Download as pptx, pdf, or txt
You might also like
- JCAHO Patient Tracer Survey ToolDocument8 pagesJCAHO Patient Tracer Survey ToolSherine HaykalNo ratings yet
- Nutri Lab ReviewerDocument53 pagesNutri Lab ReviewerRaquel MonsalveNo ratings yet
- NT1 - Sim - STD - 240306 2Document8 pagesNT1 - Sim - STD - 240306 2vitagp1124No ratings yet
- 2014-02-27 Revised - Surgeon Call Enhanced RecoveryDocument14 pages2014-02-27 Revised - Surgeon Call Enhanced RecoveryMahmoud IbrahimNo ratings yet
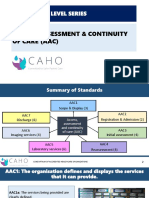
- AAC-Entry Level SeriesDocument51 pagesAAC-Entry Level SeriesPallavi Deepak DongreNo ratings yet
- Lec 4. Radiology WorkflowDocument24 pagesLec 4. Radiology Workflowallexa jimlaniNo ratings yet
- Documentation LabDocument41 pagesDocumentation LabYuna LeeNo ratings yet
- AACDocument45 pagesAACJagdish EmmehattiNo ratings yet
- Course Plan .......Document12 pagesCourse Plan .......chandhomepcNo ratings yet
- KH Enviornment of Care PhysiciansDocument2 pagesKH Enviornment of Care PhysiciansAngelo Russel LazagaNo ratings yet
- Perioperative - Semester SummaryDocument67 pagesPerioperative - Semester SummaryPatricia Eleanor FranksNo ratings yet
- Module 1 Identify and Record Cases of Priority Diseases, Conditions or Events - 7augDocument49 pagesModule 1 Identify and Record Cases of Priority Diseases, Conditions or Events - 7augSolomon Fallah Foa SandyNo ratings yet
- Golden Gate Colleges - Mrs. Gypsyrose Arojado: Health AssessmentDocument3 pagesGolden Gate Colleges - Mrs. Gypsyrose Arojado: Health AssessmentJaellaNo ratings yet
- RRT PPT With Changes Staff 12 30 13Document22 pagesRRT PPT With Changes Staff 12 30 13Dhaya DhayaNo ratings yet
- AAC-Entry Level SeriesDocument48 pagesAAC-Entry Level SeriesChandu PanditNo ratings yet
- Section Ite M Checklist Description Number TitleDocument4 pagesSection Ite M Checklist Description Number TitleIbrahim MassuquetoNo ratings yet
- Lecture 8 Surveillance FinalDocument55 pagesLecture 8 Surveillance FinalKhalil UllahNo ratings yet
- Chapter 12 NCM103Document22 pagesChapter 12 NCM103CyeonjNo ratings yet
- Or NursingDocument6 pagesOr NursingMark Elben TeodoroNo ratings yet
- Sentinel EventsDocument14 pagesSentinel EventsNatasha BhasinNo ratings yet
- Emergency and Disaster NursingDocument9 pagesEmergency and Disaster NursingDempsey AlmirañezNo ratings yet
- L2 Triage PrinciplesDocument38 pagesL2 Triage PrinciplesCrystal CHAN (FABULOUS)No ratings yet
- AHRQ Safety Program For Mechanically Ventilated Patients: The Four Es of Early MobilityDocument29 pagesAHRQ Safety Program For Mechanically Ventilated Patients: The Four Es of Early MobilityRosmira Agreda CabreraNo ratings yet
- BLI2028: Apparent Cause Analysis: Theresa Triplett Issues Management Program Manager Office of Institutional AssuranceDocument21 pagesBLI2028: Apparent Cause Analysis: Theresa Triplett Issues Management Program Manager Office of Institutional AssuranceMaureen Janelle RemaneaNo ratings yet
- Anesthesia Concept Book AtfDocument272 pagesAnesthesia Concept Book AtfDaksh ChoudharyNo ratings yet
- Weeks 6. Applyng Risk and Hazard ManagementDocument20 pagesWeeks 6. Applyng Risk and Hazard ManagementDhevana LyktaNo ratings yet
- General Pre and Post Operative Care-4 - 2Document2 pagesGeneral Pre and Post Operative Care-4 - 2BudiBoyPratamaNo ratings yet
- Incident Investigation ProcedureDocument31 pagesIncident Investigation ProcedureYuva samaj sewa TrustNo ratings yet
- wk4 DR Panithee 3july PDFDocument40 pageswk4 DR Panithee 3july PDFaekwinNo ratings yet
- HIPKABI-translation Into Research 16 DesDocument92 pagesHIPKABI-translation Into Research 16 Desar-rohhmah lantaisatuNo ratings yet
- Covid Vaccination Program DesignDocument22 pagesCovid Vaccination Program DesignJanet Vargas Gendrano100% (1)
