
Sameer Anatomy
Sameer Anatomy
You might also like
- Ana202 - Gross Anatomy of The Abdominal Esophagus Ans Stomach Gross 2021 (Autosaved) (Autosaved)Document45 pagesAna202 - Gross Anatomy of The Abdominal Esophagus Ans Stomach Gross 2021 (Autosaved) (Autosaved)ezekieldare91No ratings yet
- Anatomy of Stomach: Name:-Saumya Singh Roll: - 83 Bds 1 Yr BidshDocument22 pagesAnatomy of Stomach: Name:-Saumya Singh Roll: - 83 Bds 1 Yr BidshHiteshNo ratings yet
- StomachDocument24 pagesStomachHarini KarthikeyanNo ratings yet
- Anatomy of StomachDocument58 pagesAnatomy of StomachSkinny tuberNo ratings yet
- The Small Intestine-1Document38 pagesThe Small Intestine-1ChiderahNo ratings yet
- Digestive System (2015 - 06 - 09 20 - 43 - 48 Utc)Document90 pagesDigestive System (2015 - 06 - 09 20 - 43 - 48 Utc)DiazNo ratings yet
- The StomachDocument3 pagesThe StomachAhmad BdeirNo ratings yet
- Stomac 1Document28 pagesStomac 1BonzowoNo ratings yet
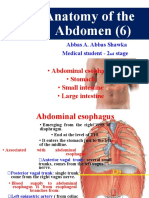
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Digestive SystemDocument64 pagesDigestive SystemAyro Business CenterNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- Abdomen Part IDocument110 pagesAbdomen Part IAbel GirmaNo ratings yet
- 1 Anerior Abdominl WLL Os Witout RecordDocument60 pages1 Anerior Abdominl WLL Os Witout Recordomeryou2004No ratings yet
- LO1 Anatomy and Histology of Lower Gi TractDocument180 pagesLO1 Anatomy and Histology of Lower Gi TractIcarus WingsNo ratings yet
- STOMACHDocument13 pagesSTOMACHNOOB GAM1NGNo ratings yet
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaNo ratings yet
- Anatomy of The AbdomenDocument107 pagesAnatomy of The AbdomenmichaelhossianNo ratings yet
- Digestive SystemDocument106 pagesDigestive Systemshahzaibzafargondal11786No ratings yet
- Slides - GITDocument68 pagesSlides - GITSalman KhanNo ratings yet
- StomachDocument24 pagesStomachesra1altahirNo ratings yet
- Abdo. VisceraDocument123 pagesAbdo. VisceraDureti DuretiNo ratings yet
- Overview of The Gastro Intestinal System: For Pc-I Medicine Students By: Zelalem. ADocument55 pagesOverview of The Gastro Intestinal System: For Pc-I Medicine Students By: Zelalem. AAmanuel MaruNo ratings yet
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuNo ratings yet
- Digestive System SummarisedDocument10 pagesDigestive System SummarisedJanetNo ratings yet
- Definition.: The Human Digestive SystemDocument32 pagesDefinition.: The Human Digestive SystemEmma Joel OtaiNo ratings yet
- 3 Stomach & Small Intestine Oct 2017Document50 pages3 Stomach & Small Intestine Oct 2017mayankNo ratings yet
- Anatomy of The Abdomen (1) : - IntroductionDocument21 pagesAnatomy of The Abdomen (1) : - IntroductionMunachande KanondoNo ratings yet
- Stomach: DR Kavitha M Kjiar (Savli)Document52 pagesStomach: DR Kavitha M Kjiar (Savli)Dhaval Chauhan0% (1)
- Name - Asha SharmaDocument15 pagesName - Asha SharmapraveenkumarnitkkrNo ratings yet
- Digestive TractDocument51 pagesDigestive Tractnimonayoseph27No ratings yet
- Lecture 12Document4 pagesLecture 12A-Naeem To'mah Al-sawaieNo ratings yet
- AbdomenDocument26 pagesAbdomenOlivia Chandra DeviNo ratings yet
- Anatomy of The EsophagusDocument14 pagesAnatomy of The EsophagusroselynroukayaNo ratings yet
- Anatomy of Lower Digestive SystemDocument85 pagesAnatomy of Lower Digestive SystemjoshinafaccNo ratings yet
- Lecture 4-Stomach - Parts of StomachDocument34 pagesLecture 4-Stomach - Parts of Stomachsamiiikhan5264No ratings yet
- STOMACHDocument20 pagesSTOMACHChoudhary FahadNo ratings yet
- Gi AnatomyDocument67 pagesGi AnatomyasyanadhikaryNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- LEC. 4&5. Digestive SystemDocument65 pagesLEC. 4&5. Digestive Systemmay498550No ratings yet
- The StomachDocument3 pagesThe StomachSanjay KishoreNo ratings yet
- StomachDocument29 pagesStomachSupriti Verma Bhatnagar100% (1)
- 8.3rd-copyDocument19 pages8.3rd-copysarakhaled1104No ratings yet
