Download as pptx, pdf, or txt
You might also like
- VacancyRpt - R0 - Y1S2Document262 pagesVacancyRpt - R0 - Y1S2Darren OngNo ratings yet
- Hospital Project Proposal PDFDocument15 pagesHospital Project Proposal PDFSatya Prakash Sundram100% (1)
- Antipsychotics: Dr. Jai Shri Ram Junior Resident Department of Psychiatry RCSM GMC KolhapurDocument43 pagesAntipsychotics: Dr. Jai Shri Ram Junior Resident Department of Psychiatry RCSM GMC Kolhapurjairamjiki1996No ratings yet
- Clinical PharmacologyDocument29 pagesClinical PharmacologyBilal KhanNo ratings yet
- Antipsychotic Drugs: (Neuroleptics, Major Tranquillizer Ataractic)Document63 pagesAntipsychotic Drugs: (Neuroleptics, Major Tranquillizer Ataractic)Muhammad Masoom Akhtar100% (1)
- Pharmacotherapy For SchizophreniaDocument17 pagesPharmacotherapy For SchizophreniaNadya SaptarinaNo ratings yet
- Antidepressent (AutoRecovered)Document11 pagesAntidepressent (AutoRecovered)chakdiva11No ratings yet
- PharmatherapyDocument21 pagesPharmatherapyiiout346No ratings yet
- Psychotropic Medications Questions You Should Ask Your 37th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for October 16th, 2022: 3rd editionFrom EverandPsychotropic Medications Questions You Should Ask Your 37th Psychiatric Consultation William R. Yee M.D., J.D., Copyright Applied for October 16th, 2022: 3rd editionNo ratings yet
- نسخة ANTI-ARRHYTHMIC 2Document28 pagesنسخة ANTI-ARRHYTHMIC 2ManWol JangNo ratings yet
- ANXIOLYTICSDocument33 pagesANXIOLYTICSCletus MichaelNo ratings yet
- Anti PsycoticsDocument11 pagesAnti PsycoticsManayNo ratings yet
- Antidepressants Ssris, Snris: Selective Serotonin Reuptake Inhibitors Norepinephrine Reuptake InhibitorsDocument23 pagesAntidepressants Ssris, Snris: Selective Serotonin Reuptake Inhibitors Norepinephrine Reuptake InhibitorsJosh SchultzNo ratings yet
- Psychopamacology PresentationDocument131 pagesPsychopamacology Presentationsalmalissu0No ratings yet
- Null 2Document46 pagesNull 2Wazeerullah KhanNo ratings yet
- Pharma Cns2Document14 pagesPharma Cns2Umair MazharNo ratings yet
- AnxiolyticsDocument12 pagesAnxiolyticsIbraheem JabbarNo ratings yet
- Drug Class Review On BenzosDocument48 pagesDrug Class Review On BenzosRico RodriguezNo ratings yet
- SchizophreniaDocument9 pagesSchizophreniasavyaNo ratings yet
- 2 SchizophreniaDocument37 pages2 SchizophreniaAjigotto ubiq.No ratings yet
- Antipsychotics,-WPS OfficeDocument7 pagesAntipsychotics,-WPS Officermconvidhya sri2015No ratings yet
- Second Gen AtipsychoticDocument34 pagesSecond Gen Atipsychoticemamma hashirNo ratings yet
- Pharmacology of AntidepressantsDocument28 pagesPharmacology of Antidepressantsحيدر كريم سعيد حمزهNo ratings yet
- SCHIZOPHRENIADocument4 pagesSCHIZOPHRENIAFast MasoodNo ratings yet
- Antipsychotic Drugs: Referance Book .Essential of Pharmacology by Shah NawazDocument47 pagesAntipsychotic Drugs: Referance Book .Essential of Pharmacology by Shah NawazLaiba ShahNo ratings yet
- Antipsychotic Final PresentationDocument24 pagesAntipsychotic Final PresentationKhadija ArshadNo ratings yet
- 15) Psych Pharm IIDocument3 pages15) Psych Pharm IIFatimaNo ratings yet
- Antipsychotic DrugsDocument47 pagesAntipsychotic DrugsIkram UddinNo ratings yet
- AntidepresentDocument34 pagesAntidepresentmariaNo ratings yet
- Sedatives and Hypnotics-2Document10 pagesSedatives and Hypnotics-2FRANCA JAMGBADINo ratings yet
- Drug Treatment of Psychosis: Martha I. Dávila-García, Ph.D. Howard University Department of Pharmacology Spring 2002Document56 pagesDrug Treatment of Psychosis: Martha I. Dávila-García, Ph.D. Howard University Department of Pharmacology Spring 2002Deva RajNo ratings yet
