
Chapter 4 - Hematological Malignancies
Chapter 4 - Hematological Malignancies
You might also like
- Med Surg Final Exam Question BankDocument16 pagesMed Surg Final Exam Question Bankamelis100% (4)
- Non-Malignant Leukocyte Abnormalities PDFDocument35 pagesNon-Malignant Leukocyte Abnormalities PDFSindhu BabuNo ratings yet
- WBC DisorderDocument24 pagesWBC DisorderNirav SharmaNo ratings yet
- 2 WBCsDocument31 pages2 WBCsDanz ShNo ratings yet
- ERYTHROPOIESISDocument17 pagesERYTHROPOIESISsureshNo ratings yet
- ErythropoiesisDocument44 pagesErythropoiesisDr ratna kumariNo ratings yet
- Anemia 101-Case StudiesDocument20 pagesAnemia 101-Case StudiesZamharira MuslimNo ratings yet
- Cell CycleDocument27 pagesCell CycleDNYANESHWAR BIRADARNo ratings yet
- Cellular and Molecular Basis of InheritanceDocument71 pagesCellular and Molecular Basis of InheritancevalikoNo ratings yet
- Chapter 6 Cell CycleDocument28 pagesChapter 6 Cell CyclefatimaNo ratings yet
- Cell CycleDocument82 pagesCell CyclejxhnrafaelNo ratings yet
- Disorders of Granulocytes and MonocytesDocument45 pagesDisorders of Granulocytes and Monocytesswathi bsNo ratings yet
- Moleculer Basis of NeoplasiaDocument33 pagesMoleculer Basis of NeoplasiahudaNo ratings yet
- Haemolytic AnaemiaDocument44 pagesHaemolytic AnaemiaMark DemNo ratings yet
- Leucocytic DisordersDocument142 pagesLeucocytic DisordersBahaa ShaabanNo ratings yet
- HEMATOPOESISDocument71 pagesHEMATOPOESISHussenNo ratings yet
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- Haematology SAQDocument16 pagesHaematology SAQPowell KitagwaNo ratings yet
- Patho Physiology Lecture13Document10 pagesPatho Physiology Lecture13Manar AlzobiNo ratings yet
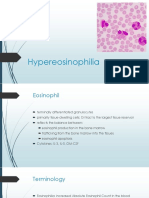
- Hypereosinophilia: DR Satya PrakashDocument19 pagesHypereosinophilia: DR Satya PrakashSatya PrakashNo ratings yet
- Haematological MalignanciesDocument63 pagesHaematological MalignanciesIsaac MwangiNo ratings yet
- Approach To Anemia: How To Efficiently and Accurately Work Up The Anemic ChildrenDocument16 pagesApproach To Anemia: How To Efficiently and Accurately Work Up The Anemic ChildrenArinaNo ratings yet
- Leucemia Limfatica CronicaDocument52 pagesLeucemia Limfatica CronicaAnghel BogdanNo ratings yet
- Quantitative and Qualitative Disorders of WBCsDocument9 pagesQuantitative and Qualitative Disorders of WBCsOliver BarnyakNo ratings yet
- Granulomatous Inflammation ThyroidDocument55 pagesGranulomatous Inflammation ThyroidKamlesh PrajapatiNo ratings yet
- Clinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDocument24 pagesClinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDzil FikriNo ratings yet
- LeukemiaDocument1 pageLeukemiaGomathiRachakondaNo ratings yet
- Molecular Basis of Cell AgingDocument57 pagesMolecular Basis of Cell AgingIrene Sulinsia NapitupuluNo ratings yet
- Anemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9Document30 pagesAnemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9hercolaniumNo ratings yet
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GNo ratings yet
- Anemia Chronic DiseaseDocument51 pagesAnemia Chronic Diseased_shadevNo ratings yet
- Pathology - Chapter 14Document14 pagesPathology - Chapter 14Cory GrayNo ratings yet
