Download as pptx, pdf, or txt
You might also like
- Zeiss Laser 532 Service InstructionsDocument64 pagesZeiss Laser 532 Service InstructionsJavier Hdez100% (3)
- Mindray BS-200 - Service - Solution For Liquid Level Detect ErrorDocument16 pagesMindray BS-200 - Service - Solution For Liquid Level Detect ErrortranngockhoaNo ratings yet
- Humphrey Visual Field Interpretation - : Basic Glaucoma CourseDocument75 pagesHumphrey Visual Field Interpretation - : Basic Glaucoma CourseKetut AryawanNo ratings yet
- CorelDRAW Graphics Suite X7Document12 pagesCorelDRAW Graphics Suite X7Kevin Jack Maguiña Balarezo100% (1)
- 01 93 312-003.E11 HEP Basics of Perimetry SWDocument38 pages01 93 312-003.E11 HEP Basics of Perimetry SWMohamed AbdulaalNo ratings yet
- Paul Herzmark Intro To MicrosDocument62 pagesPaul Herzmark Intro To MicrosPetter willNo ratings yet
- Visual FieldsDocument86 pagesVisual FieldsoptorameshgpNo ratings yet
- Note3 PreClass PDFDocument21 pagesNote3 PreClass PDFSimon SiuNo ratings yet
- Ultrasound Quiz 1: UTQB50Document8 pagesUltrasound Quiz 1: UTQB50kingstonNo ratings yet
- WTW TurbidityDocument6 pagesWTW TurbidityIndra AditamaNo ratings yet
- Elements of Virtual PerceptionDocument45 pagesElements of Virtual PerceptionShivaNo ratings yet
- Tin It Us Quick GuideDocument5 pagesTin It Us Quick GuideMaria AntoniaNo ratings yet
- Basics of Imaging 2020Document36 pagesBasics of Imaging 2020None ImportantNo ratings yet
- OTDRDocument35 pagesOTDRkamenRider AgitoNo ratings yet
- Ugr Ku-LeuvenDocument24 pagesUgr Ku-LeuvenFenandoNo ratings yet
- VisualFields (Toric09, Handout)Document10 pagesVisualFields (Toric09, Handout)Paul H ArtesNo ratings yet
- EXP1-SOUND INTENSITY MEASUREMENT-non GuidedDocument4 pagesEXP1-SOUND INTENSITY MEASUREMENT-non GuidedRyan LauNo ratings yet
- Principle of Optical MicrosDocument24 pagesPrinciple of Optical MicrosPreeti RaoNo ratings yet
- Basics of PerimetryDocument96 pagesBasics of Perimetryதமிழன்டா தமிழன்டாNo ratings yet
- Color Communication & MatchingDocument46 pagesColor Communication & Matchingtrường phạmNo ratings yet
- Perimetry TestingDocument9 pagesPerimetry TestingEdward StevensonNo ratings yet
- TestingDocument18 pagesTestingVivekanandan JNo ratings yet
- Ultrasound Quiz 2Document4 pagesUltrasound Quiz 2Awadhesh Singh YadavNo ratings yet
- Intensity of Sound - TestingDocument9 pagesIntensity of Sound - TestingAtreyapurapu KrishnaNo ratings yet
- Usg B SCANDocument11 pagesUsg B SCANabuahmed&janaNo ratings yet
- 7 Common Oscilloscope Probing Pitfalls To AvoidDocument24 pages7 Common Oscilloscope Probing Pitfalls To AvoidFaizan MalikNo ratings yet
- Refractive Index of PrismDocument6 pagesRefractive Index of Prismpriyanka .SNo ratings yet
- Sine V-Ray BookDocument32 pagesSine V-Ray BookMoe yeik mayNo ratings yet
- Lecture NoiseDocument59 pagesLecture NoiselaterNo ratings yet
- NepheloturbidometryDocument6 pagesNepheloturbidometryzaife khanNo ratings yet
- Part1 - Eye - DV (7 Files Merged)Document127 pagesPart1 - Eye - DV (7 Files Merged)Matthew MalekNo ratings yet
- Part 1. General Instrumentation Concepts: Reading Assignment: Chapter 1 in Our TextbookDocument115 pagesPart 1. General Instrumentation Concepts: Reading Assignment: Chapter 1 in Our TextbookGlan DevadhasNo ratings yet
- Visualacuity PresentationDocument39 pagesVisualacuity PresentationcinemoviesuNo ratings yet
- أدوات القياسDocument3 pagesأدوات القياسKhezzari MerwenNo ratings yet
