
HMF by Kumaresan
HMF by Kumaresan
You might also like
- 2012 Goh & Burns Teaching Speaking - A Holistic ApproachDocument16 pages2012 Goh & Burns Teaching Speaking - A Holistic Approachdemarcus.benjamineNo ratings yet
- Neuroleadership Book PDF Free Neuroscience Leadership Management PsychologyDocument265 pagesNeuroleadership Book PDF Free Neuroscience Leadership Management Psychologyjames teboul100% (1)
- Neurological AssessmentDocument10 pagesNeurological AssessmentKristine AlejandroNo ratings yet
- Neuro Vital SignsDocument3 pagesNeuro Vital SignsKrissa Lei Pahang Razo100% (1)
- Neurological AssessmentDocument6 pagesNeurological AssessmentAlyssa Van Vark100% (1)
- Neuro AssessmentDocument13 pagesNeuro AssessmentOrlea Francisco-Sisio100% (2)
- My Ideal Classroom Environmental DesignDocument5 pagesMy Ideal Classroom Environmental Designapi-448497298No ratings yet
- HBO Decision MakingDocument28 pagesHBO Decision MakingKha RenNo ratings yet
- 1 Neuro AssessmentDocument10 pages1 Neuro Assessmentshuchi joshiNo ratings yet
- Advanced Nursin-Wps Office RachelDocument14 pagesAdvanced Nursin-Wps Office RachelRachel GeddamNo ratings yet
- Higher Mental FunctionDocument29 pagesHigher Mental Function19 Arya Ganesh OjhaNo ratings yet
- Assesment, Interpretation and Manganement of Altered ConsciousnessDocument36 pagesAssesment, Interpretation and Manganement of Altered ConsciousnessDwi Kartika RukmiNo ratings yet
- Higher Mental FunctionDocument26 pagesHigher Mental FunctionAJAYNo ratings yet
- Neuro Assessment: The Single Most Important AssessmentDocument10 pagesNeuro Assessment: The Single Most Important AssessmentpapadaadNo ratings yet
- Glasgow Coma ScaleDocument22 pagesGlasgow Coma Scaleshabatat2002No ratings yet
- Neurological AssessmentDocument9 pagesNeurological AssessmentrlinaoNo ratings yet
- Altered Level of ConsciousnessDocument8 pagesAltered Level of ConsciousnessMhae De GuzmanNo ratings yet
- The Single Most Important AssessmentDocument7 pagesThe Single Most Important Assessmenthellfire222No ratings yet
- Coma and Altered Mental Status: January 2006Document33 pagesComa and Altered Mental Status: January 2006pipikafiyaNo ratings yet
- Advance Nursing PracticeDocument12 pagesAdvance Nursing PracticebldewnaNo ratings yet
- Glasgow Coma Scale Zen2Document7 pagesGlasgow Coma Scale Zen2Zen Firhan ShahabNo ratings yet
- 1 Sensory Examination in Neuromuscular RehabilitationDocument44 pages1 Sensory Examination in Neuromuscular RehabilitationBinte MuhammadNo ratings yet
- Unconsciousness SeminarDocument23 pagesUnconsciousness SeminarJosh100% (3)
- Essentials of Neurological AssessmentDocument22 pagesEssentials of Neurological AssessmentSaid UstaranNo ratings yet
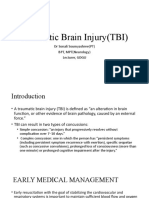
- Traumatic Brain Injury (TBI) : DR Sonali Soumyashree (PT) BPT, MPT (Neurology) Lecturer, GDGUDocument23 pagesTraumatic Brain Injury (TBI) : DR Sonali Soumyashree (PT) BPT, MPT (Neurology) Lecturer, GDGUSonali SoumyashreeNo ratings yet
- NvsDocument49 pagesNvsChong Uy AlawiNo ratings yet
- The Internal Processes Regulator and CognatorDocument2 pagesThe Internal Processes Regulator and CognatorJayrelle D. SafranNo ratings yet
- Level of ConsciousnessDocument10 pagesLevel of ConsciousnessDinda Ramos100% (1)
- The Patient With Altered ConsciousnessDocument59 pagesThe Patient With Altered Consciousnesssunilk09No ratings yet
- Neuromuscular System: Med SurgDocument25 pagesNeuromuscular System: Med Surgp23bhatiaNo ratings yet
