
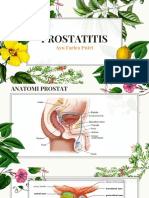
Prostatitis
Prostatitis
You might also like
- Urological and Gynaecological Chronic Pelvic Pain: Current TherapiesDocument401 pagesUrological and Gynaecological Chronic Pelvic Pain: Current TherapiesEn MengNo ratings yet
- Update On Prostatitis and TreatmentsDocument37 pagesUpdate On Prostatitis and TreatmentsAlbert Palomino RaymeNo ratings yet
- Aur v2 Id1016Document5 pagesAur v2 Id1016weisiNo ratings yet
- Pelvic PainDocument7 pagesPelvic PainwahyunizaNo ratings yet
- Chronic Pelvic PainDocument32 pagesChronic Pelvic PainKiyyaa KebedeNo ratings yet
- Premature Ejaculation and Chronic Bacterial Prostatitis: Original ArticleDocument5 pagesPremature Ejaculation and Chronic Bacterial Prostatitis: Original ArticleVarunNo ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- Michael Chancellor, Royal Oak, MI Pradeep Tyagi, Pittsburgh, PA Jayabalan Nirmal, Don Bui, Kenneth Peters, Royal Oak, MIDocument2 pagesMichael Chancellor, Royal Oak, MI Pradeep Tyagi, Pittsburgh, PA Jayabalan Nirmal, Don Bui, Kenneth Peters, Royal Oak, MIPpa Gpat AmitNo ratings yet
- TrafficDocument9 pagesTrafficMelanie LaginanNo ratings yet
- Bernstein 2005Document5 pagesBernstein 2005TediNo ratings yet
- Best of The 2001 AUA Annual MeetingDocument14 pagesBest of The 2001 AUA Annual MeetingneleatucicovshiiNo ratings yet
- The Effect of Photobiomodulation On Chemotherapy-Induced PeripheralDocument8 pagesThe Effect of Photobiomodulation On Chemotherapy-Induced PeripheralLizeth Arce100% (1)
- CR Management of FI - PeeyushDocument84 pagesCR Management of FI - Peeyushpeeyush2487No ratings yet
- AUS 05 History and Physical ExaminationDocument39 pagesAUS 05 History and Physical ExaminationhalayehiahNo ratings yet
- 10 1016@j Ejogrb 2015 09 020Document5 pages10 1016@j Ejogrb 2015 09 020samuel tapia pardoNo ratings yet
- Spring 2024 Clinical Soap Note 02Document5 pagesSpring 2024 Clinical Soap Note 02ivanbrosiffNo ratings yet
- Laporan KasusDocument22 pagesLaporan KasusMahek MunawarNo ratings yet
- Peleg: Case Report Sexual Intercourse As Potential Treatment For Intractable HiccupsDocument2 pagesPeleg: Case Report Sexual Intercourse As Potential Treatment For Intractable HiccupsdansippNo ratings yet
- Prostatitis AUA 2017Document29 pagesProstatitis AUA 2017Andres Felipe Cordoba AriasNo ratings yet
- 2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain SyndromeDocument7 pages2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain Syndromeenfermeironilson6321No ratings yet
- Acute Abdomen For EP: Prasit Wuthisuthimethawee Department of Emergency Medicine Prince of Songkla UniversityDocument77 pagesAcute Abdomen For EP: Prasit Wuthisuthimethawee Department of Emergency Medicine Prince of Songkla UniversityGunawan SamosirNo ratings yet
- Assessment and Diagnostic ExamsDocument10 pagesAssessment and Diagnostic ExamsJan Mark SotoNo ratings yet
- PST Partum HemorrhageDocument15 pagesPST Partum HemorrhageSampat Kumawat100% (1)
- Botulinum Toxin Injection For Childhood Constipation Is Safe and Can Be Effective Regardless of Anal Sphincter Dynamics. 2017Document5 pagesBotulinum Toxin Injection For Childhood Constipation Is Safe and Can Be Effective Regardless of Anal Sphincter Dynamics. 2017Gunduz AgaNo ratings yet
- Six-Month Follow-Up of Kinesitherapy For Cerebral Motor Disorders in Early ChildhoodDocument8 pagesSix-Month Follow-Up of Kinesitherapy For Cerebral Motor Disorders in Early ChildhoodIJAR JOURNALNo ratings yet
- Approach To Low Back PainDocument93 pagesApproach To Low Back Pain5jwd22sjfvNo ratings yet
