - Dr. Kristo A. Nababan, Sp. KKDocument91 pagesDermatitis Eksematosa - Dr. Kristo A. Nababan, Sp. KKJhost Clinton PurbaNo ratings yet
- Reactive Erythemas and VasculitisDocument51 pagesReactive Erythemas and VasculitisMoayad NawaflehNo ratings yet
- Dr. R. Sekhon - Dermatology Telehealth Jan 27 MRDocument45 pagesDr. R. Sekhon - Dermatology Telehealth Jan 27 MRAnissa ADNo ratings yet
- 1 - Facial Dermatoses and Hair Disorders - 2023Document87 pages1 - Facial Dermatoses and Hair Disorders - 2023mesexel246No ratings yet
- DermatitisDocument44 pagesDermatitisAyuMardewi50% (2)
- DermatitisDocument61 pagesDermatitisAlex XanderNo ratings yet
- Dermatology in 2hrsDocument222 pagesDermatology in 2hrslarisaP100% (4)
- Dermatology Eczema: Click To Edit Master Subtitle StyleDocument19 pagesDermatology Eczema: Click To Edit Master Subtitle StyleAiman Tymer100% (1)
- Derma ADDocument49 pagesDerma ADFatima Marwa Teo MaghinayNo ratings yet
- Kuliah SMTR VDocument117 pagesKuliah SMTR VHorakhty PrideNo ratings yet
- Skin and BurnDocument52 pagesSkin and Burniifatmax20No ratings yet
- 6435 SOAP NOTE Presentation Atopic DermatitisDocument21 pages6435 SOAP NOTE Presentation Atopic DermatitisMelinda Powell100% (2)
- Acute Inflammatory DermatosesDocument29 pagesAcute Inflammatory DermatosesHaniya KhanNo ratings yet
- DermatitisDocument3 pagesDermatitisMaytham AbasNo ratings yet
- Adebola Ogunbiyi, FMCP, FWACP, FRCP, FNAMED UCH, IbadanDocument63 pagesAdebola Ogunbiyi, FMCP, FWACP, FRCP, FNAMED UCH, Ibadanadamu mohammadNo ratings yet
- Assalamu'alikum WR WB: Harijono KariosentonoDocument59 pagesAssalamu'alikum WR WB: Harijono KariosentonoDhiastikaNo ratings yet
- DddsDocument50 pagesDddsOsama AlhaseNo ratings yet
- Skin Diseases PresentationDocument23 pagesSkin Diseases PresentationDaniTadeNo ratings yet
- Skin and Soft Tissue Infectons 1Document51 pagesSkin and Soft Tissue Infectons 1AISHWARYA T DNo ratings yet
- NTU Skin Pathology 2024Document75 pagesNTU Skin Pathology 2024Chen HouyuNo ratings yet
- Complete Medical Guide for Disease Volume VII; Atopic DermatitisFrom EverandComplete Medical Guide for Disease Volume VII; Atopic DermatitisNo ratings yet
- DKA Uganda August 2023Document35 pagesDKA Uganda August 2023Deborah ChemutaiNo ratings yet
- Year 3 Courses - Semester I & 2 - MBCHBDocument14 pagesYear 3 Courses - Semester I & 2 - MBCHBDeborah ChemutaiNo ratings yet
- FUMSA GA Concept Draft JONATHANDocument7 pagesFUMSA GA Concept Draft JONATHANDeborah ChemutaiNo ratings yet
- Year 1 Semester 1 - 2021 Timetable Final VersionDocument12 pagesYear 1 Semester 1 - 2021 Timetable Final VersionDeborah ChemutaiNo ratings yet
- Doctor Patient Relationship Muk March 2021Document28 pagesDoctor Patient Relationship Muk March 2021Deborah Chemutai100% (1)
- First Aid Training Wagagai Company 2011Document153 pagesFirst Aid Training Wagagai Company 2011Deborah ChemutaiNo ratings yet
- Gene Expression - May 7 2021 MakCHS (Compatibility Mode)Document20 pagesGene Expression - May 7 2021 MakCHS (Compatibility Mode)Deborah ChemutaiNo ratings yet
- Practical Timeline SEM II TRUNK-0Document1 pagePractical Timeline SEM II TRUNK-0Deborah ChemutaiNo ratings yet
- Exam 4KEY - 2016Document13 pagesExam 4KEY - 2016Deborah ChemutaiNo ratings yet
- 35148753Document134 pages35148753Deborah ChemutaiNo ratings yet
- District: Palisa District: S/N School Specific Findings RecommendationsDocument2 pagesDistrict: Palisa District: S/N School Specific Findings RecommendationsDeborah ChemutaiNo ratings yet
- Transcription Is A Cellular Process During Which RNA Is SynthesizedDocument7 pagesTranscription Is A Cellular Process During Which RNA Is SynthesizedDeborah ChemutaiNo ratings yet