- PSYCHOPHARMACOLOGYDocument35 pagesPSYCHOPHARMACOLOGYsalehaqamer64No ratings yet
- Psychotropic MedicationDocument28 pagesPsychotropic Medicationrmconvidhya sri2015No ratings yet
- Drugs Used in Mental IllnessDocument60 pagesDrugs Used in Mental IllnessDixa MeNo ratings yet
- Lecture - 3 Agents Used To Manage Schizophrenia June 2014Document36 pagesLecture - 3 Agents Used To Manage Schizophrenia June 2014Robert EdwardsNo ratings yet
- week 7Document12 pagesweek 7Noor Ul Ain TahirNo ratings yet
- PsychopharmacologyDocument77 pagesPsychopharmacologychachaazkaNo ratings yet
- Antipsychotic Agents & LithiumDocument66 pagesAntipsychotic Agents & LithiumNárēsh Yadav GäddēNo ratings yet
- Final PharmaDocument17 pagesFinal PharmaAmmara SiddiquiNo ratings yet
- Antipsychotics Risks and BenefitsDocument38 pagesAntipsychotics Risks and BenefitsElleNo ratings yet
- Types of Antidepressants and How They WorkDocument1 pageTypes of Antidepressants and How They WorkSadiq AchakzaiNo ratings yet
- Receptors Involved in Mental Disorders and The UseDocument17 pagesReceptors Involved in Mental Disorders and The Usedabafe4365No ratings yet
- Benzodiazipine Withdrawal SyndromeDocument5 pagesBenzodiazipine Withdrawal Syndromes.s.r.k.m. guptaNo ratings yet
- Antidepressents XyzDocument82 pagesAntidepressents XyzAnuranjan VishwakarmaNo ratings yet
- Antihypnotics and AnxiolyticsDocument12 pagesAntihypnotics and AnxiolyticsSabreena NordinNo ratings yet
- Autonomic 2Document5 pagesAutonomic 2Rudi_RegobizNo ratings yet
- Antipsychotics and Lithium TBLDocument10 pagesAntipsychotics and Lithium TBLTanveerNo ratings yet
- Psychopharmacology: Psychoses: Mental HealthDocument22 pagesPsychopharmacology: Psychoses: Mental Healthmeliha_mela1No ratings yet
- CH301N Antidepressants PresentationDocument15 pagesCH301N Antidepressants PresentationmaevienceNo ratings yet
- Name: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicDocument16 pagesName: Class: Department: Roll No.: Subject: Course Code: Cr. HR.: Submitted To: Date of Submission: TopicAnoosha FarooquiNo ratings yet
- Joanne Bernadette C. Aguilar BSN-3Document7 pagesJoanne Bernadette C. Aguilar BSN-3Joanne Bernadette AguilarNo ratings yet
- AnxiolyticsDocument8 pagesAnxiolyticsHengky_FandriNo ratings yet
- DosingAtypicalAntipsychoticsReview TREMEAU DialoguesClinicalNeuroscience2002Document6 pagesDosingAtypicalAntipsychoticsReview TREMEAU DialoguesClinicalNeuroscience2002Leslie CitromeNo ratings yet
- The PSYCH MAP ColoredDocument2 pagesThe PSYCH MAP Coloredcentrino17No ratings yet
- Tratamento de Tran PersonaDocument35 pagesTratamento de Tran PersonaDIARISTAS hgmfNo ratings yet
- Psychotropic DrugsDocument81 pagesPsychotropic DrugsJoan100% (2)
- Nm-Lec15 - (Anxiolytics, Sedatives & Hypnotics)Document39 pagesNm-Lec15 - (Anxiolytics, Sedatives & Hypnotics)geng gengNo ratings yet
- Antidepressants Are MedicationsDocument16 pagesAntidepressants Are MedicationsTaj lamajedNo ratings yet
- Hypnosedative Drugs 17.10.2023Document49 pagesHypnosedative Drugs 17.10.2023Nuhu SibaNo ratings yet
- Warnick-Prescribing Meds For Anxiety and Depression PlenaryDocument33 pagesWarnick-Prescribing Meds For Anxiety and Depression PlenaryAKNTAI002No ratings yet
- AntipsychoticsDocument47 pagesAntipsychoticsammar_ahmed_19No ratings yet
- SULPYCO Method: A New Quantum and Integrative Approach to DepressionFrom EverandSULPYCO Method: A New Quantum and Integrative Approach to DepressionNo ratings yet