- Articol Despre UTI in Paraplegic DogsDocument6 pagesArticol Despre UTI in Paraplegic DogsCristian FloreaNo ratings yet
- Relieving Symptoms of Meralgia Paresthetica Using Kinesio Taping - A Pilot StudyDocument3 pagesRelieving Symptoms of Meralgia Paresthetica Using Kinesio Taping - A Pilot StudyAdam MorrellNo ratings yet
- Ijms 19 03457Document6 pagesIjms 19 03457efendirahimNo ratings yet
- Acute Low Back PainDocument27 pagesAcute Low Back PainGalih Cakhya ImawanNo ratings yet
- 6 Tarcuan Myasthenia GravisDocument6 pages6 Tarcuan Myasthenia GravisAllan CastroNo ratings yet
- Continuous Compared With Cyclic Oral Contraceptives For The Treatment of Primary DysmenorrheaDocument9 pagesContinuous Compared With Cyclic Oral Contraceptives For The Treatment of Primary Dysmenorrheadokter wawanNo ratings yet
- J Eururo 2009 03 043Document7 pagesJ Eururo 2009 03 043vaibhav vinkareNo ratings yet
- Chen 2021Document8 pagesChen 2021metha anandaNo ratings yet
- Sii ArtículoDocument5 pagesSii ArtículoMonserrat Garduño FonsecaNo ratings yet
- Pelvic Pain1Document49 pagesPelvic Pain1kimshim81No ratings yet
- Pasricha 2020Document7 pagesPasricha 2020maloreed5No ratings yet
- Jam 4-10 1Document19 pagesJam 4-10 1Nur Ainatun NadrahNo ratings yet
- Ni Hms 454712Document14 pagesNi Hms 454712ponekNo ratings yet
- CPC Compiled Report FinalDocument24 pagesCPC Compiled Report FinalNestley TiongsonNo ratings yet
- Jurnal 6Document8 pagesJurnal 6Fatma BaagilNo ratings yet
- Chronic LumbagoDocument8 pagesChronic LumbagoOscar FrizziNo ratings yet
- Preparation For Safe PT Care 6 25 12Document20 pagesPreparation For Safe PT Care 6 25 12api-314231720100% (1)
- Tau 10 11 4100Document10 pagesTau 10 11 4100marcelloNo ratings yet
- Serum Neuroinflammatory Disease-Induced Central Nervous System Proteins Predict Clinical Onset of Experimental Autoimmune EncephalomyelitisDocument15 pagesSerum Neuroinflammatory Disease-Induced Central Nervous System Proteins Predict Clinical Onset of Experimental Autoimmune EncephalomyelitisIchim MadalinaNo ratings yet
- Pelvis Perineum Cases 04Document5 pagesPelvis Perineum Cases 04Uloko ChristopherNo ratings yet
- ANC ModuleDocument103 pagesANC ModulePreeti ChouhanNo ratings yet
- Case Study of Acute AppendicitisDocument28 pagesCase Study of Acute AppendicitisDominique RamosNo ratings yet
- Treatment of Gynecomastia With Prednisone Case RepDocument8 pagesTreatment of Gynecomastia With Prednisone Case RepGonzalo Sanchez DiazNo ratings yet
- Moldmedjournal 2017 603 Lacusta Full ArticleDocument6 pagesMoldmedjournal 2017 603 Lacusta Full Articlestudentactivity bookNo ratings yet
- Shaista ProtpolioDocument15 pagesShaista ProtpolioShafiq Ur RahmanNo ratings yet
- GUS2 - K5 - BPH Final 1Document52 pagesGUS2 - K5 - BPH Final 1Arifin MuhammadNo ratings yet
- 7th Lecture EBPDocument20 pages7th Lecture EBPway to satlokNo ratings yet
- General Santos Doctors' Medical School Foundation Inc.: Septic Shock Secondary To Ascending Cholangitis S/P ErcpDocument40 pagesGeneral Santos Doctors' Medical School Foundation Inc.: Septic Shock Secondary To Ascending Cholangitis S/P Ercpjay kusainNo ratings yet
- Quality of Life, and Survival in Patients With Effect of Neurolytic Celiac Plexus Block On Pain ReliefDocument9 pagesQuality of Life, and Survival in Patients With Effect of Neurolytic Celiac Plexus Block On Pain ReliefPrabhakar KumarNo ratings yet
- Untitled DocumentDocument16 pagesUntitled Documentclockstudy5No ratings yet
