
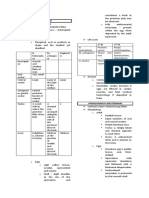
Ciliates & Sporozoa
Ciliates & Sporozoa
You might also like
- Pathology of NoaDocument164 pagesPathology of NoaAnonymous milwFDXNo ratings yet
- Immuno Virology BacteriologyDocument309 pagesImmuno Virology BacteriologyJulianna MacintyreNo ratings yet
- Parasitology DoneDocument5 pagesParasitology DoneShawn Gaurav Jha100% (2)
- Electronic Atlas of ParasitologyDocument650 pagesElectronic Atlas of Parasitologystormyccs100% (7)
- ApicomplexaDocument47 pagesApicomplexaJosh BernalNo ratings yet
- Module 7 - Protozoans (Flagellates and Ciliates)Document75 pagesModule 7 - Protozoans (Flagellates and Ciliates)Arnold GarcinesNo ratings yet
- (PROTOZOANS) Phylum ApicomplexaDocument8 pages(PROTOZOANS) Phylum ApicomplexaEunice AndradeNo ratings yet
- The Digestive System: and ItsDocument102 pagesThe Digestive System: and ItsRhea Andrea Uy100% (1)
- Electrolyte Disorders: David Minter, DO, F.A.C.O.IDocument102 pagesElectrolyte Disorders: David Minter, DO, F.A.C.O.INabeel Shahzad100% (1)
- Protozoans - Ciliates and FlagellatesDocument80 pagesProtozoans - Ciliates and FlagellatesfsdafvNo ratings yet
- ProtozoansDocument2 pagesProtozoansJonathanPayongayongNo ratings yet
- Protista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Document6 pagesProtista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Primo GeorgeNo ratings yet
- C19 2 Hemopoiesis Eythropoiesis LeukopoiesisDocument11 pagesC19 2 Hemopoiesis Eythropoiesis Leukopoiesisnurul azisyah auraNo ratings yet
- Leukocytes, Granulocytes, The Monocyte-Macrophage System, and InflammationDocument10 pagesLeukocytes, Granulocytes, The Monocyte-Macrophage System, and InflammationShi no MeNo ratings yet
- Lec 1 - IntroductionDocument3 pagesLec 1 - IntroductionHaendra Mae DapilagaNo ratings yet
- Heterophyid: ST NDDocument3 pagesHeterophyid: ST NDIvan ChuaNo ratings yet
- Midterm Chapter7Document43 pagesMidterm Chapter7Frances FranciscoNo ratings yet
- APP2 E1 NoteDocument28 pagesAPP2 E1 NotelifecostNo ratings yet
- Lesson 3Document71 pagesLesson 3Angel joyce ValenciaNo ratings yet
- Staphylococcus LectureDocument66 pagesStaphylococcus LectureFarhan Azmain FahimNo ratings yet
- Week 1 Renal Physiology and Intro To Urinalysis (Lecture)Document4 pagesWeek 1 Renal Physiology and Intro To Urinalysis (Lecture)Dayledaniel Sorveto100% (1)
- Kinds of Blood CellDocument3 pagesKinds of Blood CellBalkis HumairohNo ratings yet
- Anat 4.3 GIT Histo - ZuluetaDocument8 pagesAnat 4.3 GIT Histo - Zuluetalovelots1234No ratings yet
- Protozoans Lecture AmoebaDocument42 pagesProtozoans Lecture Amoebablue_blooded23100% (1)
- Bacteria - Morphology & ClassificationDocument38 pagesBacteria - Morphology & ClassificationAfshan NasirNo ratings yet
- Cestodes and TrematodesDocument48 pagesCestodes and TrematodesFort SalvadorNo ratings yet
- Polyomavirus LectureDocument60 pagesPolyomavirus Lecturerggefrm75% (4)
- Parasitic AmoebaDocument23 pagesParasitic AmoebaJethrö MallariNo ratings yet
- VirologyDocument9 pagesVirologyAnisha SarmaNo ratings yet
- Genus Staphylococcus: Characteristic S.epidermidis S.saprophyticusDocument5 pagesGenus Staphylococcus: Characteristic S.epidermidis S.saprophyticusxxdrivexxNo ratings yet
- Syphilis: Michelle LinardiDocument20 pagesSyphilis: Michelle Linardimichelle95No ratings yet
- What Is CoagulationDocument6 pagesWhat Is CoagulationKang Wenn LeeNo ratings yet
- Hema I Chapter 4 - AnticoagDocument16 pagesHema I Chapter 4 - AnticoagderibewNo ratings yet
