Download as pptx, pdf, or txt
You might also like
- EthicsDocument13 pagesEthicsapi-485081343No ratings yet
- BCPS Study 10monthDocument5 pagesBCPS Study 10monthMagdy Ali ELsherbenyNo ratings yet
- BIND ScoreDocument2 pagesBIND Scoremahi_elsemary701175% (4)
- Ichthyosis Hystrix CurthDocument4 pagesIchthyosis Hystrix Curtheby_3tamaNo ratings yet
- Mfds April 2014 DONEDocument11 pagesMfds April 2014 DONEJoyce LimNo ratings yet
- Oral Lichen PlanusDocument28 pagesOral Lichen PlanusParul SinghNo ratings yet
- AL-Quds University Faculty of Dentistry Oral Pathology - Final Exam Third Year DR. Fahed HabashDocument10 pagesAL-Quds University Faculty of Dentistry Oral Pathology - Final Exam Third Year DR. Fahed HabashDaniella DukmakNo ratings yet
- Cosmetology Competency Exam 20101Document22 pagesCosmetology Competency Exam 20101ScribdTranslationsNo ratings yet
- Stages of Gingival InflammationDocument13 pagesStages of Gingival Inflammationvisi thiriyanNo ratings yet
- DR Meenakshi MDS Oral PathologyDocument29 pagesDR Meenakshi MDS Oral PathologyDr. Meenakshi SinghalNo ratings yet
- Fungal Infections of The Oral CavityDocument56 pagesFungal Infections of The Oral CavityAkash Anilkumar Malini100% (1)
- Desquamative GingivitisDocument41 pagesDesquamative Gingivitislucents100% (1)
- Ndodontics: Rubber Dam Frames and AccesoriesDocument5 pagesNdodontics: Rubber Dam Frames and AccesoriesFaber SidabutarNo ratings yet
- Oral Manifestations in Tuberculosis FinalDocument44 pagesOral Manifestations in Tuberculosis FinalCute ThingsNo ratings yet
- Prosthodontics - Removable Partial Denture: Prepared By: Michelle Ann Z. Zalzos, DMDDocument31 pagesProsthodontics - Removable Partial Denture: Prepared By: Michelle Ann Z. Zalzos, DMDMaryjoy PaladanNo ratings yet
- 2 5456181012360856193Document70 pages2 5456181012360856193Maha KhalidNo ratings yet
- Pyogenic GranulomaDocument13 pagesPyogenic GranulomaPiyusha SharmaNo ratings yet
- 2002 PDFDocument9 pages2002 PDFUlrich DjehaNo ratings yet
- Secondary Space Infection Oral SurgeryDocument4 pagesSecondary Space Infection Oral SurgeryFourthMolar.comNo ratings yet
- Gingival InflammationDocument19 pagesGingival InflammationmirfanulhaqNo ratings yet
- Bacterial Infections of Oral CavityDocument63 pagesBacterial Infections of Oral CavityAkash Anilkumar Malini67% (6)
- Gaint Cell Lesions UPLOADDocument176 pagesGaint Cell Lesions UPLOADAkshayNo ratings yet
- MCQDocument3 pagesMCQFoysal SirazeeNo ratings yet
- Oral Patho Test 1Document11 pagesOral Patho Test 1Vijay K PatelNo ratings yet
- Failures in Periodontal Therapy: Review ArticleDocument6 pagesFailures in Periodontal Therapy: Review ArticlezinniaNo ratings yet
- Dermatoven MCQDocument30 pagesDermatoven MCQS2 GIZI FKUI 2020No ratings yet
- KEY: Certain, Pretty Sure, Possible: 18 Years Old/female CameDocument8 pagesKEY: Certain, Pretty Sure, Possible: 18 Years Old/female Camefairodz salapudinNo ratings yet
- Culture Media in Oral PathologyDocument6 pagesCulture Media in Oral Pathologyimi4No ratings yet
- Tumours of Skin: DR F Bhatti Pennine VTS Sept 08Document39 pagesTumours of Skin: DR F Bhatti Pennine VTS Sept 08pfxbkNo ratings yet
- Summary of Diseases Exam 1Document9 pagesSummary of Diseases Exam 1smn416No ratings yet