- AsenapineTransdermalPatchVsPlaceboPosterAbstract CITROME BiolPsych2019Document1 pageAsenapineTransdermalPatchVsPlaceboPosterAbstract CITROME BiolPsych2019Leslie CitromeNo ratings yet
- Diagnostic Approach of Dyspepsia SyndromeDocument20 pagesDiagnostic Approach of Dyspepsia SyndromeYaniNo ratings yet
- Etanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialDocument8 pagesEtanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialGiuseppe AcanforaNo ratings yet
- ProstatitisDocument13 pagesProstatitisBlanca HernándezNo ratings yet
- Acupuncture and Cold Laser Therapy For Pudendal Nerve PainDocument8 pagesAcupuncture and Cold Laser Therapy For Pudendal Nerve PainJøsh HessNo ratings yet
- Pentosan Polysulfate SodiumDocument1 pagePentosan Polysulfate SodiumOdessa FileNo ratings yet
- Ayurpharm 231Document6 pagesAyurpharm 231deepak anandNo ratings yet
- TCM and ProstateDocument5 pagesTCM and Prostatenadamau22633No ratings yet
- Prostate & Homoeopathic ManagementDocument69 pagesProstate & Homoeopathic ManagementSasiikumar Vattiyoorkavu Sankaran NairNo ratings yet
- PROSTATITIS (Tentiran Dr. Rinto)Document34 pagesPROSTATITIS (Tentiran Dr. Rinto)Anonymous kkogwa9CjNo ratings yet
- ProstitisDocument31 pagesProstitisMuhammad Makki0% (1)
- EAU Urological Guidelines Chronic Pelvic PainDocument100 pagesEAU Urological Guidelines Chronic Pelvic Painha606No ratings yet
- Male Pelvic Floor - Advanced Massage and BodyworkDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodyworkpujarze2No ratings yet
- Diagnosis and Treatment of Bacterial ProstatitisDocument5 pagesDiagnosis and Treatment of Bacterial ProstatitislobeseyNo ratings yet
- ProstatitisDocument23 pagesProstatitisDoha Ebed100% (1)
- Premature EjaculationDocument44 pagesPremature EjaculationTarek Anis67% (6)
- Campbell 12 TH CH 56 Inflammatory and Pain Conditions of The MaleDocument22 pagesCampbell 12 TH CH 56 Inflammatory and Pain Conditions of The MaleIkramIzatNo ratings yet
- Clinical UrologyDocument98 pagesClinical Urologythapan87100% (2)
- Male Pelvic Floor - Advanced Massage and Bodywork PDFDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodywork PDFpujarze2No ratings yet
- Urology PDFDocument24 pagesUrology PDFzzNo ratings yet
- Vibroacoustic Apparatus Vitafon-T : Exploitation Manual AND User GuideDocument44 pagesVibroacoustic Apparatus Vitafon-T : Exploitation Manual AND User GuideMax Smith0% (1)
- Prostatitis and Male Chronic Pelvic Pain Syndrome: What Is The Prostate?Document10 pagesProstatitis and Male Chronic Pelvic Pain Syndrome: What Is The Prostate?emagooNo ratings yet
- Dysuria in AdultsDocument8 pagesDysuria in AdultsSi vis pacem...No ratings yet
- BeepollenDocument14 pagesBeepollenInten KusumaNo ratings yet
- Thermaspec Presentation - September 2019Document70 pagesThermaspec Presentation - September 2019jack danialsNo ratings yet
- Abstracts USICON2017Document618 pagesAbstracts USICON2017rdLuis1No ratings yet
- Challenging Cases in Urological Surgery Karl Pang Full ChapterDocument77 pagesChallenging Cases in Urological Surgery Karl Pang Full Chapterroy.mula622100% (7)
- Curs 7 Urinary Tract InfectionsDocument110 pagesCurs 7 Urinary Tract InfectionsAnamaria SNo ratings yet
- Guidelines On: Chronic Pelvic PainDocument90 pagesGuidelines On: Chronic Pelvic PainPatrascu CristiNo ratings yet
- Pelvic PainDocument7 pagesPelvic PainwahyunizaNo ratings yet
- Treating HomestasisDocument49 pagesTreating HomestasisFahadNo ratings yet
- Male Dyspareunia - UpToDate PDFDocument15 pagesMale Dyspareunia - UpToDate PDFCamilo HernandezNo ratings yet























































































