Download as pptx, pdf, or txt
You might also like
- Colouring in For Emotional ClarityDocument6 pagesColouring in For Emotional ClarityRoy RoyNo ratings yet
- Date Performed: August 18, 2015 Group No. and Section: Group 5 WCDE-A Date Submitted: September 1, 2015 Group MembersDocument28 pagesDate Performed: August 18, 2015 Group No. and Section: Group 5 WCDE-A Date Submitted: September 1, 2015 Group MembersCm MacaliaNo ratings yet
- Neonatal HyperbilirubinemiaDocument22 pagesNeonatal HyperbilirubinemiaAnkur WadheraNo ratings yet
- Case Stude NNJDocument7 pagesCase Stude NNJmuzamirNo ratings yet
- Neonatal Jaundice: Zilpa, AMODocument44 pagesNeonatal Jaundice: Zilpa, AMOmarco luenaNo ratings yet
- HyperbilirubinemiaDocument49 pagesHyperbilirubinemiaKeith LajotNo ratings yet
- Jaundice NeonatalDocument26 pagesJaundice Neonatalhunk2662No ratings yet
- II. General and Specific ObjectivesDocument5 pagesII. General and Specific ObjectivesRae Marie AquinoNo ratings yet
- Neonatal JaundiceDocument24 pagesNeonatal JaundiceChetan SekhriNo ratings yet
- 19.neonatal JaundiceDocument42 pages19.neonatal JaundiceWilhellmuss MaukaNo ratings yet
- Factors Influencing Breastfeeding Practices Among Mothers in Lafia LocalDocument13 pagesFactors Influencing Breastfeeding Practices Among Mothers in Lafia LocalCha Tozenity ChieNo ratings yet
- Live Preterm Baby Delivered NSDDocument13 pagesLive Preterm Baby Delivered NSDKristine Anne SorianoNo ratings yet
- Multiple Organ Dysfunction SyndromeDocument4 pagesMultiple Organ Dysfunction SyndromeAna Reyes100% (1)
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Fetal Distress Case DiscussionDocument55 pagesFetal Distress Case DiscussionHafsah G.No ratings yet
- Respiratory DistressDocument10 pagesRespiratory DistressnilmbbsNo ratings yet
- PDF 075Document74 pagesPDF 075crystal_rc9No ratings yet
- Gestational Diabetes Mellitus Gestational Diabetes Mellitus (GDM) Is One of TheDocument10 pagesGestational Diabetes Mellitus Gestational Diabetes Mellitus (GDM) Is One of TheJobelle AcenaNo ratings yet
- Pathophysiology of HyperbilirubinemiaDocument3 pagesPathophysiology of Hyperbilirubinemiaapi-434682657No ratings yet
- Antepartal Assessment Rubric With RationaleDocument6 pagesAntepartal Assessment Rubric With RationaleSupremo Manuel M DeluaoNo ratings yet
- MECONIUM Aspiration SyndromeDocument37 pagesMECONIUM Aspiration SyndromekamalaNo ratings yet
- RH Disease and ABO IncompatibilityDocument21 pagesRH Disease and ABO Incompatibilityjeezislove617No ratings yet
- Multiple Gestation PPTDocument22 pagesMultiple Gestation PPTIrish Ivy VibethNo ratings yet
- Premature LaborDocument59 pagesPremature LaborAmiel Francisco ReyesNo ratings yet
- Beta ThalaDocument2 pagesBeta ThalaAngie LamoNo ratings yet
- DEFINITION: Abortion Is The Expulsion or Extraction From Its MotherDocument10 pagesDEFINITION: Abortion Is The Expulsion or Extraction From Its MothermOHAN.SNo ratings yet
- Amniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingDocument19 pagesAmniotic Fluid Embolism: Women's Hospital School of Medicine Zhejiang Un Iversity Wang ZhengpingPoonam RanaNo ratings yet
- Hirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Document5 pagesHirschsprung Disease Case Study: Maecy P. Tarinay BSN 4-1Maecy OdegaardNo ratings yet
- Abortion BSN 0PR-2: Case Study of BelleDocument27 pagesAbortion BSN 0PR-2: Case Study of BellekervinNo ratings yet
- MarasmusDocument1 pageMarasmusNovilee MartinezNo ratings yet