- Note3 PDFDocument16 pagesNote3 PDFSimon SiuNo ratings yet
- Colorimetry & SpectrophotometrDocument30 pagesColorimetry & SpectrophotometrAkki GangNo ratings yet
- Bio300n Laboratory Activity 1Document2 pagesBio300n Laboratory Activity 1Justine Vens G. AgustinNo ratings yet
- Calibrators EN 2021Document2 pagesCalibrators EN 2021danielNo ratings yet
- 6-Refractive Index of Prism-27!02!2024Document6 pages6-Refractive Index of Prism-27!02!20241213Stuti IyerNo ratings yet
- VFA Visual Field AssessmentDocument51 pagesVFA Visual Field AssessmentsightbdNo ratings yet
- Man Mic Basics Photoelectric en A22 DRW 950369 02 000Document10 pagesMan Mic Basics Photoelectric en A22 DRW 950369 02 000Leoned Cova OrozcoNo ratings yet
- 2006 - An Applicability Research On JND ModelDocument8 pages2006 - An Applicability Research On JND ModelL AndyNo ratings yet
- COLORIMETRYDocument30 pagesCOLORIMETRYSusovon ChowdhuryNo ratings yet
- What Is Turbidity?Document3 pagesWhat Is Turbidity?Naman HumaneNo ratings yet
- 541 Books Doubtnut Question BankDocument31 pages541 Books Doubtnut Question Bankkcsquare6No ratings yet
- Viva Voce RPTDocument2 pagesViva Voce RPTChandanNo ratings yet
- Colorimetry & SpectrophotometrDocument30 pagesColorimetry & SpectrophotometrBadruzzaman BarbhuiyaNo ratings yet
- Slides 4Document28 pagesSlides 4Yuk Shan ChengNo ratings yet
- Final Exam Preparation2Document25 pagesFinal Exam Preparation2natashaNo ratings yet
- 10 InductionDocument28 pages10 InductionRahmaan P AlamNo ratings yet
- Subjective Refraction (Theory)Document6 pagesSubjective Refraction (Theory)ScribdTranslationsNo ratings yet
- Light Fastness PDFDocument7 pagesLight Fastness PDFAmit SinghNo ratings yet
- Radiography in Dental ClinicDocument53 pagesRadiography in Dental ClinicSara MoustafaNo ratings yet
- GURPS 4e - (Unofficial) Anthony's GURPS - Light and DarknessDocument8 pagesGURPS 4e - (Unofficial) Anthony's GURPS - Light and DarknessBruno CelhoNo ratings yet
- Visual Performance: Aspects ConditionsDocument16 pagesVisual Performance: Aspects ConditionscehborrotoNo ratings yet
- Spectroscopy: Spectral Distribution of Radiant EnergyDocument28 pagesSpectroscopy: Spectral Distribution of Radiant EnergyKarim BiswasNo ratings yet
- Cinematic Sound: Class 1: AmplitudeDocument9 pagesCinematic Sound: Class 1: AmplitudeGabriel MartinhoNo ratings yet
- ARK-1 / AR-1: Auto Ref / Keratometer / Auto RefractometerDocument6 pagesARK-1 / AR-1: Auto Ref / Keratometer / Auto RefractometerbeniNo ratings yet
- IR Thermometers ExplainedDocument4 pagesIR Thermometers Explainedsugandaraj522No ratings yet
- A3 Tumblin Film Like 04Document22 pagesA3 Tumblin Film Like 04Arijit SharmaNo ratings yet
- Reflective Optical Beam Smoke Detector User GuideDocument8 pagesReflective Optical Beam Smoke Detector User GuidejolymolyNo ratings yet
- 7.1 HFA II Hard Drive OverviewDocument17 pages7.1 HFA II Hard Drive OverviewJavier HdezNo ratings yet
- 6.1 HFAIIi Hard Drive OverviewDocument18 pages6.1 HFAIIi Hard Drive OverviewJavier HdezNo ratings yet
- 3000Document252 pages3000Abi Nan Than100% (1)
- 3.1 GlaucomaDocument33 pages3.1 GlaucomaJavier HdezNo ratings yet
- 5.1 The HFA II PrintoutDocument15 pages5.1 The HFA II PrintoutJavier HdezNo ratings yet
- 1.1 History of PerimetryDocument42 pages1.1 History of PerimetryJavier HdezNo ratings yet
- USR TCP232 302 User Manual - V1.0.3.01 PDFDocument22 pagesUSR TCP232 302 User Manual - V1.0.3.01 PDFmcgeezer1No ratings yet