- The Checklist - A Tool For Error Management and Performance ImprovementDocument5 pagesThe Checklist - A Tool For Error Management and Performance ImprovementGustavo Catalan RuzaNo ratings yet
- PKC AryanDocument62 pagesPKC AryanAryan PurohitNo ratings yet
- WHO EURO 2023 8280 48052 71230 EngDocument36 pagesWHO EURO 2023 8280 48052 71230 Engcarolerousseau72No ratings yet
- Emedica MRCGP AKT Curriculum ChecklistDocument42 pagesEmedica MRCGP AKT Curriculum ChecklistSana Mustafa100% (1)
- Handouts in Special and Inclusive EducationDocument2 pagesHandouts in Special and Inclusive EducationRex EvangelistaNo ratings yet
- Esophageal Cancer NewDocument52 pagesEsophageal Cancer Newapi-282115150No ratings yet
- Probiotics, Prebiotics and Synbiotics - A ReviewDocument12 pagesProbiotics, Prebiotics and Synbiotics - A ReviewluthfikhairulNo ratings yet
- 342 FullDocument9 pages342 FulldrdevvratNo ratings yet
- HISTORY TAKING AND PE OF CARDIAC PATIENTS. Original.Document69 pagesHISTORY TAKING AND PE OF CARDIAC PATIENTS. Original.api-3858544No ratings yet
- International Journal of Pediatric Research Ijpr 7 073Document9 pagesInternational Journal of Pediatric Research Ijpr 7 073Paul AsrNo ratings yet
- Staining Abnormalities of Dermal Collagen in Eosinophil - or Neutrophil-Rich Inflammatory Dermatoses of Horses and Cats As DemonstrateDocument6 pagesStaining Abnormalities of Dermal Collagen in Eosinophil - or Neutrophil-Rich Inflammatory Dermatoses of Horses and Cats As DemonstratejenNo ratings yet
- What Are DrugsDocument7 pagesWhat Are DrugsMelvin Jay Reyes BaluranNo ratings yet
- CLR 12021Document63 pagesCLR 12021Eliza DNNo ratings yet
- AREVIEWONHIVAIDSDocument6 pagesAREVIEWONHIVAIDSanthonybolteyNo ratings yet
- Blood Gases and Acid-Base BalanceDocument11 pagesBlood Gases and Acid-Base BalanceREMAN ALINGASANo ratings yet
- PT - Tri Sapta Jaya: Pt. Kalbe Farma KF Nimitz Non ParetoDocument22 pagesPT - Tri Sapta Jaya: Pt. Kalbe Farma KF Nimitz Non ParetoVanny Swantika Minanda AlsiNo ratings yet
- Microvascular Decompression As A Surgical Management For Trigeminal Neuralgia: Long-Term Follow-Up and Review of The LiteratureDocument8 pagesMicrovascular Decompression As A Surgical Management For Trigeminal Neuralgia: Long-Term Follow-Up and Review of The LiteratureAkmal Niam FirdausiNo ratings yet
- BronchopneumoniaDocument11 pagesBronchopneumoniaDesiree GuerraNo ratings yet
- Lung Disease: PneumoniaDocument2 pagesLung Disease: Pneumoniacayla mae carlosNo ratings yet
- Knust Lect Infectious Disease IDocument8 pagesKnust Lect Infectious Disease IAnastasiafynnNo ratings yet
- Cord Blood Fees Waste of MoneyDocument2 pagesCord Blood Fees Waste of Moneyapi-223713414No ratings yet
- Fusidic Acid - Wikipedia, The Free EncyclopediaDocument6 pagesFusidic Acid - Wikipedia, The Free EncyclopediaAnkan PalNo ratings yet
- StrokePassiveRangeMotionHemiplegicArm TRHDocument4 pagesStrokePassiveRangeMotionHemiplegicArm TRHAmy BrownNo ratings yet
- YCYSt DocumentDocument24 pagesYCYSt DocumentDodo AlsunaidiNo ratings yet
- CO4 HealthDocument3 pagesCO4 HealthJennelyn Orilla Brezo - Arcosiba100% (2)
- Dress Syndrome A Review and UpdateDocument5 pagesDress Syndrome A Review and UpdateCarlos Alberto Torres LópezNo ratings yet
- "Azithromycin": Bachelor of PharmacyDocument36 pages"Azithromycin": Bachelor of Pharmacydeepak_143No ratings yet
- Vakcinacija U Nemackoj Germany Ip VakcinaDocument3 pagesVakcinacija U Nemackoj Germany Ip VakcinaNikola IvankovicNo ratings yet
- Fowl Cholera in ChickensDocument17 pagesFowl Cholera in ChickensŠhâh NawazNo ratings yet