- Myeloproliferative DisorderDocument36 pagesMyeloproliferative DisorderKalpana ShahNo ratings yet
- POLYCYTHEMIADocument45 pagesPOLYCYTHEMIAVISHAL DUBEYNo ratings yet
- Molecular-Basis-of-Cancer-Behavior CREDITS TO OWNERDocument58 pagesMolecular-Basis-of-Cancer-Behavior CREDITS TO OWNERtfiveNo ratings yet
- Polycythemia VeraDocument4 pagesPolycythemia VeraAllyson VillarNo ratings yet
- Presented by T. V. L. Sahithi Ist Year PG Dept of PeriodonticsDocument49 pagesPresented by T. V. L. Sahithi Ist Year PG Dept of Periodonticslakshmi sahithi natakalaNo ratings yet
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniNo ratings yet
- Screening Test For Phagocytic Engulfment: DiapedesisDocument2 pagesScreening Test For Phagocytic Engulfment: DiapedesisBianca ANo ratings yet
- HeparinInduced ThrombocytopeniaDocument14 pagesHeparinInduced ThrombocytopeniaJefferson Candela RadaNo ratings yet
- Rheumatic Fever and Rheumatic Heart Disease 2017 and IeDocument59 pagesRheumatic Fever and Rheumatic Heart Disease 2017 and IeLipi GautamNo ratings yet
- Clinical EnzymologyDocument84 pagesClinical EnzymologyYeyeh SantosNo ratings yet
- Acute Lymphoblastic Leukemia (ALL)Document14 pagesAcute Lymphoblastic Leukemia (ALL)Med PhuongNo ratings yet
- Plasma Cell NeoplasmsDocument36 pagesPlasma Cell Neoplasmsdrafq2000No ratings yet
- Von Willibrand DiseasesDocument34 pagesVon Willibrand DiseasesZulfadli Hussein100% (1)
- Anemia BMLTDocument134 pagesAnemia BMLTRajkishor YadavNo ratings yet
- Oncology Revision: Paul BaillieDocument299 pagesOncology Revision: Paul BaillieMourian AmanNo ratings yet
- Macrocytic AnemiasDocument28 pagesMacrocytic AnemiasDeepankar SrigyanNo ratings yet
- Body Fluid Cell Counts by Automated MethodsDocument11 pagesBody Fluid Cell Counts by Automated MethodsntnquynhproNo ratings yet
- Exfoliative Cytology PDFDocument2 pagesExfoliative Cytology PDFStaceyNo ratings yet
- CML DiagnosisDocument4 pagesCML DiagnosisKarl Jimenez SeparaNo ratings yet
- Chronic Myeloid Leukemia HammadDocument33 pagesChronic Myeloid Leukemia HammadFaizan AhmedNo ratings yet
- Blood Cells MorphologyDocument20 pagesBlood Cells Morphologymoonfire2009No ratings yet
- Thallasemia: Shinta O WardhaniDocument12 pagesThallasemia: Shinta O WardhaniTonny Aldo Aprillino100% (1)
- Thrombosis and EmbolismDocument39 pagesThrombosis and Embolismilva100% (1)
- MULTIPLE MYELOMA For Medical Students. Copy - 032148Document39 pagesMULTIPLE MYELOMA For Medical Students. Copy - 032148Miracle Odenigbo100% (2)
- Chronic CholecystitisDocument7 pagesChronic CholecystitisErika alfonsoNo ratings yet
- Hematopoeitic System& Blood, KBK 2015 LDLDocument80 pagesHematopoeitic System& Blood, KBK 2015 LDLgita dwi ananda100% (1)
- CytologyDocument12 pagesCytologyEsther HutagalungNo ratings yet
- Acute Myeloid LeukemiaDocument1 pageAcute Myeloid LeukemiaAlleah Salbo KepusNo ratings yet
- Anatomy & Physiology Myelodysplastic Syndrome: PathophysiologyDocument8 pagesAnatomy & Physiology Myelodysplastic Syndrome: PathophysiologyLouise Anne Agnazata GayoNo ratings yet
- Pediatric Tumors 1Document35 pagesPediatric Tumors 1SarahNo ratings yet
- Nkarta Presentation March 2022Document29 pagesNkarta Presentation March 2022StNo ratings yet