- Entamoeba SPPDocument21 pagesEntamoeba SPPragnabulletinNo ratings yet
- 3 Year CPC October 8, 20202Document4 pages3 Year CPC October 8, 20202Raian SuyuNo ratings yet
- Microscopic Morphology Myocardial InfarctionDocument10 pagesMicroscopic Morphology Myocardial InfarctionnathanielNo ratings yet
- Topic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsDocument6 pagesTopic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsJhunrick Corpuz TumpalanNo ratings yet
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- Screening Test For Phagocytic Engulfment: DiapedesisDocument2 pagesScreening Test For Phagocytic Engulfment: DiapedesisBianca ANo ratings yet
- 1.structure of BacteriaDocument12 pages1.structure of BacteriaDr P N N ReddyNo ratings yet
- Chapter 9 The Immune System NotesDocument8 pagesChapter 9 The Immune System NotesFelix LeNo ratings yet
- Pathology 1st Practical ExamDocument101 pagesPathology 1st Practical Examjeffrey_co_1No ratings yet
- Cestodes PDFDocument171 pagesCestodes PDFsummer djNo ratings yet
- Trichuriasis: Disease Type: Parasitic Disease Common Name: Causative Agent: Species of Trichuris Disease DiscriptionDocument9 pagesTrichuriasis: Disease Type: Parasitic Disease Common Name: Causative Agent: Species of Trichuris Disease DiscriptionBrijesh Singh YadavNo ratings yet
- Submitted By: Group 6 MT 3BDocument49 pagesSubmitted By: Group 6 MT 3BChristine Joy TanglaoNo ratings yet
- Presented by T. V. L. Sahithi Ist Year PG Dept of PeriodonticsDocument49 pagesPresented by T. V. L. Sahithi Ist Year PG Dept of Periodonticslakshmi sahithi natakalaNo ratings yet
- Acute Inflammation 2Document33 pagesAcute Inflammation 2The MedicalNo ratings yet
- 07 Pathological ClacificationDocument10 pages07 Pathological Clacificationraanja2No ratings yet
- RMTnotes PARASITOLOGYDocument68 pagesRMTnotes PARASITOLOGYArvin O-CaféNo ratings yet
- Haematological MalignanciesDocument63 pagesHaematological MalignanciesIsaac MwangiNo ratings yet
- EDs Basic Histology PDFDocument208 pagesEDs Basic Histology PDFTemesgen Endalew0% (1)
- Physiology Summary Chapter 33Document5 pagesPhysiology Summary Chapter 33gail018100% (1)
- Clin Path Trans 3.05 Urinalysis (2b)Document6 pagesClin Path Trans 3.05 Urinalysis (2b)Reymart FernandezNo ratings yet
- ENTEROBACTERIACEAEDocument13 pagesENTEROBACTERIACEAEStephen Jao Ayala Ujano100% (1)
- Blood Cells and The Hematopoetic SystemDocument53 pagesBlood Cells and The Hematopoetic SystemMeet RandhawaNo ratings yet
- Patho Final Study GuideDocument55 pagesPatho Final Study GuideBritNo ratings yet
- IS LessonDocument30 pagesIS Lessonjohn dale duranoNo ratings yet
- Virology - S1: Abbas Adel Group 4Document38 pagesVirology - S1: Abbas Adel Group 4William BufNo ratings yet
- Quantitative and Qualitative Disorders of WBCsDocument9 pagesQuantitative and Qualitative Disorders of WBCsOliver BarnyakNo ratings yet
- Subcutaneous & Systemic MycosesDocument7 pagesSubcutaneous & Systemic MycosesDee GeeNo ratings yet
- Proceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964From EverandProceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964Augusto CorradettiNo ratings yet
- Chapter 8Document53 pagesChapter 8contactrafiakhuramNo ratings yet
- Parasitology-Lec 13 MalariaDocument6 pagesParasitology-Lec 13 Malariaapi-3743217No ratings yet
- Protozoan Maricelle ManlutacDocument53 pagesProtozoan Maricelle ManlutacGlanela ManalotoNo ratings yet