- Benign Oral Soft Tissue TumorsDocument83 pagesBenign Oral Soft Tissue TumorsHanin AbukhiaraNo ratings yet
- 7 Bleeding Disorders DR - AlaaDocument35 pages7 Bleeding Disorders DR - Alaaaj1998ajNo ratings yet
- Aggressive Periodontitis: Localized & Generalized Forms by SamDocument24 pagesAggressive Periodontitis: Localized & Generalized Forms by SamNaghman Zuberi100% (1)
- Oral Path Summary SheetDocument5 pagesOral Path Summary Sheettrangy77No ratings yet
- Periodontal Problems in KidsDocument49 pagesPeriodontal Problems in KidsRaksmey PhanNo ratings yet
- Annular Lesions in Dermatology PDFDocument6 pagesAnnular Lesions in Dermatology PDFYanna RizkiaNo ratings yet
- Oral Pathology Lec - 1Document25 pagesOral Pathology Lec - 1مصطفى محمدNo ratings yet
- Open and Closed Mouth Techniques of Local AnesthesiaDocument88 pagesOpen and Closed Mouth Techniques of Local AnesthesiaAtika Iftikhar MirNo ratings yet
- Dermatology Mcqs For PGDocument204 pagesDermatology Mcqs For PGjusta7863No ratings yet
- Endo MishapsDocument66 pagesEndo MishapsmahmoudNo ratings yet
- DermatologyDocument3 pagesDermatologyDrkhslid890% (1)
- Derma MCQ Ch01 PDFDocument20 pagesDerma MCQ Ch01 PDFShah NawazNo ratings yet
- 2015Document45 pages2015jimmyNo ratings yet
- 2020 Tongue Disorders Ods 210Document25 pages2020 Tongue Disorders Ods 210Farhaana ShaboodienNo ratings yet
- Periodontal DiseasesDocument47 pagesPeriodontal DiseasesPratikNo ratings yet
- Vesiculobullous DiseasesDocument40 pagesVesiculobullous Diseasessgoeldoc_550661200100% (1)
- Histopathology of Dental Dental Caries 1Document39 pagesHistopathology of Dental Dental Caries 1Diana SuhartiNo ratings yet
- 01 Oral Cavity PDFDocument106 pages01 Oral Cavity PDFGhaydaa Abukhairan0% (1)
- Oral Pathology II BQDocument13 pagesOral Pathology II BQعبدالله إبراهيمNo ratings yet
- Vesiculobullous Disorders in Children2Document5 pagesVesiculobullous Disorders in Children2Luciana FernandesNo ratings yet
- Bollous MCQDocument21 pagesBollous MCQalh bashar100% (1)
- Neet SampleDocument18 pagesNeet SampledrpnnreddyNo ratings yet
- Osce 2018Document1 pageOsce 2018areej alblowiNo ratings yet
- Ve Siculo Bull Ous DiseasesDocument73 pagesVe Siculo Bull Ous DiseasesAARYANo ratings yet
- IPMdp 0801 A 12Document2 pagesIPMdp 0801 A 12Adelya AwdyaNo ratings yet
- Maxillary Nerve: Dr. Sanjana Mall Department of PedodonticsDocument48 pagesMaxillary Nerve: Dr. Sanjana Mall Department of PedodonticsSanjana MallNo ratings yet
- Gingival EnlargementDocument125 pagesGingival Enlargementdr_saurabhsinha_165No ratings yet
- Post-Test Periodontology: Prepared By: Dr. Christian Galileo DavidDocument4 pagesPost-Test Periodontology: Prepared By: Dr. Christian Galileo DavidAlene Victoria SareNo ratings yet
- Guidelines For The Management of Nappy RashDocument13 pagesGuidelines For The Management of Nappy RashOva PradiptaNo ratings yet
- Good Morning: by Ibrahim GBRDocument34 pagesGood Morning: by Ibrahim GBRDento - PhilicNo ratings yet
- Ranula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandRanula Cyst, (Salivary Cyst) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- GALLBLADDERDocument16 pagesGALLBLADDERKadenceFreya-Charisse G PosadasBulintao100% (2)
- Breast CancerDocument68 pagesBreast Cancerapi-3748365100% (4)