- PeritoneumDocument39 pagesPeritoneumtuhinsinghNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Abdominal Plain Film Radiography For Emergency Cases: Preceptor: Dr. NOVITA Sp. RadDocument50 pagesAbdominal Plain Film Radiography For Emergency Cases: Preceptor: Dr. NOVITA Sp. RadViviAnisaPutriNo ratings yet
- Abdominal Assessment: Jonalyn S. Esco,.Rn.,ManDocument77 pagesAbdominal Assessment: Jonalyn S. Esco,.Rn.,ManClifford Subagan Patil-aoNo ratings yet
- Peritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianDocument24 pagesPeritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianCristina GrajdeanNo ratings yet
- Digestive System Moath Nairat, MDDocument90 pagesDigestive System Moath Nairat, MDRaj KumarNo ratings yet
- Abdominal Organs Essay SolutionDocument77 pagesAbdominal Organs Essay SolutionEmmanuel IshiomaNo ratings yet
- 3.digestive SystemDocument103 pages3.digestive Systemokoti.omutanyi22No ratings yet
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaNo ratings yet
- Histology of Gastrointestinal TractDocument46 pagesHistology of Gastrointestinal Tractandreas kevinNo ratings yet
- Anatomy of OesophagusDocument57 pagesAnatomy of Oesophagusmel_anshul100% (1)
- Git Joy - 022307Document87 pagesGit Joy - 022307ayashanpNo ratings yet
- Digestive SystemDocument43 pagesDigestive SystemSimply MiniNo ratings yet
- Abdomen - Esophagus To ColonDocument42 pagesAbdomen - Esophagus To ColonBibek GajmerNo ratings yet
- 1 KidneyDocument49 pages1 Kidneywcbkk4vt9fNo ratings yet
- My StomachDocument24 pagesMy StomachPriya GKNo ratings yet
- Digestive System MLTDocument27 pagesDigestive System MLTAbdulrahman MohammedNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- نموذج ميزانية تدريبDocument2 pagesنموذج ميزانية تدريبعمولةNo ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)
- Cheadle Area Committee 15th March 2016Document176 pagesCheadle Area Committee 15th March 2016IainRobertsNo ratings yet
- Ethics in Healthcare Setting (Therapy)Document10 pagesEthics in Healthcare Setting (Therapy)Milcah ShabanjiNo ratings yet
- Definition of Terms Mine SurveyingDocument2 pagesDefinition of Terms Mine Surveyingaquariuspj25100% (3)
- Tendon Transfers in Foot Drop: Sridhar Krishnamurthy Mohamed IbrahimDocument9 pagesTendon Transfers in Foot Drop: Sridhar Krishnamurthy Mohamed IbrahimHuseyinSahinNo ratings yet
- Wastewater Characteristics: Table 7.1.5 Table 7.1.6Document4 pagesWastewater Characteristics: Table 7.1.5 Table 7.1.6Amin EnviroNo ratings yet
- Learning & Teaching MethodologyDocument17 pagesLearning & Teaching MethodologyVaidya Gautham M33% (6)
- Domestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentDocument35 pagesDomestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentirayoNo ratings yet
- Supreme Court Case Analysis - Vishaka and Ors v. State of Rajasthan and Ors by - Kavisha Gupta - Latest LawsDocument2 pagesSupreme Court Case Analysis - Vishaka and Ors v. State of Rajasthan and Ors by - Kavisha Gupta - Latest LawsAdv Akshay KshirsagarNo ratings yet
- Three Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphDocument10 pagesThree Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphLuluk NafisahNo ratings yet
- Review of Agriculture Robotics: Practicality and FeasibilityDocument6 pagesReview of Agriculture Robotics: Practicality and Feasibilityaldy faleraNo ratings yet
- 2 2 Bioaivers ExperienceDocument80 pages2 2 Bioaivers Experienceblashyrkh_79No ratings yet
- Vibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsDocument44 pagesVibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsSeres KozmicNo ratings yet
- Annex 3 - 5-Revised EMFDocument3 pagesAnnex 3 - 5-Revised EMFVholts Villa VitugNo ratings yet
- Epaper 20 October 2022Document22 pagesEpaper 20 October 2022Tauya DauramanziNo ratings yet
- Final DraftDocument37 pagesFinal DraftMorareng MariettaNo ratings yet
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- E Mannual Temperate Fruits 1Document44 pagesE Mannual Temperate Fruits 1gamerrr.mahiNo ratings yet
- Supply Chain Risk Management - A Literature Review (Final)Document55 pagesSupply Chain Risk Management - A Literature Review (Final)Rizki Agam SyahputraNo ratings yet