- Sop Bedside Surgical ProceduresDocument4 pagesSop Bedside Surgical ProceduresInge SengkeyNo ratings yet
- Fundamentals of Nursing: BulletsDocument27 pagesFundamentals of Nursing: BulletsKristian Dave DivaNo ratings yet
- RCA Methodology For Investigation 1686321388Document37 pagesRCA Methodology For Investigation 1686321388sravanivenkataNo ratings yet
- Centra Analisis Causa Raiz Taller Mayo 2019 CocasepDocument46 pagesCentra Analisis Causa Raiz Taller Mayo 2019 CocasepGUILLERMO MARTÍNEZ PLNo ratings yet
- Ratna Puji Priyanti, S.Kep., NS., M.S Credited By: Ns. Senja SetiakaDocument39 pagesRatna Puji Priyanti, S.Kep., NS., M.S Credited By: Ns. Senja SetiakaIrmaNo ratings yet
- 3 Triage DocumentationDocument6 pages3 Triage DocumentationKianne Rae Fernandez PalmaNo ratings yet
- EM Clinical 7Document12 pagesEM Clinical 7Shinta Kusuma WNo ratings yet
- Disaster Management 2Document20 pagesDisaster Management 2TPA BCMHospitalNo ratings yet
- Management of Perioperative Client: Unit 5Document62 pagesManagement of Perioperative Client: Unit 5Ann A.No ratings yet
- Anesthesia Concept BookDocument274 pagesAnesthesia Concept BookMagic Feet100% (1)
- Part I: Emergency Department (ED) : SKINNY ReasoningDocument6 pagesPart I: Emergency Department (ED) : SKINNY ReasoningUzumaki KNo ratings yet
- H.A Rle First Lecture B5Document8 pagesH.A Rle First Lecture B5MARIANNE JOY ELEAZARNo ratings yet
- Patient Safety Di Kamar BedahDocument36 pagesPatient Safety Di Kamar BedahDewa DyskaNo ratings yet
- Pre-Quiz: Test Your Knowledge: 1. OSHA Has DevelopedDocument25 pagesPre-Quiz: Test Your Knowledge: 1. OSHA Has DevelopedJonryl NovicioNo ratings yet
- Studi Kasus RCA DR DiniDocument36 pagesStudi Kasus RCA DR Dinirusda al suwaibahNo ratings yet
- HSE Question Asked in Interviews PDFDocument15 pagesHSE Question Asked in Interviews PDFZubi KhankhailNo ratings yet
- RCA Worksheets With ActionsDocument29 pagesRCA Worksheets With ActionsMusaddiq MohammedNo ratings yet
- Case Analysis Format: Medical-Surgical & Maternal and Child Health Nursing ConceptsDocument4 pagesCase Analysis Format: Medical-Surgical & Maternal and Child Health Nursing ConceptsEmmy Flor ValmoriaNo ratings yet
- S M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationDocument6 pagesS M A R T: 201 A TEST #3 Define and Discuss The Purpose of Outcome IdentificationLindsay JonesNo ratings yet
- I.E (Adpie)Document4 pagesI.E (Adpie)Jayrelle D. SafranNo ratings yet
- Annexure 3 MC-Hospital Front Desk CoordinatorDocument14 pagesAnnexure 3 MC-Hospital Front Desk Coordinatorrais ahmadNo ratings yet
- Deviation & OOSDocument56 pagesDeviation & OOSRakeshNo ratings yet
- Table - For - Disaster - Preparedness - Plan - Outline (1) (1) October 2014Document3 pagesTable - For - Disaster - Preparedness - Plan - Outline (1) (1) October 2014hany winihastutiNo ratings yet
- FDARDocument41 pagesFDARJojo Justo100% (2)
- Root Cause AnalysisDocument5 pagesRoot Cause AnalysisPrabhas_Das7No ratings yet
- Preparation For Hospital Adaptation Presentation - 20240329 - 072106 - 0000Document38 pagesPreparation For Hospital Adaptation Presentation - 20240329 - 072106 - 0000Krizamay AggerNo ratings yet
- Anaesthesia and Sedation Outside TheatresDocument15 pagesAnaesthesia and Sedation Outside Theatresمحمد زينNo ratings yet
- Incident Investigation Facilitator Training Slide (Option 2) Final SlideDocument62 pagesIncident Investigation Facilitator Training Slide (Option 2) Final Slidecatherineezinwanne1No ratings yet
- Model Curriculum: Medical Laboratory TechnicianDocument46 pagesModel Curriculum: Medical Laboratory Techniciantoshan ramNo ratings yet
- TÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANOFrom EverandTÉCNICAS DEL AUXILIAR DE ENFERMERÍA EN EL ÁREA DE QUIRÓFANONo ratings yet
- Drug Study NifedipineDocument3 pagesDrug Study NifedipineJanzelvine Lee MontenegroNo ratings yet
- Knowledge, Attitude and Practice of Anganwadi Workers On Homoeopathic FormulationsDocument8 pagesKnowledge, Attitude and Practice of Anganwadi Workers On Homoeopathic FormulationsnovaNo ratings yet
- Health Care Facilities in KenyaDocument942 pagesHealth Care Facilities in KenyaPeter_Mutuma_1763100% (1)
- Involve US - A Stinging Eloquent Response To Discriminatory Guidelines in MBBS AdmissionsDocument2 pagesInvolve US - A Stinging Eloquent Response To Discriminatory Guidelines in MBBS AdmissionsDisability Rights AllianceNo ratings yet
- Michael J. Drabkin, MD Joins New York Imaging SpecialistsDocument4 pagesMichael J. Drabkin, MD Joins New York Imaging SpecialistsPR.comNo ratings yet
- CMS Memo and Approval of Kentucky 1115 WaiverDocument10 pagesCMS Memo and Approval of Kentucky 1115 WaiverInsider LouisvilleNo ratings yet
- Myra Estrin LevineDocument24 pagesMyra Estrin LevineLeonardo Balondo DulaNo ratings yet
- Burns FrostbitesDocument2 pagesBurns FrostbitesMaksims МаrkovsNo ratings yet
- The Management of Acute DystonicDocument2 pagesThe Management of Acute DystonictaqinosNo ratings yet
- DownloaderDocument6 pagesDownloaderSandeep SinghNo ratings yet
- مذكرة القصيمDocument126 pagesمذكرة القصيمAmr KazzazNo ratings yet
- SCRIPT Final EditDocument8 pagesSCRIPT Final EditRolando Ng IIINo ratings yet
- Me 46Document39 pagesMe 46Ace DanishNo ratings yet
- Ojha 2016Document7 pagesOjha 2016Manuel M SerazziNo ratings yet
- Chapter 4 Nutrition Weight Control and ExerciseDocument11 pagesChapter 4 Nutrition Weight Control and ExerciseDevanshNo ratings yet
- Republic If The PhilippinesDocument3 pagesRepublic If The PhilippinesKirby C. CatulinNo ratings yet
- Activity Design For Health SummitDocument2 pagesActivity Design For Health SummitJunard M. Lu Hap100% (2)
- CBSE Class 10 English Communicative SET 1 Compartment Annual Question Paper 2018Document8 pagesCBSE Class 10 English Communicative SET 1 Compartment Annual Question Paper 2018yashagg2008No ratings yet
- Ra 10354 PDFDocument24 pagesRa 10354 PDFmarkkkkkkkheeessNo ratings yet
- Position Description: About Boston Animal ShelterDocument2 pagesPosition Description: About Boston Animal ShelterJie ChengNo ratings yet
- Preboard 2 Maternal and Child and CHNDocument27 pagesPreboard 2 Maternal and Child and CHNDavid Lopez100% (3)
- ARANGUEZ NORTH SECONDARY SCHOO1. IIdocxDocument8 pagesARANGUEZ NORTH SECONDARY SCHOO1. IIdocxDevi RambaranNo ratings yet
- Legend Vaidhya NarayanamurthyDocument2 pagesLegend Vaidhya Narayanamurthyanbarasu86No ratings yet
- Historical Overview SaliganDocument21 pagesHistorical Overview SaliganReine Jholo BagaipoNo ratings yet
- Peritonits: - Peritonitis:Is An Inflammation (Irritation) of The Peritoneum, TheDocument20 pagesPeritonits: - Peritonitis:Is An Inflammation (Irritation) of The Peritoneum, TheManish SapkotaNo ratings yet
- Pamantasan NG Cabuyao: College of NursingDocument3 pagesPamantasan NG Cabuyao: College of NursingIssaiah Nicolle CeciliaNo ratings yet
- The Facts About COVID-19 Tests: The Two Test TypesDocument1 pageThe Facts About COVID-19 Tests: The Two Test TypesqwNo ratings yet
- Pediatrics Rapid RevisionDocument72 pagesPediatrics Rapid RevisionWorld MedclickzNo ratings yet
- 2012 - Yoon Et Al. - Contouring Guidelines of The Inguinal Lymph Nodes Using Lymphangiograms For The Delivery of Radiation Therapy in GastroDocument1 page2012 - Yoon Et Al. - Contouring Guidelines of The Inguinal Lymph Nodes Using Lymphangiograms For The Delivery of Radiation Therapy in GastroPoljarLijanNo ratings yet