- MicroPara Viro Questions by ApollonDocument13 pagesMicroPara Viro Questions by ApollonAngelo MercedeNo ratings yet
- Protist GuideDocument30 pagesProtist GuidemavicarigoreNo ratings yet
- Malaria Research in IndiaDocument8 pagesMalaria Research in IndiaPradeepNo ratings yet
- Methods in MalariaDocument351 pagesMethods in Malariakel910No ratings yet
- Plasmodium VivaxDocument4 pagesPlasmodium VivaxSUTHAN100% (1)
- Malaria 25 03 09Document131 pagesMalaria 25 03 09Dr.Jagadish Nuchina100% (5)
- Biology - Unit 4 Kingdom ProtistaDocument0 pagesBiology - Unit 4 Kingdom Protistawww.bhawesh.com.npNo ratings yet
- S Porozoa Plasmodium: Scientific Name: Plasmodium Higher Classification: PlasmodiidaeDocument8 pagesS Porozoa Plasmodium: Scientific Name: Plasmodium Higher Classification: PlasmodiidaeRhodaOriginalNo ratings yet
- Wbjee 2012 Biology Question PaperDocument8 pagesWbjee 2012 Biology Question Papersaurav guptaNo ratings yet
- Organism Staining OsceDocument105 pagesOrganism Staining OsceNachchakorn DellNo ratings yet
- Textbook Microbial Control of Vector Borne Diseases 1St Edition Brij Kishore Tyagi Ebook All Chapter PDFDocument53 pagesTextbook Microbial Control of Vector Borne Diseases 1St Edition Brij Kishore Tyagi Ebook All Chapter PDFjohn.saenz973100% (10)
- Literature Review On Malaria PDFDocument7 pagesLiterature Review On Malaria PDFaflsqyljm100% (1)
- Jornal Inggris 5Document7 pagesJornal Inggris 5putra aryaNo ratings yet
- Malaria Journal: Computer Vision For Microscopy Diagnosis of MalariaDocument14 pagesMalaria Journal: Computer Vision For Microscopy Diagnosis of MalariaDaniel Alfredo Galindo ChoqueNo ratings yet
- Group 3: Widia Yuni Pratiwi Sari Saiba Ningrum Ni Putu Rika Fadlunnisa Tiya MutiaraDocument12 pagesGroup 3: Widia Yuni Pratiwi Sari Saiba Ningrum Ni Putu Rika Fadlunnisa Tiya MutiaraWidia YuniNo ratings yet
- Malaria Situation in India: Dr. Neeraj Dhingra Additional Director & Head Malaria Division, NVBDCP Dghs Mohfw IndiaDocument21 pagesMalaria Situation in India: Dr. Neeraj Dhingra Additional Director & Head Malaria Division, NVBDCP Dghs Mohfw IndiaMJ SolNo ratings yet
- Helping Tapan RRB Je GS MCQ PDFDocument318 pagesHelping Tapan RRB Je GS MCQ PDFPoonam TripathiNo ratings yet
- 12Document72 pages12Malik RohailNo ratings yet
- MalariaDocument5 pagesMalariaRina KhazarenNo ratings yet
- Biology Notes Chap: 2Document4 pagesBiology Notes Chap: 2R.S.H82% (11)
- List of On-Roll Ph.D. Scholars at Thapar University, Patiala As On 29.06.2017Document18 pagesList of On-Roll Ph.D. Scholars at Thapar University, Patiala As On 29.06.2017SumanNo ratings yet
- What Causes Malaria?Document8 pagesWhat Causes Malaria?Dulce M. LupaseNo ratings yet
- AGBODEKA ET AL (3) - 2017 - Activité Antiplasmodiale Des Plantes Médicinales D'afrique de L'ouest Revue de La LitteratureDocument9 pagesAGBODEKA ET AL (3) - 2017 - Activité Antiplasmodiale Des Plantes Médicinales D'afrique de L'ouest Revue de La LitteratureGBEKLEYNo ratings yet
- Malaria Identification It Is Easier Than You Think!: Susan Flaker Johnson, MT (ASCP), MEPDDocument30 pagesMalaria Identification It Is Easier Than You Think!: Susan Flaker Johnson, MT (ASCP), MEPDasclswisconsinNo ratings yet
- Malaria Treatment Guidelines WHO 2010Document211 pagesMalaria Treatment Guidelines WHO 2010emc27No ratings yet