- OB Module 5Document48 pagesOB Module 5Neena MolNo ratings yet
- Red Black TreeDocument22 pagesRed Black TreeBelLa Quiennt BeycaNo ratings yet
- Influence of Ni On Martensitic Phase Transformations in NiTi Shape Memory Alloys 2010 Acta MaterialiaDocument15 pagesInfluence of Ni On Martensitic Phase Transformations in NiTi Shape Memory Alloys 2010 Acta MaterialiaJhonk FigueroaNo ratings yet
- The Pavilion Lounge: A Cricket Themed LoungeDocument34 pagesThe Pavilion Lounge: A Cricket Themed LoungeShreya DGNo ratings yet
- Base Oils: Technical Data Sheet NEXBASE 3043Document2 pagesBase Oils: Technical Data Sheet NEXBASE 3043Axel Mahya AvichenaNo ratings yet
- En 2014-03-17 RTU500 Series Product Catalogue OnlineDocument78 pagesEn 2014-03-17 RTU500 Series Product Catalogue OnlineЖорж КаназирскиNo ratings yet
- Skoda New Scala Brochure February 2024Document27 pagesSkoda New Scala Brochure February 2024ayawe888888No ratings yet
- Frank Kitson Warfare WholeDocument96 pagesFrank Kitson Warfare WholeDaniel RubinsteinNo ratings yet
- Hazardous Materials Operating GuideDocument128 pagesHazardous Materials Operating GuidenhishamNo ratings yet
- Neos 100Document34 pagesNeos 100David Bustamante ReyNo ratings yet
- Charusat NAAC SSRDocument204 pagesCharusat NAAC SSRbmcm bmefcolleges.edu.inNo ratings yet
- March 27, 2014Document10 pagesMarch 27, 2014The Delphos HeraldNo ratings yet
- AaDocument4 pagesAaCheck OndesNo ratings yet
- Strategic Leadership in The Media IndustryDocument6 pagesStrategic Leadership in The Media IndustryKorie ArsieNo ratings yet
- CSC 218 Notes 3Document8 pagesCSC 218 Notes 3Musa JubrilNo ratings yet
- 7.1.1 Administrator's Guide AIXDocument1,170 pages7.1.1 Administrator's Guide AIXÁgoston Péter100% (1)
- Investigating The Effect of Some Fabric Parameters On The Thermal Comfort Properties of Flat Knitted Acrylic Fabrics For Winter WearDocument11 pagesInvestigating The Effect of Some Fabric Parameters On The Thermal Comfort Properties of Flat Knitted Acrylic Fabrics For Winter WearSudipto BeheraNo ratings yet
- Lenovo V330-15IKB: 81AX0164GJDocument3 pagesLenovo V330-15IKB: 81AX0164GJLESTER HERRERANo ratings yet
- LAS 1A The Magic PomegranateDocument2 pagesLAS 1A The Magic PomegranateCherry Maravilla Basa MingoaNo ratings yet
- Users Manual 4215923Document7 pagesUsers Manual 4215923smallhausenNo ratings yet
- Machine Learning - 9: BITS PilaniDocument13 pagesMachine Learning - 9: BITS PilaniSimran sandhuNo ratings yet
- The World Is An Apple (Script)Document8 pagesThe World Is An Apple (Script)armandNo ratings yet
- Ch4 BootstrapDocument90 pagesCh4 BootstrapDaniels PicturesNo ratings yet
- Republic Act No. 7722: Higher Education Act of 1994Document45 pagesRepublic Act No. 7722: Higher Education Act of 1994belle100% (2)
- Installation Manual For Sea Tel 5009-17 Broadband-At-Sea Transmit / Receive System With Selectable Co-Pol or Cross-Pol ReceiveDocument173 pagesInstallation Manual For Sea Tel 5009-17 Broadband-At-Sea Transmit / Receive System With Selectable Co-Pol or Cross-Pol ReceiveJuan E CstllNo ratings yet
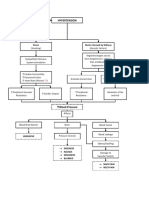
- Hypertension Concept MapDocument1 pageHypertension Concept Mapjyd parreñoNo ratings yet
- Resume Sr. Software Test Engineer, CRIF Solution, PuneDocument4 pagesResume Sr. Software Test Engineer, CRIF Solution, PuneamanNo ratings yet
- 0510 w09 Ms 3 PDFDocument13 pages0510 w09 Ms 3 PDFmastermido524No ratings yet