- Altered Level of Consciousness - LOCDocument36 pagesAltered Level of Consciousness - LOCCecil MonteroNo ratings yet
- Elib - Tips - Performing Neurological AssessmentDocument34 pagesElib - Tips - Performing Neurological AssessmentTcx YivcNo ratings yet
- Assessment of Neurologic System: Nursing Health Assessment NCM101 Paolo Christian Bautista, RN LecturerDocument58 pagesAssessment of Neurologic System: Nursing Health Assessment NCM101 Paolo Christian Bautista, RN LecturerShaira SariaNo ratings yet
- Assignment of Neurology (Repaired) .Docx - 1494344936467Document24 pagesAssignment of Neurology (Repaired) .Docx - 1494344936467Amrit Preet KaurNo ratings yet
- Koma PPT EnglishDocument122 pagesKoma PPT EnglishRendy ReventonNo ratings yet
- Mental Status Examination: Level of ConsciousnessDocument4 pagesMental Status Examination: Level of Consciousnessmonica bayaoaNo ratings yet
- NCM 116Document9 pagesNCM 116karen dapalNo ratings yet
- Assessment of Neurologic Function: Dr. Lubna DwerijDocument41 pagesAssessment of Neurologic Function: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Neuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDocument29 pagesNeuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDarvin MathewNo ratings yet
- Coma and SyncopeDocument59 pagesComa and Syncopeabotreka056No ratings yet
- Physical Assessment - Specifics On General ObservationsDocument14 pagesPhysical Assessment - Specifics On General ObservationsJennifer B. GarciaNo ratings yet
- Altered Level of ConsciousnessDocument1 pageAltered Level of ConsciousnessChristian Jay Sacueza BucadNo ratings yet
- DRS R 98 FormDocument4 pagesDRS R 98 Formi love garfieldNo ratings yet
- Eyes Open, BrainDocument6 pagesEyes Open, BrainnikesemperNo ratings yet
- 05.delirium Rating ScaleDocument4 pages05.delirium Rating Scalei love garfieldNo ratings yet
- Assessment of The Nervous System - FinalDocument76 pagesAssessment of The Nervous System - FinalRona Lucido100% (1)
- Altered Mental StatusDocument151 pagesAltered Mental StatusbrentupdegraffNo ratings yet
- Unconsciousness - L SuneethaDocument16 pagesUnconsciousness - L SuneethaLanke SuneethaNo ratings yet
- NSO Glasgow Coma ScaleDocument3 pagesNSO Glasgow Coma Scaleanon_657718264No ratings yet
- Nuero Notes #2Document16 pagesNuero Notes #2Monica JubaneNo ratings yet
- Fundamental of Nursing IIDocument42 pagesFundamental of Nursing IIkezstacey61No ratings yet
- Neurological Examination PDFDocument17 pagesNeurological Examination PDFElsy MayjoNo ratings yet
- Altered Mental Status - 1Document28 pagesAltered Mental Status - 1Angelia Ongko PrabowoNo ratings yet
- Wall Neuro 2010Document34 pagesWall Neuro 2010Kath Jacinto100% (1)
- Lab Act 2 SensoryDocument5 pagesLab Act 2 SensoryZgama AbdulrahmanNo ratings yet
- Clinical Significance of Neuro AssessmentDocument1 pageClinical Significance of Neuro AssessmentabrarbuttNo ratings yet
- An Approach To Coma.Document32 pagesAn Approach To Coma.Divya GNo ratings yet
- Neurological AssessmentDocument113 pagesNeurological AssessmentAkshay BadoreNo ratings yet
- Advance Nursing Practice Presentation On Sensory DeprivationDocument22 pagesAdvance Nursing Practice Presentation On Sensory DeprivationLaveena Aswale67% (3)
- Dor, Sedação e AnalgesiaDocument33 pagesDor, Sedação e Analgesiatiago alvesNo ratings yet
- The AVPU ScaleDocument10 pagesThe AVPU ScalePrateek YadavNo ratings yet