Download as pptx, pdf, or txt
You might also like
- Urological and Gynaecological Chronic Pelvic Pain: Current TherapiesDocument401 pagesUrological and Gynaecological Chronic Pelvic Pain: Current TherapiesEn MengNo ratings yet
- Update On Prostatitis and TreatmentsDocument37 pagesUpdate On Prostatitis and TreatmentsAlbert Palomino RaymeNo ratings yet
- Aur v2 Id1016Document5 pagesAur v2 Id1016weisiNo ratings yet
- Pelvic PainDocument7 pagesPelvic PainwahyunizaNo ratings yet
- Chronic Pelvic PainDocument32 pagesChronic Pelvic PainKiyyaa KebedeNo ratings yet
- Premature Ejaculation and Chronic Bacterial Prostatitis: Original ArticleDocument5 pagesPremature Ejaculation and Chronic Bacterial Prostatitis: Original ArticleVarunNo ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- Michael Chancellor, Royal Oak, MI Pradeep Tyagi, Pittsburgh, PA Jayabalan Nirmal, Don Bui, Kenneth Peters, Royal Oak, MIDocument2 pagesMichael Chancellor, Royal Oak, MI Pradeep Tyagi, Pittsburgh, PA Jayabalan Nirmal, Don Bui, Kenneth Peters, Royal Oak, MIPpa Gpat AmitNo ratings yet
- TrafficDocument9 pagesTrafficMelanie LaginanNo ratings yet
- Bernstein 2005Document5 pagesBernstein 2005TediNo ratings yet
- Best of The 2001 AUA Annual MeetingDocument14 pagesBest of The 2001 AUA Annual MeetingneleatucicovshiiNo ratings yet
- The Effect of Photobiomodulation On Chemotherapy-Induced PeripheralDocument8 pagesThe Effect of Photobiomodulation On Chemotherapy-Induced PeripheralLizeth Arce100% (1)
- CR Management of FI - PeeyushDocument84 pagesCR Management of FI - Peeyushpeeyush2487No ratings yet
- AUS 05 History and Physical ExaminationDocument39 pagesAUS 05 History and Physical ExaminationhalayehiahNo ratings yet
- 10 1016@j Ejogrb 2015 09 020Document5 pages10 1016@j Ejogrb 2015 09 020samuel tapia pardoNo ratings yet
- Spring 2024 Clinical Soap Note 02Document5 pagesSpring 2024 Clinical Soap Note 02ivanbrosiffNo ratings yet
- Laporan KasusDocument22 pagesLaporan KasusMahek MunawarNo ratings yet
- Peleg: Case Report Sexual Intercourse As Potential Treatment For Intractable HiccupsDocument2 pagesPeleg: Case Report Sexual Intercourse As Potential Treatment For Intractable HiccupsdansippNo ratings yet
- Prostatitis AUA 2017Document29 pagesProstatitis AUA 2017Andres Felipe Cordoba AriasNo ratings yet
- 2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain SyndromeDocument7 pages2017 Hwanglyunhaedok Pharmacopuncture Versus Saline Pharmacopuncture On Chronic Nonbacterial Prostatitis:Chronic Pelvic Pain Syndromeenfermeironilson6321No ratings yet
- Acute Abdomen For EP: Prasit Wuthisuthimethawee Department of Emergency Medicine Prince of Songkla UniversityDocument77 pagesAcute Abdomen For EP: Prasit Wuthisuthimethawee Department of Emergency Medicine Prince of Songkla UniversityGunawan SamosirNo ratings yet
- Assessment and Diagnostic ExamsDocument10 pagesAssessment and Diagnostic ExamsJan Mark SotoNo ratings yet
- PST Partum HemorrhageDocument15 pagesPST Partum HemorrhageSampat Kumawat100% (1)
- Botulinum Toxin Injection For Childhood Constipation Is Safe and Can Be Effective Regardless of Anal Sphincter Dynamics. 2017Document5 pagesBotulinum Toxin Injection For Childhood Constipation Is Safe and Can Be Effective Regardless of Anal Sphincter Dynamics. 2017Gunduz AgaNo ratings yet
- Six-Month Follow-Up of Kinesitherapy For Cerebral Motor Disorders in Early ChildhoodDocument8 pagesSix-Month Follow-Up of Kinesitherapy For Cerebral Motor Disorders in Early ChildhoodIJAR JOURNALNo ratings yet