- Disorders of The Blood and Neoplastic DisordersDocument72 pagesDisorders of The Blood and Neoplastic DisordersavisenicNo ratings yet
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Pediatric OncologyDocument57 pagesPediatric Oncologyjoycechicago100% (2)
- Acute Myeloid Leukemia: in This PageDocument6 pagesAcute Myeloid Leukemia: in This Pagebabbajee4uNo ratings yet
- September 2018: Frcpath Questions Hemato-OncologyDocument24 pagesSeptember 2018: Frcpath Questions Hemato-OncologySyed Danish Ali100% (1)
- Cancer Science DPhil Projects 2021 v5.0Document96 pagesCancer Science DPhil Projects 2021 v5.0David LeeNo ratings yet
- Leukaemia Lecture 01 - Aml - DRDocument69 pagesLeukaemia Lecture 01 - Aml - DRapi-273068056100% (1)
- Sheng Li CVDocument9 pagesSheng Li CVBasharat BhatNo ratings yet
- KJM 2022 97 5 308Document11 pagesKJM 2022 97 5 308knighderNo ratings yet
- 9.myelodysplastic Syndromes (MDS)Document21 pages9.myelodysplastic Syndromes (MDS)Safi UllahNo ratings yet
- 531 (1999) T. R. Golub: Science Et AlDocument8 pages531 (1999) T. R. Golub: Science Et AlBair PuigNo ratings yet
- Leukaemia Cutis in A 12-Year-Old Boy With Acute Myeloid LeukemiaDocument7 pagesLeukaemia Cutis in A 12-Year-Old Boy With Acute Myeloid LeukemiafikriafisNo ratings yet
- MUST To KNOW in Immunohematology Blood BankingDocument42 pagesMUST To KNOW in Immunohematology Blood BankingMerhella Amor Suerte MendozaNo ratings yet
- Review Article WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 4th EditionDocument8 pagesReview Article WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 4th EditionCat NhanNo ratings yet
- Leukemia Panel Sample ReportDocument2 pagesLeukemia Panel Sample ReportAnmol DubeyNo ratings yet
- Etiology of Gingivitis: September 2011Document19 pagesEtiology of Gingivitis: September 2011Phúc BùiNo ratings yet
- Resident Autopsy LogDocument5 pagesResident Autopsy LogrboumendjelNo ratings yet
- Conference On Aml Date 13072024Document2 pagesConference On Aml Date 13072024Sanjaykumar YadavNo ratings yet
- PANCYTOPENIADocument51 pagesPANCYTOPENIAResmyNo ratings yet
- Pathology Revision E6.5Document129 pagesPathology Revision E6.5massprithiv58No ratings yet
- Mouse Models of Cancer Methods and Protocols Methods in Molecular Biology 2773 1St Edition Maja Cemazar Online Ebook Texxtbook Full Chapter PDFDocument69 pagesMouse Models of Cancer Methods and Protocols Methods in Molecular Biology 2773 1St Edition Maja Cemazar Online Ebook Texxtbook Full Chapter PDFruth.eyer418100% (10)
- Hema Part 3 Final PDFDocument188 pagesHema Part 3 Final PDFH.B.ANo ratings yet
- Flow Cytometry in Neoplastic Hematology. Morphologic-Immunophen Otypic-Genetic Correlation 4th Edition Wojciech GorczycaDocument70 pagesFlow Cytometry in Neoplastic Hematology. Morphologic-Immunophen Otypic-Genetic Correlation 4th Edition Wojciech Gorczycaperlamissing899100% (7)
- 2.acknowledgement and Def Disease CompleteDocument18 pages2.acknowledgement and Def Disease CompleteStephanie Joy EscalaNo ratings yet
- Invasive Pulmonary Aspergillosis - Semin Respir Crit Care Med 2020Document19 pagesInvasive Pulmonary Aspergillosis - Semin Respir Crit Care Med 2020MICHAEL AMARILLO CORREANo ratings yet























































































Download as ppt, pdf, or txt