- Malaria Must Go (Satb)Document7 pagesMalaria Must Go (Satb)Mubiru DavidNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- Pathology of NoaDocument164 pagesPathology of NoaAnonymous milwFDXNo ratings yet
- Immuno Virology BacteriologyDocument309 pagesImmuno Virology BacteriologyJulianna MacintyreNo ratings yet
- Parasitology DoneDocument5 pagesParasitology DoneShawn Gaurav Jha100% (2)
- Electronic Atlas of ParasitologyDocument650 pagesElectronic Atlas of Parasitologystormyccs100% (7)
- ApicomplexaDocument47 pagesApicomplexaJosh BernalNo ratings yet
- Module 7 - Protozoans (Flagellates and Ciliates)Document75 pagesModule 7 - Protozoans (Flagellates and Ciliates)Arnold GarcinesNo ratings yet
- (PROTOZOANS) Phylum ApicomplexaDocument8 pages(PROTOZOANS) Phylum ApicomplexaEunice AndradeNo ratings yet
- The Digestive System: and ItsDocument102 pagesThe Digestive System: and ItsRhea Andrea Uy100% (1)
- Electrolyte Disorders: David Minter, DO, F.A.C.O.IDocument102 pagesElectrolyte Disorders: David Minter, DO, F.A.C.O.INabeel Shahzad100% (1)
- Protozoans - Ciliates and FlagellatesDocument80 pagesProtozoans - Ciliates and FlagellatesfsdafvNo ratings yet
- ProtozoansDocument2 pagesProtozoansJonathanPayongayongNo ratings yet
- Protista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Document6 pagesProtista (Subdivision Protozoa) : Bütschlii), or Pathogenic (E. Histolytica)Primo GeorgeNo ratings yet
- C19 2 Hemopoiesis Eythropoiesis LeukopoiesisDocument11 pagesC19 2 Hemopoiesis Eythropoiesis Leukopoiesisnurul azisyah auraNo ratings yet
- Leukocytes, Granulocytes, The Monocyte-Macrophage System, and InflammationDocument10 pagesLeukocytes, Granulocytes, The Monocyte-Macrophage System, and InflammationShi no MeNo ratings yet
- Lec 1 - IntroductionDocument3 pagesLec 1 - IntroductionHaendra Mae DapilagaNo ratings yet
- Heterophyid: ST NDDocument3 pagesHeterophyid: ST NDIvan ChuaNo ratings yet
- Midterm Chapter7Document43 pagesMidterm Chapter7Frances FranciscoNo ratings yet
- APP2 E1 NoteDocument28 pagesAPP2 E1 NotelifecostNo ratings yet
- Lesson 3Document71 pagesLesson 3Angel joyce ValenciaNo ratings yet
- Staphylococcus LectureDocument66 pagesStaphylococcus LectureFarhan Azmain FahimNo ratings yet
- Week 1 Renal Physiology and Intro To Urinalysis (Lecture)Document4 pagesWeek 1 Renal Physiology and Intro To Urinalysis (Lecture)Dayledaniel Sorveto100% (1)
- Kinds of Blood CellDocument3 pagesKinds of Blood CellBalkis HumairohNo ratings yet
- Anat 4.3 GIT Histo - ZuluetaDocument8 pagesAnat 4.3 GIT Histo - Zuluetalovelots1234No ratings yet
- Protozoans Lecture AmoebaDocument42 pagesProtozoans Lecture Amoebablue_blooded23100% (1)
- Bacteria - Morphology & ClassificationDocument38 pagesBacteria - Morphology & ClassificationAfshan NasirNo ratings yet
- Cestodes and TrematodesDocument48 pagesCestodes and TrematodesFort SalvadorNo ratings yet
- Polyomavirus LectureDocument60 pagesPolyomavirus Lecturerggefrm75% (4)
- Parasitic AmoebaDocument23 pagesParasitic AmoebaJethrö MallariNo ratings yet
- VirologyDocument9 pagesVirologyAnisha SarmaNo ratings yet
- Genus Staphylococcus: Characteristic S.epidermidis S.saprophyticusDocument5 pagesGenus Staphylococcus: Characteristic S.epidermidis S.saprophyticusxxdrivexxNo ratings yet
- Syphilis: Michelle LinardiDocument20 pagesSyphilis: Michelle Linardimichelle95No ratings yet
- What Is CoagulationDocument6 pagesWhat Is CoagulationKang Wenn LeeNo ratings yet
- Hema I Chapter 4 - AnticoagDocument16 pagesHema I Chapter 4 - AnticoagderibewNo ratings yet