- Approach To Low Back PainDocument93 pagesApproach To Low Back Pain5jwd22sjfvNo ratings yet
- Articol Despre UTI in Paraplegic DogsDocument6 pagesArticol Despre UTI in Paraplegic DogsCristian FloreaNo ratings yet
- Relieving Symptoms of Meralgia Paresthetica Using Kinesio Taping - A Pilot StudyDocument3 pagesRelieving Symptoms of Meralgia Paresthetica Using Kinesio Taping - A Pilot StudyAdam MorrellNo ratings yet
- Ijms 19 03457Document6 pagesIjms 19 03457efendirahimNo ratings yet
- Acute Low Back PainDocument27 pagesAcute Low Back PainGalih Cakhya ImawanNo ratings yet
- 6 Tarcuan Myasthenia GravisDocument6 pages6 Tarcuan Myasthenia GravisAllan CastroNo ratings yet
- Continuous Compared With Cyclic Oral Contraceptives For The Treatment of Primary DysmenorrheaDocument9 pagesContinuous Compared With Cyclic Oral Contraceptives For The Treatment of Primary Dysmenorrheadokter wawanNo ratings yet
- J Eururo 2009 03 043Document7 pagesJ Eururo 2009 03 043vaibhav vinkareNo ratings yet
- Chen 2021Document8 pagesChen 2021metha anandaNo ratings yet
- Sii ArtículoDocument5 pagesSii ArtículoMonserrat Garduño FonsecaNo ratings yet
- Pelvic Pain1Document49 pagesPelvic Pain1kimshim81No ratings yet
- Pasricha 2020Document7 pagesPasricha 2020maloreed5No ratings yet
- Jam 4-10 1Document19 pagesJam 4-10 1Nur Ainatun NadrahNo ratings yet
- Ni Hms 454712Document14 pagesNi Hms 454712ponekNo ratings yet
- CPC Compiled Report FinalDocument24 pagesCPC Compiled Report FinalNestley TiongsonNo ratings yet
- Jurnal 6Document8 pagesJurnal 6Fatma BaagilNo ratings yet
- Chronic LumbagoDocument8 pagesChronic LumbagoOscar FrizziNo ratings yet
- Preparation For Safe PT Care 6 25 12Document20 pagesPreparation For Safe PT Care 6 25 12api-314231720100% (1)
- Tau 10 11 4100Document10 pagesTau 10 11 4100marcelloNo ratings yet
- Serum Neuroinflammatory Disease-Induced Central Nervous System Proteins Predict Clinical Onset of Experimental Autoimmune EncephalomyelitisDocument15 pagesSerum Neuroinflammatory Disease-Induced Central Nervous System Proteins Predict Clinical Onset of Experimental Autoimmune EncephalomyelitisIchim MadalinaNo ratings yet
- Pelvis Perineum Cases 04Document5 pagesPelvis Perineum Cases 04Uloko ChristopherNo ratings yet
- ANC ModuleDocument103 pagesANC ModulePreeti ChouhanNo ratings yet
- Case Study of Acute AppendicitisDocument28 pagesCase Study of Acute AppendicitisDominique RamosNo ratings yet
- Treatment of Gynecomastia With Prednisone Case RepDocument8 pagesTreatment of Gynecomastia With Prednisone Case RepGonzalo Sanchez DiazNo ratings yet
- Moldmedjournal 2017 603 Lacusta Full ArticleDocument6 pagesMoldmedjournal 2017 603 Lacusta Full Articlestudentactivity bookNo ratings yet
- Shaista ProtpolioDocument15 pagesShaista ProtpolioShafiq Ur RahmanNo ratings yet
- GUS2 - K5 - BPH Final 1Document52 pagesGUS2 - K5 - BPH Final 1Arifin MuhammadNo ratings yet
- 7th Lecture EBPDocument20 pages7th Lecture EBPway to satlokNo ratings yet
- General Santos Doctors' Medical School Foundation Inc.: Septic Shock Secondary To Ascending Cholangitis S/P ErcpDocument40 pagesGeneral Santos Doctors' Medical School Foundation Inc.: Septic Shock Secondary To Ascending Cholangitis S/P Ercpjay kusainNo ratings yet
- Quality of Life, and Survival in Patients With Effect of Neurolytic Celiac Plexus Block On Pain ReliefDocument9 pagesQuality of Life, and Survival in Patients With Effect of Neurolytic Celiac Plexus Block On Pain ReliefPrabhakar KumarNo ratings yet
- Untitled DocumentDocument16 pagesUntitled Documentclockstudy5No ratings yet