- Beyond The Brain Re-Thinking Epilepsy Diagnosis And Treatment Through The Mind-Body ConnectionFrom EverandBeyond The Brain Re-Thinking Epilepsy Diagnosis And Treatment Through The Mind-Body ConnectionNo ratings yet
- Sleep: Regulation of Health Apps for Sleep Tracking (Guided Visualizations and Sleep Affirmations for Calm and Abundance in Anxious Artists)From EverandSleep: Regulation of Health Apps for Sleep Tracking (Guided Visualizations and Sleep Affirmations for Calm and Abundance in Anxious Artists)No ratings yet
- Roy's Adaptation ModelDocument20 pagesRoy's Adaptation ModelKiana Vren Jermia100% (6)
- The Self With OthersDocument61 pagesThe Self With OthersJohnny Ortega Sy Reyes IINo ratings yet
- English Text How To Have More WillpowerDocument1 pageEnglish Text How To Have More WillpowercarlorodriguesNo ratings yet
- Questioning PDFDocument7 pagesQuestioning PDFLokesh NANo ratings yet
- An Introduction To Child Development - Thomas KeenanDocument264 pagesAn Introduction To Child Development - Thomas KeenanMonikha Chandra boseNo ratings yet
- Seven Characteristics of ParadigmsDocument3 pagesSeven Characteristics of Paradigmsvedu710% (1)
- Neuro DynamicsDocument30 pagesNeuro DynamicsAnnisa Rahma SariNo ratings yet
- Intravenous Anesthetics: JRRMMC PGI Regalado, Trina Elisse TDocument18 pagesIntravenous Anesthetics: JRRMMC PGI Regalado, Trina Elisse THoneylynNo ratings yet
- Loftus Palmer 1974Document22 pagesLoftus Palmer 1974api-188978784No ratings yet
- Auditory Processing Disorder in Children - Symptoms and TreatmentsDocument2 pagesAuditory Processing Disorder in Children - Symptoms and TreatmentsAnn VillablancaNo ratings yet
- No. Isbn VolDocument131 pagesNo. Isbn VolBayu SmadaNo ratings yet
- Teaching Englishthrough SongsDocument22 pagesTeaching Englishthrough SongsLivia LuNo ratings yet
- Teste Faux PasDocument5 pagesTeste Faux PasAdriano FerrazNo ratings yet
- First Step To Achieve Your Objective - GomezDocument8 pagesFirst Step To Achieve Your Objective - GomezNicole Ivy GorimoNo ratings yet
- Why Teach Reading in The Different Content Areas?: Presented By: Roque R. Sabasaje Helen E. MaasinDocument11 pagesWhy Teach Reading in The Different Content Areas?: Presented By: Roque R. Sabasaje Helen E. MaasinluisaNo ratings yet
- Socialpsychology Week1recapDocument5 pagesSocialpsychology Week1recapYvzNo ratings yet
- سرﺪﻟا ١ Introducing Language Acquisition ﺔﻐﻠﻟا بﺎﺴﺘﻛا لﺎﺧدإ Lesson Objectives: فاﺪھﻷا سرﺪﻟاDocument26 pagesسرﺪﻟا ١ Introducing Language Acquisition ﺔﻐﻠﻟا بﺎﺴﺘﻛا لﺎﺧدإ Lesson Objectives: فاﺪھﻷا سرﺪﻟاfedo backNo ratings yet
- AutismDocument11 pagesAutismapi-3005480250% (1)
- Neural Networks For DummiesDocument10 pagesNeural Networks For DummiesmanojNo ratings yet
- FacilitateDocument17 pagesFacilitateCherrymae PoculanNo ratings yet
- Mindfulness and Psychology-Mark WilliamsDocument7 pagesMindfulness and Psychology-Mark WilliamsssanagavNo ratings yet
- Expert Judgement Checklist of Learning Media "E-Writing": 1 (Poor) 2 (Enough) 3 (Good) 4 (Very Good) 5 (Excellent)Document3 pagesExpert Judgement Checklist of Learning Media "E-Writing": 1 (Poor) 2 (Enough) 3 (Good) 4 (Very Good) 5 (Excellent)Sari DewiNo ratings yet
- Army Team Crew PDFDocument1 pageArmy Team Crew PDFAmirah AliNo ratings yet
- Academy Stars 3 - Syllabus - Test 3Document7 pagesAcademy Stars 3 - Syllabus - Test 3MargaritaCancelaNo ratings yet
- Autism - Literature ReviewDocument10 pagesAutism - Literature Reviewapi-446507356No ratings yet