- Entamoeba SPPDocument21 pagesEntamoeba SPPragnabulletinNo ratings yet
- 3 Year CPC October 8, 20202Document4 pages3 Year CPC October 8, 20202Raian SuyuNo ratings yet
- Microscopic Morphology Myocardial InfarctionDocument10 pagesMicroscopic Morphology Myocardial InfarctionnathanielNo ratings yet
- Topic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsDocument6 pagesTopic Outline: Elements of Parasitology (3P's) Types of Association of Living OrganismsJhunrick Corpuz TumpalanNo ratings yet
- Abdominal AbscessDocument3 pagesAbdominal AbscessIchalAzNo ratings yet
- Screening Test For Phagocytic Engulfment: DiapedesisDocument2 pagesScreening Test For Phagocytic Engulfment: DiapedesisBianca ANo ratings yet
- 1.structure of BacteriaDocument12 pages1.structure of BacteriaDr P N N ReddyNo ratings yet
- Chapter 9 The Immune System NotesDocument8 pagesChapter 9 The Immune System NotesFelix LeNo ratings yet
- Pathology 1st Practical ExamDocument101 pagesPathology 1st Practical Examjeffrey_co_1No ratings yet
- Cestodes PDFDocument171 pagesCestodes PDFsummer djNo ratings yet
- Trichuriasis: Disease Type: Parasitic Disease Common Name: Causative Agent: Species of Trichuris Disease DiscriptionDocument9 pagesTrichuriasis: Disease Type: Parasitic Disease Common Name: Causative Agent: Species of Trichuris Disease DiscriptionBrijesh Singh YadavNo ratings yet
- Submitted By: Group 6 MT 3BDocument49 pagesSubmitted By: Group 6 MT 3BChristine Joy TanglaoNo ratings yet
- Presented by T. V. L. Sahithi Ist Year PG Dept of PeriodonticsDocument49 pagesPresented by T. V. L. Sahithi Ist Year PG Dept of Periodonticslakshmi sahithi natakalaNo ratings yet
- Acute Inflammation 2Document33 pagesAcute Inflammation 2The MedicalNo ratings yet
- 07 Pathological ClacificationDocument10 pages07 Pathological Clacificationraanja2No ratings yet
- RMTnotes PARASITOLOGYDocument68 pagesRMTnotes PARASITOLOGYArvin O-CaféNo ratings yet
- Haematological MalignanciesDocument63 pagesHaematological MalignanciesIsaac MwangiNo ratings yet
- EDs Basic Histology PDFDocument208 pagesEDs Basic Histology PDFTemesgen Endalew0% (1)
- Physiology Summary Chapter 33Document5 pagesPhysiology Summary Chapter 33gail018100% (1)
- Clin Path Trans 3.05 Urinalysis (2b)Document6 pagesClin Path Trans 3.05 Urinalysis (2b)Reymart FernandezNo ratings yet
- ENTEROBACTERIACEAEDocument13 pagesENTEROBACTERIACEAEStephen Jao Ayala Ujano100% (1)
- Blood Cells and The Hematopoetic SystemDocument53 pagesBlood Cells and The Hematopoetic SystemMeet RandhawaNo ratings yet
- Patho Final Study GuideDocument55 pagesPatho Final Study GuideBritNo ratings yet
- IS LessonDocument30 pagesIS Lessonjohn dale duranoNo ratings yet
- Virology - S1: Abbas Adel Group 4Document38 pagesVirology - S1: Abbas Adel Group 4William BufNo ratings yet
- Quantitative and Qualitative Disorders of WBCsDocument9 pagesQuantitative and Qualitative Disorders of WBCsOliver BarnyakNo ratings yet
- Subcutaneous & Systemic MycosesDocument7 pagesSubcutaneous & Systemic MycosesDee GeeNo ratings yet
- Proceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964From EverandProceedings of the First International Congress of Parasitology: Roma, 21-26 September 1964Augusto CorradettiNo ratings yet
- Chapter 8Document53 pagesChapter 8contactrafiakhuramNo ratings yet
- Parasitology-Lec 13 MalariaDocument6 pagesParasitology-Lec 13 Malariaapi-3743217No ratings yet
- Protozoan Maricelle ManlutacDocument53 pagesProtozoan Maricelle ManlutacGlanela ManalotoNo ratings yet