- AsenapineTransdermalPatchVsPlaceboPosterAbstract CITROME BiolPsych2019Document1 pageAsenapineTransdermalPatchVsPlaceboPosterAbstract CITROME BiolPsych2019Leslie CitromeNo ratings yet
- Diagnostic Approach of Dyspepsia SyndromeDocument20 pagesDiagnostic Approach of Dyspepsia SyndromeYaniNo ratings yet
- Etanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialDocument8 pagesEtanercept in Alzheimer Disease: A Randomized, Placebo-Controlled, Double-Blind, Phase 2 TrialGiuseppe AcanforaNo ratings yet
- ProstatitisDocument13 pagesProstatitisBlanca HernándezNo ratings yet
- Acupuncture and Cold Laser Therapy For Pudendal Nerve PainDocument8 pagesAcupuncture and Cold Laser Therapy For Pudendal Nerve PainJøsh HessNo ratings yet
- Pentosan Polysulfate SodiumDocument1 pagePentosan Polysulfate SodiumOdessa FileNo ratings yet
- Ayurpharm 231Document6 pagesAyurpharm 231deepak anandNo ratings yet
- TCM and ProstateDocument5 pagesTCM and Prostatenadamau22633No ratings yet
- Prostate & Homoeopathic ManagementDocument69 pagesProstate & Homoeopathic ManagementSasiikumar Vattiyoorkavu Sankaran NairNo ratings yet
- PROSTATITIS (Tentiran Dr. Rinto)Document34 pagesPROSTATITIS (Tentiran Dr. Rinto)Anonymous kkogwa9CjNo ratings yet
- ProstitisDocument31 pagesProstitisMuhammad Makki0% (1)
- EAU Urological Guidelines Chronic Pelvic PainDocument100 pagesEAU Urological Guidelines Chronic Pelvic Painha606No ratings yet
- Male Pelvic Floor - Advanced Massage and BodyworkDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodyworkpujarze2No ratings yet
- Diagnosis and Treatment of Bacterial ProstatitisDocument5 pagesDiagnosis and Treatment of Bacterial ProstatitislobeseyNo ratings yet
- ProstatitisDocument23 pagesProstatitisDoha Ebed100% (1)
- Premature EjaculationDocument44 pagesPremature EjaculationTarek Anis67% (6)
- Campbell 12 TH CH 56 Inflammatory and Pain Conditions of The MaleDocument22 pagesCampbell 12 TH CH 56 Inflammatory and Pain Conditions of The MaleIkramIzatNo ratings yet
- Clinical UrologyDocument98 pagesClinical Urologythapan87100% (2)
- Male Pelvic Floor - Advanced Massage and Bodywork PDFDocument6 pagesMale Pelvic Floor - Advanced Massage and Bodywork PDFpujarze2No ratings yet
- Urology PDFDocument24 pagesUrology PDFzzNo ratings yet
- Vibroacoustic Apparatus Vitafon-T : Exploitation Manual AND User GuideDocument44 pagesVibroacoustic Apparatus Vitafon-T : Exploitation Manual AND User GuideMax Smith0% (1)
- Prostatitis and Male Chronic Pelvic Pain Syndrome: What Is The Prostate?Document10 pagesProstatitis and Male Chronic Pelvic Pain Syndrome: What Is The Prostate?emagooNo ratings yet
- Dysuria in AdultsDocument8 pagesDysuria in AdultsSi vis pacem...No ratings yet
- BeepollenDocument14 pagesBeepollenInten KusumaNo ratings yet
- Thermaspec Presentation - September 2019Document70 pagesThermaspec Presentation - September 2019jack danialsNo ratings yet
- Abstracts USICON2017Document618 pagesAbstracts USICON2017rdLuis1No ratings yet
- Challenging Cases in Urological Surgery Karl Pang Full ChapterDocument77 pagesChallenging Cases in Urological Surgery Karl Pang Full Chapterroy.mula622100% (7)
- Curs 7 Urinary Tract InfectionsDocument110 pagesCurs 7 Urinary Tract InfectionsAnamaria SNo ratings yet
- Guidelines On: Chronic Pelvic PainDocument90 pagesGuidelines On: Chronic Pelvic PainPatrascu CristiNo ratings yet
- Pelvic PainDocument7 pagesPelvic PainwahyunizaNo ratings yet
- Treating HomestasisDocument49 pagesTreating HomestasisFahadNo ratings yet
- Male Dyspareunia - UpToDate PDFDocument15 pagesMale Dyspareunia - UpToDate PDFCamilo HernandezNo ratings yet