You might also like
- Med Surg Final Exam Question BankDocument16 pagesMed Surg Final Exam Question Bankamelis100% (4)
- Non-Malignant Leukocyte Abnormalities PDFDocument35 pagesNon-Malignant Leukocyte Abnormalities PDFSindhu BabuNo ratings yet
- WBC DisorderDocument24 pagesWBC DisorderNirav SharmaNo ratings yet
- 2 WBCsDocument31 pages2 WBCsDanz ShNo ratings yet
- ERYTHROPOIESISDocument17 pagesERYTHROPOIESISsureshNo ratings yet
- ErythropoiesisDocument44 pagesErythropoiesisDr ratna kumariNo ratings yet
- Anemia 101-Case StudiesDocument20 pagesAnemia 101-Case StudiesZamharira MuslimNo ratings yet
- Cell CycleDocument27 pagesCell CycleDNYANESHWAR BIRADARNo ratings yet
- Cellular and Molecular Basis of InheritanceDocument71 pagesCellular and Molecular Basis of InheritancevalikoNo ratings yet
- Chapter 6 Cell CycleDocument28 pagesChapter 6 Cell CyclefatimaNo ratings yet
- Cell CycleDocument82 pagesCell CyclejxhnrafaelNo ratings yet
- Disorders of Granulocytes and MonocytesDocument45 pagesDisorders of Granulocytes and Monocytesswathi bsNo ratings yet
- Moleculer Basis of NeoplasiaDocument33 pagesMoleculer Basis of NeoplasiahudaNo ratings yet
- Haemolytic AnaemiaDocument44 pagesHaemolytic AnaemiaMark DemNo ratings yet
- Leucocytic DisordersDocument142 pagesLeucocytic DisordersBahaa ShaabanNo ratings yet
- HEMATOPOESISDocument71 pagesHEMATOPOESISHussenNo ratings yet
- CML, CLLDocument118 pagesCML, CLLMunesh SherawatNo ratings yet
- Haematology SAQDocument16 pagesHaematology SAQPowell KitagwaNo ratings yet
- Patho Physiology Lecture13Document10 pagesPatho Physiology Lecture13Manar AlzobiNo ratings yet
- Hypereosinophilia: DR Satya PrakashDocument19 pagesHypereosinophilia: DR Satya PrakashSatya PrakashNo ratings yet
- Haematological MalignanciesDocument63 pagesHaematological MalignanciesIsaac MwangiNo ratings yet
- Approach To Anemia: How To Efficiently and Accurately Work Up The Anemic ChildrenDocument16 pagesApproach To Anemia: How To Efficiently and Accurately Work Up The Anemic ChildrenArinaNo ratings yet
- Leucemia Limfatica CronicaDocument52 pagesLeucemia Limfatica CronicaAnghel BogdanNo ratings yet
- Quantitative and Qualitative Disorders of WBCsDocument9 pagesQuantitative and Qualitative Disorders of WBCsOliver BarnyakNo ratings yet
- Granulomatous Inflammation ThyroidDocument55 pagesGranulomatous Inflammation ThyroidKamlesh PrajapatiNo ratings yet
- Clinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDocument24 pagesClinical Approach To Anemia: Fakultas Kedokteran Universitas Prima IndonesiaDzil FikriNo ratings yet
- LeukemiaDocument1 pageLeukemiaGomathiRachakondaNo ratings yet
- Molecular Basis of Cell AgingDocument57 pagesMolecular Basis of Cell AgingIrene Sulinsia NapitupuluNo ratings yet
- Anemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9Document30 pagesAnemia and Its Classification by DR Bashir Ahmed Dar A Sopore Kashmir 1228039135310976 9hercolaniumNo ratings yet
- Lymphoid NeoplasmsDocument52 pagesLymphoid NeoplasmsAmalia Riska GNo ratings yet
- Anemia Chronic DiseaseDocument51 pagesAnemia Chronic Diseased_shadevNo ratings yet
- Pathology - Chapter 14Document14 pagesPathology - Chapter 14Cory GrayNo ratings yet
- Myeloproliferative DisorderDocument36 pagesMyeloproliferative DisorderKalpana ShahNo ratings yet