- Case Study HydrocephalusDocument19 pagesCase Study HydrocephalusJane Mae JesoroNo ratings yet
- Premature Rupture of MembraneDocument5 pagesPremature Rupture of MembraneEspiritu, ChriscelNo ratings yet
- Colonic Irrigation - Children's Hospital of Pittsburgh of UPMCDocument3 pagesColonic Irrigation - Children's Hospital of Pittsburgh of UPMCWaNda GrNo ratings yet
- Congenital Syphilis SeminarDocument32 pagesCongenital Syphilis SeminarRavi KumawatNo ratings yet
- Fetal DistressDocument19 pagesFetal DistressAnnisa DentinNo ratings yet
- Essential New Born Care ScriptDocument3 pagesEssential New Born Care ScriptShiela Joy DuquezNo ratings yet
- Management of Patients With Intestinal and Rectal DisordersDocument33 pagesManagement of Patients With Intestinal and Rectal DisordersDoneva Lyn MedinaNo ratings yet
- Observational Case Study of A NewbornDocument2 pagesObservational Case Study of A NewbornCheska Mae PalicNo ratings yet
- Translational Research: Generating Evidence For PracticeDocument24 pagesTranslational Research: Generating Evidence For Practicebeer_ettaaNo ratings yet
- Case Stude NNJDocument6 pagesCase Stude NNJmuzamirNo ratings yet
- Pregnancy Induced HypertensionDocument4 pagesPregnancy Induced HypertensionMjhay SalvadorNo ratings yet
- Ileus MeconiumDocument27 pagesIleus MeconiumDebby TamaraNo ratings yet
- Neonatal SepsisDocument65 pagesNeonatal SepsisRomMy WiEn MicKhoNo ratings yet
- PEDIA CASE 3 FinalDocument9 pagesPEDIA CASE 3 FinalXandra BnnNo ratings yet
- Care of The Newborn Infant: For More Information About The Authors and Reviewers of This Module, Click HereDocument30 pagesCare of The Newborn Infant: For More Information About The Authors and Reviewers of This Module, Click HereKeynethe JanineNo ratings yet
- Typhoid FeverDocument68 pagesTyphoid FeverLd Rachel PableoNo ratings yet
- Pathological Changes of DM - 2023Document53 pagesPathological Changes of DM - 2023Visura PrabodNo ratings yet
- Pelvic Inflammatory DiseaseDocument18 pagesPelvic Inflammatory DiseaseVictorNo ratings yet
- Postpartum Hemorrhage: Prepared By: Bande, Kyla Marie O. Lorente, Alfie John CDocument22 pagesPostpartum Hemorrhage: Prepared By: Bande, Kyla Marie O. Lorente, Alfie John CNi Ki TaNo ratings yet
- BronchiolitisDocument45 pagesBronchiolitisYuusuf MubarikNo ratings yet
- GonorrheaDocument7 pagesGonorrheaEköw Santiago JavierNo ratings yet
- Oxytocic & TocolyticDocument12 pagesOxytocic & TocolyticFahmi Dwika Hafiz TrionoNo ratings yet
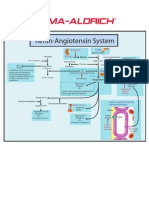
- Renin-Angiotensin SystemDocument1 pageRenin-Angiotensin SystemSigma-Aldrich100% (2)
- Individual Case PresentationDocument20 pagesIndividual Case Presentationim. EliasNo ratings yet
- NURSING CASE PRESENTATION NewDocument6 pagesNURSING CASE PRESENTATION NewHardeep KaurNo ratings yet
- Birth AsphyxiaDocument20 pagesBirth Asphyxiainne_fNo ratings yet
- Hirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHirschsprung’s Disease, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeFrom EverandThe Ride of Your Life: What I Learned about God, Love, and Adventure by Teaching My Son to Ride a BikeRating: 4.5 out of 5 stars4.5/5 (2)
- Gastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandGastric Outlet Obstruction, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- JaudiceDocument27 pagesJaudiceMar ClrNo ratings yet
- Neonatal Hyperbilirubinemia: Mahlet Abayneh Assistant Professor of PediatricsDocument41 pagesNeonatal Hyperbilirubinemia: Mahlet Abayneh Assistant Professor of PediatricsBegashawNo ratings yet