- HFOV High-Frequency-Oscillatory-VentilationDocument22 pagesHFOV High-Frequency-Oscillatory-VentilationJZNo ratings yet
- Presentation1 Ankush (Autosaved)Document17 pagesPresentation1 Ankush (Autosaved)AnshulNo ratings yet
- Red EyeDocument45 pagesRed EyeDavidVictoriousLukas100% (1)
- Siter One TabDocument8 pagesSiter One Tabhoremheb1No ratings yet
- K180428Document8 pagesK180428Tony ChenNo ratings yet
- Janssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryDocument3 pagesJanssen COVID-19 Vaccine (Johnson & Johnson) : Vaccine Preparation and Administration SummaryJohn Alex SelorioNo ratings yet
- Inn Effective TISSUE PERFUSION Related To Impaired O2 Ion AEB Dyspnea and Irregular Heart Rate and Rhythm.Document2 pagesInn Effective TISSUE PERFUSION Related To Impaired O2 Ion AEB Dyspnea and Irregular Heart Rate and Rhythm.Senyorita KHayeNo ratings yet
- CDR 24 S 8 eDocument66 pagesCDR 24 S 8 eHerminio Fuentes VelezNo ratings yet
- List of Must Read Books and Journals For DNB AnaesthesiaDocument2 pagesList of Must Read Books and Journals For DNB AnaesthesiaSirisha CkvNo ratings yet
- Rehabilitation After Amputation of The Lower Limb in The Course of Diabetic Foot SyndromeDocument7 pagesRehabilitation After Amputation of The Lower Limb in The Course of Diabetic Foot SyndromeNoreen PunjwaniNo ratings yet
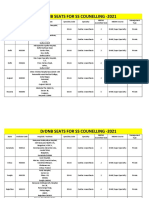
- Final DRDNB Seats For SS Counselling 2021Document152 pagesFinal DRDNB Seats For SS Counselling 2021Pavan KumarNo ratings yet
- Viral EncephalitisDocument101 pagesViral Encephalitisস্বপ্নকথাNo ratings yet
- Prognosis BipolarDocument8 pagesPrognosis BipolarTiti PrAtiwiNo ratings yet
- Baba T.1984. Cell-Mediated Immune Protection in Chickens Against P MultocidaDocument6 pagesBaba T.1984. Cell-Mediated Immune Protection in Chickens Against P MultocidakrodriguezNo ratings yet
- Doctor Sebi Diet 6 Books in 1 How To Det - Belinda GolemanDocument487 pagesDoctor Sebi Diet 6 Books in 1 How To Det - Belinda GolemanKristine Gerbolingo100% (1)
- Liver Cirrhosis: A Case Study OnDocument31 pagesLiver Cirrhosis: A Case Study OnCharmaine del RosarioNo ratings yet
- Cord Prolaps E.: Jens MartenssonDocument19 pagesCord Prolaps E.: Jens MartenssonPeter YanksonNo ratings yet
- Refractory Gastroesophageal Reflux Disease Diagnosis and ManagementDocument12 pagesRefractory Gastroesophageal Reflux Disease Diagnosis and Managementg-46005995No ratings yet
- Early Childhood Caries: A ReviewDocument7 pagesEarly Childhood Caries: A ReviewSuyatmiNo ratings yet
- Spleen Qi Defficiency SampleDocument33 pagesSpleen Qi Defficiency SampleVivek RaneNo ratings yet
- Comparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of EstradiolDocument8 pagesComparison of Estrone/Estradiol Ratio and Levels in Transfeminine Individuals on Different Routes of EstradiolSindatricks ZorokaNo ratings yet
- PsychopathologyDocument298 pagesPsychopathologyAlguémNo ratings yet
- Without Anskey-Ms RF, Ortho, Neuro - DrillsDocument13 pagesWithout Anskey-Ms RF, Ortho, Neuro - Drillsjon elleNo ratings yet
- Drug StudyDocument6 pagesDrug StudyMajo Coronel100% (1)
- Dr. Risma Dikirim Pukul 0 16sympo OptimizingDocument30 pagesDr. Risma Dikirim Pukul 0 16sympo OptimizingAlthof SonaNo ratings yet
- Urine Analysis.Document2 pagesUrine Analysis.aryasingh14022006No ratings yet