- Sepsis Content Concepts MapDocument2 pagesSepsis Content Concepts Mapghodghod1230% (1)
- Clinical CodingDocument40 pagesClinical CodingEndla NavyasreeNo ratings yet
- Self Declaration Form Details For International Arriving PassengersDocument2 pagesSelf Declaration Form Details For International Arriving PassengersKoteswar MandavaNo ratings yet
- Tablets 100 MG: DipyridamoleDocument1 pageTablets 100 MG: DipyridamoleAat Prayoga MuhtarNo ratings yet
- Group 2 - Siloam Hospital - 2Document31 pagesGroup 2 - Siloam Hospital - 2Byu PALEMBANGNo ratings yet
- Jack DanielDocument11 pagesJack DanielJack PresadoNo ratings yet
- Book 1Document166 pagesBook 1Puput HepitasariNo ratings yet
- "Ebola" The Worst Virus From AfricaDocument3 pages"Ebola" The Worst Virus From AfricaCamilo CanoNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Aulia Putri ANo ratings yet
- A Scalable Program For Customized Patient Education VideosDocument5 pagesA Scalable Program For Customized Patient Education VideositaNo ratings yet
- A Guide To The NCH NotesDocument10 pagesA Guide To The NCH Notesmadimadi11No ratings yet
- Curriculum Vitae Format: Personal DetailsDocument5 pagesCurriculum Vitae Format: Personal Detailsmuhammadalimalik122No ratings yet
- Incentive SpirometryDocument6 pagesIncentive SpirometryRiza Angela BarazanNo ratings yet
- ch04 (Lecture) - Medical TerminologyDocument33 pagesch04 (Lecture) - Medical TerminologyJomar TeofiloNo ratings yet
- Puberty: Normal, Early, and Late DevelopmentDocument2 pagesPuberty: Normal, Early, and Late Developmentnisa_neyshaaljufri0% (1)
- Epilepsia Autoinmune Revisión SistemáticaDocument10 pagesEpilepsia Autoinmune Revisión SistemáticaRICARDO HUAMANNo ratings yet
- Self Assessment Guide Pharmacy Services NC IIIDocument6 pagesSelf Assessment Guide Pharmacy Services NC IIIAnesa TuñacaoNo ratings yet
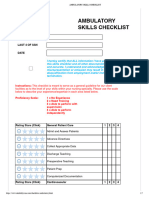
- Ambulatory Skills ChecklistDocument7 pagesAmbulatory Skills Checklistdk15janNo ratings yet
- Things Inside The First Aid Kit: Name: Emplamado, RG B. Course and Section: BS Accountancy - 1BDocument4 pagesThings Inside The First Aid Kit: Name: Emplamado, RG B. Course and Section: BS Accountancy - 1BArgNo ratings yet
- Prenatal and Postnatal CareDocument5 pagesPrenatal and Postnatal Caresarguss14100% (7)
- CHMP Assessment Report: Review Under Article 5 (3) of Regulation (EC) No 726/2004 Octagam and Associated NamesDocument7 pagesCHMP Assessment Report: Review Under Article 5 (3) of Regulation (EC) No 726/2004 Octagam and Associated NamesselmaNo ratings yet
- Southern Tagalog ChapterDocument4 pagesSouthern Tagalog ChapterwiltechworksNo ratings yet
- CV AgtDocument6 pagesCV AgtHafzhy TravelNo ratings yet
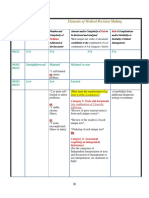
- 3-Level of MDMDocument3 pages3-Level of MDMmedical codingNo ratings yet
- Diagnosis of Spontaneous Canine Hyperadrenocorticism - 2012 ACVIM Consensus Statement (Small Animal)Document13 pagesDiagnosis of Spontaneous Canine Hyperadrenocorticism - 2012 ACVIM Consensus Statement (Small Animal)Maca Muñoz EscobedoNo ratings yet
- Sanford HealthDocument1 pageSanford Healthapi-471678788No ratings yet
- Psikoneuroimunologi: Oleh: Joni Haryanto, S.KP., MSDocument24 pagesPsikoneuroimunologi: Oleh: Joni Haryanto, S.KP., MSluluk badriyahNo ratings yet
- Subject Type of Exam Exam Date Number of Groups: Medical Chemistry Online. WRITTENDocument12 pagesSubject Type of Exam Exam Date Number of Groups: Medical Chemistry Online. WRITTENEhsan TariqNo ratings yet