- POLYCYTHEMIADocument45 pagesPOLYCYTHEMIAVISHAL DUBEYNo ratings yet
- Molecular-Basis-of-Cancer-Behavior CREDITS TO OWNERDocument58 pagesMolecular-Basis-of-Cancer-Behavior CREDITS TO OWNERtfiveNo ratings yet
- Polycythemia VeraDocument4 pagesPolycythemia VeraAllyson VillarNo ratings yet
- Presented by T. V. L. Sahithi Ist Year PG Dept of PeriodonticsDocument49 pagesPresented by T. V. L. Sahithi Ist Year PG Dept of Periodonticslakshmi sahithi natakalaNo ratings yet
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Document20 pagesHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniNo ratings yet
- Screening Test For Phagocytic Engulfment: DiapedesisDocument2 pagesScreening Test For Phagocytic Engulfment: DiapedesisBianca ANo ratings yet
- HeparinInduced ThrombocytopeniaDocument14 pagesHeparinInduced ThrombocytopeniaJefferson Candela RadaNo ratings yet
- Rheumatic Fever and Rheumatic Heart Disease 2017 and IeDocument59 pagesRheumatic Fever and Rheumatic Heart Disease 2017 and IeLipi GautamNo ratings yet
- Clinical EnzymologyDocument84 pagesClinical EnzymologyYeyeh SantosNo ratings yet
- Acute Lymphoblastic Leukemia (ALL)Document14 pagesAcute Lymphoblastic Leukemia (ALL)Med PhuongNo ratings yet
- Plasma Cell NeoplasmsDocument36 pagesPlasma Cell Neoplasmsdrafq2000No ratings yet
- Von Willibrand DiseasesDocument34 pagesVon Willibrand DiseasesZulfadli Hussein100% (1)
- Anemia BMLTDocument134 pagesAnemia BMLTRajkishor YadavNo ratings yet
- Oncology Revision: Paul BaillieDocument299 pagesOncology Revision: Paul BaillieMourian AmanNo ratings yet
- Macrocytic AnemiasDocument28 pagesMacrocytic AnemiasDeepankar SrigyanNo ratings yet
- Body Fluid Cell Counts by Automated MethodsDocument11 pagesBody Fluid Cell Counts by Automated MethodsntnquynhproNo ratings yet
- Exfoliative Cytology PDFDocument2 pagesExfoliative Cytology PDFStaceyNo ratings yet
- CML DiagnosisDocument4 pagesCML DiagnosisKarl Jimenez SeparaNo ratings yet
- Chronic Myeloid Leukemia HammadDocument33 pagesChronic Myeloid Leukemia HammadFaizan AhmedNo ratings yet
- Blood Cells MorphologyDocument20 pagesBlood Cells Morphologymoonfire2009No ratings yet
- Thallasemia: Shinta O WardhaniDocument12 pagesThallasemia: Shinta O WardhaniTonny Aldo Aprillino100% (1)
- Thrombosis and EmbolismDocument39 pagesThrombosis and Embolismilva100% (1)
- MULTIPLE MYELOMA For Medical Students. Copy - 032148Document39 pagesMULTIPLE MYELOMA For Medical Students. Copy - 032148Miracle Odenigbo100% (2)
- Chronic CholecystitisDocument7 pagesChronic CholecystitisErika alfonsoNo ratings yet
- Hematopoeitic System& Blood, KBK 2015 LDLDocument80 pagesHematopoeitic System& Blood, KBK 2015 LDLgita dwi ananda100% (1)
- CytologyDocument12 pagesCytologyEsther HutagalungNo ratings yet
- Acute Myeloid LeukemiaDocument1 pageAcute Myeloid LeukemiaAlleah Salbo KepusNo ratings yet
- Anatomy & Physiology Myelodysplastic Syndrome: PathophysiologyDocument8 pagesAnatomy & Physiology Myelodysplastic Syndrome: PathophysiologyLouise Anne Agnazata GayoNo ratings yet
- Pediatric Tumors 1Document35 pagesPediatric Tumors 1SarahNo ratings yet
- Nkarta Presentation March 2022Document29 pagesNkarta Presentation March 2022StNo ratings yet