- Retdem NeuroDocument3 pagesRetdem NeuroCharlize PareNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- 2012 Goh & Burns Teaching Speaking - A Holistic ApproachDocument16 pages2012 Goh & Burns Teaching Speaking - A Holistic Approachdemarcus.benjamineNo ratings yet
- Neuroleadership Book PDF Free Neuroscience Leadership Management PsychologyDocument265 pagesNeuroleadership Book PDF Free Neuroscience Leadership Management Psychologyjames teboul100% (1)
- Neurological AssessmentDocument10 pagesNeurological AssessmentKristine AlejandroNo ratings yet
- Neuro Vital SignsDocument3 pagesNeuro Vital SignsKrissa Lei Pahang Razo100% (1)
- Neurological AssessmentDocument6 pagesNeurological AssessmentAlyssa Van Vark100% (1)
- Neuro AssessmentDocument13 pagesNeuro AssessmentOrlea Francisco-Sisio100% (2)
- My Ideal Classroom Environmental DesignDocument5 pagesMy Ideal Classroom Environmental Designapi-448497298No ratings yet
- HBO Decision MakingDocument28 pagesHBO Decision MakingKha RenNo ratings yet
- 1 Neuro AssessmentDocument10 pages1 Neuro Assessmentshuchi joshiNo ratings yet
- Advanced Nursin-Wps Office RachelDocument14 pagesAdvanced Nursin-Wps Office RachelRachel GeddamNo ratings yet
- Higher Mental FunctionDocument29 pagesHigher Mental Function19 Arya Ganesh OjhaNo ratings yet
- Assesment, Interpretation and Manganement of Altered ConsciousnessDocument36 pagesAssesment, Interpretation and Manganement of Altered ConsciousnessDwi Kartika RukmiNo ratings yet
- Higher Mental FunctionDocument26 pagesHigher Mental FunctionAJAYNo ratings yet
- Neuro Assessment: The Single Most Important AssessmentDocument10 pagesNeuro Assessment: The Single Most Important AssessmentpapadaadNo ratings yet
- Glasgow Coma ScaleDocument22 pagesGlasgow Coma Scaleshabatat2002No ratings yet
- Neurological AssessmentDocument9 pagesNeurological AssessmentrlinaoNo ratings yet
- Altered Level of ConsciousnessDocument8 pagesAltered Level of ConsciousnessMhae De GuzmanNo ratings yet
- The Single Most Important AssessmentDocument7 pagesThe Single Most Important Assessmenthellfire222No ratings yet
- Coma and Altered Mental Status: January 2006Document33 pagesComa and Altered Mental Status: January 2006pipikafiyaNo ratings yet
- Advance Nursing PracticeDocument12 pagesAdvance Nursing PracticebldewnaNo ratings yet
- Glasgow Coma Scale Zen2Document7 pagesGlasgow Coma Scale Zen2Zen Firhan ShahabNo ratings yet
- 1 Sensory Examination in Neuromuscular RehabilitationDocument44 pages1 Sensory Examination in Neuromuscular RehabilitationBinte MuhammadNo ratings yet
- Unconsciousness SeminarDocument23 pagesUnconsciousness SeminarJosh100% (3)
- Essentials of Neurological AssessmentDocument22 pagesEssentials of Neurological AssessmentSaid UstaranNo ratings yet
- Traumatic Brain Injury (TBI) : DR Sonali Soumyashree (PT) BPT, MPT (Neurology) Lecturer, GDGUDocument23 pagesTraumatic Brain Injury (TBI) : DR Sonali Soumyashree (PT) BPT, MPT (Neurology) Lecturer, GDGUSonali SoumyashreeNo ratings yet
- NvsDocument49 pagesNvsChong Uy AlawiNo ratings yet
- The Internal Processes Regulator and CognatorDocument2 pagesThe Internal Processes Regulator and CognatorJayrelle D. SafranNo ratings yet
- Level of ConsciousnessDocument10 pagesLevel of ConsciousnessDinda Ramos100% (1)
- The Patient With Altered ConsciousnessDocument59 pagesThe Patient With Altered Consciousnesssunilk09No ratings yet
- Neuromuscular System: Med SurgDocument25 pagesNeuromuscular System: Med Surgp23bhatiaNo ratings yet