- Unit-6 Flow Through PipesDocument54 pagesUnit-6 Flow Through PipesS PrathebaNo ratings yet
- Admission Notification: 3 Floor, Composite Arts Building, Golapbag Golapbag, Burdwan: - 713 104 West Bengal, IndiaDocument3 pagesAdmission Notification: 3 Floor, Composite Arts Building, Golapbag Golapbag, Burdwan: - 713 104 West Bengal, IndiaHemnath Patra দর্শনNo ratings yet
- Clinical MedicineDocument18 pagesClinical MedicineRishikesh AsthanaNo ratings yet
- Menu PricipalDocument60 pagesMenu Pricipaldaher villarroelNo ratings yet
- III Module - A Survey On 4G-5G Dual Connectivity - Road To 5G ImplementationDocument18 pagesIII Module - A Survey On 4G-5G Dual Connectivity - Road To 5G ImplementationJoathan LessaNo ratings yet
- Operation Manual: Read Before Flying!Document24 pagesOperation Manual: Read Before Flying!ruup2010 AlexNo ratings yet
- Ga-G31m-S2l (Rev 1.2)Document33 pagesGa-G31m-S2l (Rev 1.2)Richard Hernandez RuizNo ratings yet
- II.A. Geology of Bangsamoro Autonomous Region in Muslim Mindanao (BARMM) Former ArmmDocument3 pagesII.A. Geology of Bangsamoro Autonomous Region in Muslim Mindanao (BARMM) Former ArmmMatthew Julius TatelNo ratings yet
- Virtual Artificial Sensor Technique For Functional Electrical StimulationDocument11 pagesVirtual Artificial Sensor Technique For Functional Electrical StimulationCarlos Alexandre FerriNo ratings yet
- Vintage Airplane - Jun 1979Document28 pagesVintage Airplane - Jun 1979Aviation/Space History LibraryNo ratings yet
- PWC - Emerging Trends in Real Estate 2024 ReportDocument142 pagesPWC - Emerging Trends in Real Estate 2024 Reportvaishalikarvir26No ratings yet
- Module 8 (Basic Aerodynamics)Document52 pagesModule 8 (Basic Aerodynamics)AmirAli MohebbiNo ratings yet
- SP660 (230 250W)Document1 pageSP660 (230 250W)Wildor Cordova SanchezNo ratings yet
- Gita Dhyanam English and SanskritDocument4 pagesGita Dhyanam English and SanskritSRIDHAR SUBRAMANIAM33% (3)
- Made By:-Shrish Ojha and Aryaman Singh MarjaraDocument34 pagesMade By:-Shrish Ojha and Aryaman Singh MarjaraSanskriti JoshiNo ratings yet
- Apologetics, Kreeft Chapter 11: Life After DeathDocument46 pagesApologetics, Kreeft Chapter 11: Life After DeathrichardNo ratings yet
- Assign#9Document3 pagesAssign#9Edrielle Valdez0% (1)
- Thermal Comfort of BuildingsDocument12 pagesThermal Comfort of BuildingsNavya BhardwajNo ratings yet
- Coolmay HMI User ManualDocument2 pagesCoolmay HMI User Manualspotlight studiosNo ratings yet
- Valproic Acid Drug CardDocument2 pagesValproic Acid Drug CardLiza Marie IgnacioNo ratings yet
- FF7 NT 2.0 Patch NotesDocument9 pagesFF7 NT 2.0 Patch NotesMiguel Lara JimenezNo ratings yet
- DataDocument17 pagesDataSumalatha VenkataswamyNo ratings yet
- Aerodynamics of A ParagliderDocument3 pagesAerodynamics of A Paraglider18th Attack SquadronNo ratings yet
- ANTARA Mobile Phone Portal (Angl. Qzyk)Document27 pagesANTARA Mobile Phone Portal (Angl. Qzyk)Shekina_YanaNo ratings yet
- GENERALISATIONDocument17 pagesGENERALISATIONgreyproperties88No ratings yet
- Manual Reloj DGT 2010 PDFDocument70 pagesManual Reloj DGT 2010 PDFGUILLERMO JLTNo ratings yet
- Work Tool Attachments: Product LineDocument24 pagesWork Tool Attachments: Product LineSzilárd SNo ratings yet
- PDK 025786 Diagnose enDocument296 pagesPDK 025786 Diagnose enMalek KamelNo ratings yet
- Kelainan Penis Pada AnakDocument23 pagesKelainan Penis Pada AnakAndrew SoerijadiNo ratings yet