- Disorders of The Blood and Neoplastic DisordersDocument72 pagesDisorders of The Blood and Neoplastic DisordersavisenicNo ratings yet
- Red and White Blood Cell DisordersDocument11 pagesRed and White Blood Cell DisordersVittorio Di PaoloNo ratings yet
- Pediatric OncologyDocument57 pagesPediatric Oncologyjoycechicago100% (2)
- Acute Myeloid Leukemia: in This PageDocument6 pagesAcute Myeloid Leukemia: in This Pagebabbajee4uNo ratings yet
- September 2018: Frcpath Questions Hemato-OncologyDocument24 pagesSeptember 2018: Frcpath Questions Hemato-OncologySyed Danish Ali100% (1)
- Cancer Science DPhil Projects 2021 v5.0Document96 pagesCancer Science DPhil Projects 2021 v5.0David LeeNo ratings yet
- Leukaemia Lecture 01 - Aml - DRDocument69 pagesLeukaemia Lecture 01 - Aml - DRapi-273068056100% (1)
- Sheng Li CVDocument9 pagesSheng Li CVBasharat BhatNo ratings yet
- KJM 2022 97 5 308Document11 pagesKJM 2022 97 5 308knighderNo ratings yet
- 9.myelodysplastic Syndromes (MDS)Document21 pages9.myelodysplastic Syndromes (MDS)Safi UllahNo ratings yet
- 531 (1999) T. R. Golub: Science Et AlDocument8 pages531 (1999) T. R. Golub: Science Et AlBair PuigNo ratings yet
- Leukaemia Cutis in A 12-Year-Old Boy With Acute Myeloid LeukemiaDocument7 pagesLeukaemia Cutis in A 12-Year-Old Boy With Acute Myeloid LeukemiafikriafisNo ratings yet
- MUST To KNOW in Immunohematology Blood BankingDocument42 pagesMUST To KNOW in Immunohematology Blood BankingMerhella Amor Suerte MendozaNo ratings yet
- Review Article WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 4th EditionDocument8 pagesReview Article WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues 4th EditionCat NhanNo ratings yet
- Leukemia Panel Sample ReportDocument2 pagesLeukemia Panel Sample ReportAnmol DubeyNo ratings yet
- Etiology of Gingivitis: September 2011Document19 pagesEtiology of Gingivitis: September 2011Phúc BùiNo ratings yet
- Resident Autopsy LogDocument5 pagesResident Autopsy LogrboumendjelNo ratings yet
- Conference On Aml Date 13072024Document2 pagesConference On Aml Date 13072024Sanjaykumar YadavNo ratings yet
- PANCYTOPENIADocument51 pagesPANCYTOPENIAResmyNo ratings yet
- Pathology Revision E6.5Document129 pagesPathology Revision E6.5massprithiv58No ratings yet
- Mouse Models of Cancer Methods and Protocols Methods in Molecular Biology 2773 1St Edition Maja Cemazar Online Ebook Texxtbook Full Chapter PDFDocument69 pagesMouse Models of Cancer Methods and Protocols Methods in Molecular Biology 2773 1St Edition Maja Cemazar Online Ebook Texxtbook Full Chapter PDFruth.eyer418100% (10)
- Hema Part 3 Final PDFDocument188 pagesHema Part 3 Final PDFH.B.ANo ratings yet
- Flow Cytometry in Neoplastic Hematology. Morphologic-Immunophen Otypic-Genetic Correlation 4th Edition Wojciech GorczycaDocument70 pagesFlow Cytometry in Neoplastic Hematology. Morphologic-Immunophen Otypic-Genetic Correlation 4th Edition Wojciech Gorczycaperlamissing899100% (7)
- 2.acknowledgement and Def Disease CompleteDocument18 pages2.acknowledgement and Def Disease CompleteStephanie Joy EscalaNo ratings yet
- Invasive Pulmonary Aspergillosis - Semin Respir Crit Care Med 2020Document19 pagesInvasive Pulmonary Aspergillosis - Semin Respir Crit Care Med 2020MICHAEL AMARILLO CORREANo ratings yet