- Altered Level of Consciousness - LOCDocument36 pagesAltered Level of Consciousness - LOCCecil MonteroNo ratings yet
- Elib - Tips - Performing Neurological AssessmentDocument34 pagesElib - Tips - Performing Neurological AssessmentTcx YivcNo ratings yet
- Assessment of Neurologic System: Nursing Health Assessment NCM101 Paolo Christian Bautista, RN LecturerDocument58 pagesAssessment of Neurologic System: Nursing Health Assessment NCM101 Paolo Christian Bautista, RN LecturerShaira SariaNo ratings yet
- Assignment of Neurology (Repaired) .Docx - 1494344936467Document24 pagesAssignment of Neurology (Repaired) .Docx - 1494344936467Amrit Preet KaurNo ratings yet
- Koma PPT EnglishDocument122 pagesKoma PPT EnglishRendy ReventonNo ratings yet
- Mental Status Examination: Level of ConsciousnessDocument4 pagesMental Status Examination: Level of Consciousnessmonica bayaoaNo ratings yet
- NCM 116Document9 pagesNCM 116karen dapalNo ratings yet
- Assessment of Neurologic Function: Dr. Lubna DwerijDocument41 pagesAssessment of Neurologic Function: Dr. Lubna DwerijNoor MajaliNo ratings yet
- Neuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDocument29 pagesNeuro 101: Nursing Neuro Assessment: Kristen Ankrom, RN, SCRN, CCCC Stroke Coordinator Coliseum Medical CentersDarvin MathewNo ratings yet
- Coma and SyncopeDocument59 pagesComa and Syncopeabotreka056No ratings yet
- Physical Assessment - Specifics On General ObservationsDocument14 pagesPhysical Assessment - Specifics On General ObservationsJennifer B. GarciaNo ratings yet
- Altered Level of ConsciousnessDocument1 pageAltered Level of ConsciousnessChristian Jay Sacueza BucadNo ratings yet
- DRS R 98 FormDocument4 pagesDRS R 98 Formi love garfieldNo ratings yet
- Eyes Open, BrainDocument6 pagesEyes Open, BrainnikesemperNo ratings yet
- 05.delirium Rating ScaleDocument4 pages05.delirium Rating Scalei love garfieldNo ratings yet
- Assessment of The Nervous System - FinalDocument76 pagesAssessment of The Nervous System - FinalRona Lucido100% (1)
- Altered Mental StatusDocument151 pagesAltered Mental StatusbrentupdegraffNo ratings yet
- Unconsciousness - L SuneethaDocument16 pagesUnconsciousness - L SuneethaLanke SuneethaNo ratings yet
- NSO Glasgow Coma ScaleDocument3 pagesNSO Glasgow Coma Scaleanon_657718264No ratings yet
- Nuero Notes #2Document16 pagesNuero Notes #2Monica JubaneNo ratings yet
- Fundamental of Nursing IIDocument42 pagesFundamental of Nursing IIkezstacey61No ratings yet
- Neurological Examination PDFDocument17 pagesNeurological Examination PDFElsy MayjoNo ratings yet
- Altered Mental Status - 1Document28 pagesAltered Mental Status - 1Angelia Ongko PrabowoNo ratings yet
- Wall Neuro 2010Document34 pagesWall Neuro 2010Kath Jacinto100% (1)
- Lab Act 2 SensoryDocument5 pagesLab Act 2 SensoryZgama AbdulrahmanNo ratings yet
- Clinical Significance of Neuro AssessmentDocument1 pageClinical Significance of Neuro AssessmentabrarbuttNo ratings yet
- An Approach To Coma.Document32 pagesAn Approach To Coma.Divya GNo ratings yet
- Neurological AssessmentDocument113 pagesNeurological AssessmentAkshay BadoreNo ratings yet
- Advance Nursing Practice Presentation On Sensory DeprivationDocument22 pagesAdvance Nursing Practice Presentation On Sensory DeprivationLaveena Aswale67% (3)
- Dor, Sedação e AnalgesiaDocument33 pagesDor, Sedação e Analgesiatiago alvesNo ratings yet
- The AVPU ScaleDocument10 pagesThe AVPU ScalePrateek YadavNo ratings yet