- MicroPara Viro Questions by ApollonDocument13 pagesMicroPara Viro Questions by ApollonAngelo MercedeNo ratings yet
- Protist GuideDocument30 pagesProtist GuidemavicarigoreNo ratings yet
- Malaria Research in IndiaDocument8 pagesMalaria Research in IndiaPradeepNo ratings yet
- Methods in MalariaDocument351 pagesMethods in Malariakel910No ratings yet
- Plasmodium VivaxDocument4 pagesPlasmodium VivaxSUTHAN100% (1)
- Malaria 25 03 09Document131 pagesMalaria 25 03 09Dr.Jagadish Nuchina100% (5)
- Biology - Unit 4 Kingdom ProtistaDocument0 pagesBiology - Unit 4 Kingdom Protistawww.bhawesh.com.npNo ratings yet
- S Porozoa Plasmodium: Scientific Name: Plasmodium Higher Classification: PlasmodiidaeDocument8 pagesS Porozoa Plasmodium: Scientific Name: Plasmodium Higher Classification: PlasmodiidaeRhodaOriginalNo ratings yet
- Wbjee 2012 Biology Question PaperDocument8 pagesWbjee 2012 Biology Question Papersaurav guptaNo ratings yet
- Organism Staining OsceDocument105 pagesOrganism Staining OsceNachchakorn DellNo ratings yet
- Textbook Microbial Control of Vector Borne Diseases 1St Edition Brij Kishore Tyagi Ebook All Chapter PDFDocument53 pagesTextbook Microbial Control of Vector Borne Diseases 1St Edition Brij Kishore Tyagi Ebook All Chapter PDFjohn.saenz973100% (10)
- Literature Review On Malaria PDFDocument7 pagesLiterature Review On Malaria PDFaflsqyljm100% (1)
- Jornal Inggris 5Document7 pagesJornal Inggris 5putra aryaNo ratings yet
- Malaria Journal: Computer Vision For Microscopy Diagnosis of MalariaDocument14 pagesMalaria Journal: Computer Vision For Microscopy Diagnosis of MalariaDaniel Alfredo Galindo ChoqueNo ratings yet
- Group 3: Widia Yuni Pratiwi Sari Saiba Ningrum Ni Putu Rika Fadlunnisa Tiya MutiaraDocument12 pagesGroup 3: Widia Yuni Pratiwi Sari Saiba Ningrum Ni Putu Rika Fadlunnisa Tiya MutiaraWidia YuniNo ratings yet
- Malaria Situation in India: Dr. Neeraj Dhingra Additional Director & Head Malaria Division, NVBDCP Dghs Mohfw IndiaDocument21 pagesMalaria Situation in India: Dr. Neeraj Dhingra Additional Director & Head Malaria Division, NVBDCP Dghs Mohfw IndiaMJ SolNo ratings yet
- Helping Tapan RRB Je GS MCQ PDFDocument318 pagesHelping Tapan RRB Je GS MCQ PDFPoonam TripathiNo ratings yet
- 12Document72 pages12Malik RohailNo ratings yet
- MalariaDocument5 pagesMalariaRina KhazarenNo ratings yet
- Biology Notes Chap: 2Document4 pagesBiology Notes Chap: 2R.S.H82% (11)
- List of On-Roll Ph.D. Scholars at Thapar University, Patiala As On 29.06.2017Document18 pagesList of On-Roll Ph.D. Scholars at Thapar University, Patiala As On 29.06.2017SumanNo ratings yet
- What Causes Malaria?Document8 pagesWhat Causes Malaria?Dulce M. LupaseNo ratings yet
- AGBODEKA ET AL (3) - 2017 - Activité Antiplasmodiale Des Plantes Médicinales D'afrique de L'ouest Revue de La LitteratureDocument9 pagesAGBODEKA ET AL (3) - 2017 - Activité Antiplasmodiale Des Plantes Médicinales D'afrique de L'ouest Revue de La LitteratureGBEKLEYNo ratings yet
- Malaria Identification It Is Easier Than You Think!: Susan Flaker Johnson, MT (ASCP), MEPDDocument30 pagesMalaria Identification It Is Easier Than You Think!: Susan Flaker Johnson, MT (ASCP), MEPDasclswisconsinNo ratings yet
- Malaria Treatment Guidelines WHO 2010Document211 pagesMalaria Treatment Guidelines WHO 2010emc27No ratings yet
- Malaria Must Go (Satb)Document7 pagesMalaria Must Go (Satb)Mubiru DavidNo ratings yet