- Beyond The Brain Re-Thinking Epilepsy Diagnosis And Treatment Through The Mind-Body ConnectionFrom EverandBeyond The Brain Re-Thinking Epilepsy Diagnosis And Treatment Through The Mind-Body ConnectionNo ratings yet
- Sleep: Regulation of Health Apps for Sleep Tracking (Guided Visualizations and Sleep Affirmations for Calm and Abundance in Anxious Artists)From EverandSleep: Regulation of Health Apps for Sleep Tracking (Guided Visualizations and Sleep Affirmations for Calm and Abundance in Anxious Artists)No ratings yet
- Roy's Adaptation ModelDocument20 pagesRoy's Adaptation ModelKiana Vren Jermia100% (6)
- The Self With OthersDocument61 pagesThe Self With OthersJohnny Ortega Sy Reyes IINo ratings yet
- English Text How To Have More WillpowerDocument1 pageEnglish Text How To Have More WillpowercarlorodriguesNo ratings yet
- Questioning PDFDocument7 pagesQuestioning PDFLokesh NANo ratings yet
- An Introduction To Child Development - Thomas KeenanDocument264 pagesAn Introduction To Child Development - Thomas KeenanMonikha Chandra boseNo ratings yet
- Seven Characteristics of ParadigmsDocument3 pagesSeven Characteristics of Paradigmsvedu710% (1)
- Neuro DynamicsDocument30 pagesNeuro DynamicsAnnisa Rahma SariNo ratings yet
- Intravenous Anesthetics: JRRMMC PGI Regalado, Trina Elisse TDocument18 pagesIntravenous Anesthetics: JRRMMC PGI Regalado, Trina Elisse THoneylynNo ratings yet
- Loftus Palmer 1974Document22 pagesLoftus Palmer 1974api-188978784No ratings yet
- Auditory Processing Disorder in Children - Symptoms and TreatmentsDocument2 pagesAuditory Processing Disorder in Children - Symptoms and TreatmentsAnn VillablancaNo ratings yet
- No. Isbn VolDocument131 pagesNo. Isbn VolBayu SmadaNo ratings yet
- Teaching Englishthrough SongsDocument22 pagesTeaching Englishthrough SongsLivia LuNo ratings yet
- Teste Faux PasDocument5 pagesTeste Faux PasAdriano FerrazNo ratings yet
- First Step To Achieve Your Objective - GomezDocument8 pagesFirst Step To Achieve Your Objective - GomezNicole Ivy GorimoNo ratings yet
- Why Teach Reading in The Different Content Areas?: Presented By: Roque R. Sabasaje Helen E. MaasinDocument11 pagesWhy Teach Reading in The Different Content Areas?: Presented By: Roque R. Sabasaje Helen E. MaasinluisaNo ratings yet
- Socialpsychology Week1recapDocument5 pagesSocialpsychology Week1recapYvzNo ratings yet
- سرﺪﻟا ١ Introducing Language Acquisition ﺔﻐﻠﻟا بﺎﺴﺘﻛا لﺎﺧدإ Lesson Objectives: فاﺪھﻷا سرﺪﻟاDocument26 pagesسرﺪﻟا ١ Introducing Language Acquisition ﺔﻐﻠﻟا بﺎﺴﺘﻛا لﺎﺧدإ Lesson Objectives: فاﺪھﻷا سرﺪﻟاfedo backNo ratings yet
- AutismDocument11 pagesAutismapi-3005480250% (1)
- Neural Networks For DummiesDocument10 pagesNeural Networks For DummiesmanojNo ratings yet
- FacilitateDocument17 pagesFacilitateCherrymae PoculanNo ratings yet
- Mindfulness and Psychology-Mark WilliamsDocument7 pagesMindfulness and Psychology-Mark WilliamsssanagavNo ratings yet
- Expert Judgement Checklist of Learning Media "E-Writing": 1 (Poor) 2 (Enough) 3 (Good) 4 (Very Good) 5 (Excellent)Document3 pagesExpert Judgement Checklist of Learning Media "E-Writing": 1 (Poor) 2 (Enough) 3 (Good) 4 (Very Good) 5 (Excellent)Sari DewiNo ratings yet
- Army Team Crew PDFDocument1 pageArmy Team Crew PDFAmirah AliNo ratings yet
- Academy Stars 3 - Syllabus - Test 3Document7 pagesAcademy Stars 3 - Syllabus - Test 3MargaritaCancelaNo ratings yet
- Autism - Literature ReviewDocument10 pagesAutism - Literature Reviewapi-446507356No ratings yet
- Retdem NeuroDocument3 pagesRetdem NeuroCharlize PareNo ratings yet