- Set3 PDFDocument36 pagesSet3 PDFvishwas100% (1)
- Barrel Firing - Paul WandlessDocument9 pagesBarrel Firing - Paul WandlessStefan Van Cleemput0% (1)
- 1A Innledning - EPS - Flyer - 2 - Jan - VaslestadDocument4 pages1A Innledning - EPS - Flyer - 2 - Jan - VaslestadNCS40 Trương Quốc BảoNo ratings yet
- Mushroom BoardsDocument4 pagesMushroom BoardsRemyaNo ratings yet
- Sala Ta Orn Dam Bill of QuantitiesDocument38 pagesSala Ta Orn Dam Bill of QuantitiesSothearaThengNo ratings yet
- Nutri QuizDocument26 pagesNutri QuizChona Candace Christian AndalNo ratings yet
- Build 443Document5 pagesBuild 443mh_tadayonNo ratings yet
- Clinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What IsDocument5 pagesClinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What Isarranguezjr5991No ratings yet
- CPM 0250 Water Pumping System Using River Force DevDocument9 pagesCPM 0250 Water Pumping System Using River Force DevmanjunathNo ratings yet
- TLE Cookery10 Q4 W3 V4Document7 pagesTLE Cookery10 Q4 W3 V4Maria Rose Tariga Aquino100% (2)





















































































Download as pptx, pdf, or txt
You might also like
- Ana202 - Gross Anatomy of The Abdominal Esophagus Ans Stomach Gross 2021 (Autosaved) (Autosaved)Document45 pagesAna202 - Gross Anatomy of The Abdominal Esophagus Ans Stomach Gross 2021 (Autosaved) (Autosaved)ezekieldare91No ratings yet
- Anatomy of Stomach: Name:-Saumya Singh Roll: - 83 Bds 1 Yr BidshDocument22 pagesAnatomy of Stomach: Name:-Saumya Singh Roll: - 83 Bds 1 Yr BidshHiteshNo ratings yet
- StomachDocument24 pagesStomachHarini KarthikeyanNo ratings yet
- Anatomy of StomachDocument58 pagesAnatomy of StomachSkinny tuberNo ratings yet
- The Small Intestine-1Document38 pagesThe Small Intestine-1ChiderahNo ratings yet
- Digestive System (2015 - 06 - 09 20 - 43 - 48 Utc)Document90 pagesDigestive System (2015 - 06 - 09 20 - 43 - 48 Utc)DiazNo ratings yet
- The StomachDocument3 pagesThe StomachAhmad BdeirNo ratings yet
- Stomac 1Document28 pagesStomac 1BonzowoNo ratings yet
- Anatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineDocument34 pagesAnatomy of The Abdomen (6) : - Abdominal Esophagus - Stomach - Small Intestine - Large IntestineBilal YimamNo ratings yet
- Digestive SystemDocument64 pagesDigestive SystemAyro Business CenterNo ratings yet
- Abdominal AnatomyDocument39 pagesAbdominal AnatomyRahul MandhanNo ratings yet
- Abdomen Part IDocument110 pagesAbdomen Part IAbel GirmaNo ratings yet
- 1 Anerior Abdominl WLL Os Witout RecordDocument60 pages1 Anerior Abdominl WLL Os Witout Recordomeryou2004No ratings yet
- LO1 Anatomy and Histology of Lower Gi TractDocument180 pagesLO1 Anatomy and Histology of Lower Gi TractIcarus WingsNo ratings yet
- STOMACHDocument13 pagesSTOMACHNOOB GAM1NGNo ratings yet
- Anatomi Dan Histologi Saluran Cerna BawahDocument20 pagesAnatomi Dan Histologi Saluran Cerna BawahIlhamDevirxaNo ratings yet
- Anatomy of The AbdomenDocument107 pagesAnatomy of The AbdomenmichaelhossianNo ratings yet
- Digestive SystemDocument106 pagesDigestive Systemshahzaibzafargondal11786No ratings yet
- Slides - GITDocument68 pagesSlides - GITSalman KhanNo ratings yet
- StomachDocument24 pagesStomachesra1altahirNo ratings yet
- Abdo. VisceraDocument123 pagesAbdo. VisceraDureti DuretiNo ratings yet
- Overview of The Gastro Intestinal System: For Pc-I Medicine Students By: Zelalem. ADocument55 pagesOverview of The Gastro Intestinal System: For Pc-I Medicine Students By: Zelalem. AAmanuel MaruNo ratings yet
- ANAT 221 - PeritoneumDocument22 pagesANAT 221 - PeritoneumWisdom IkechukwuNo ratings yet
- Digestive System SummarisedDocument10 pagesDigestive System SummarisedJanetNo ratings yet
- Definition.: The Human Digestive SystemDocument32 pagesDefinition.: The Human Digestive SystemEmma Joel OtaiNo ratings yet
- 3 Stomach & Small Intestine Oct 2017Document50 pages3 Stomach & Small Intestine Oct 2017mayankNo ratings yet
- Anatomy of The Abdomen (1) : - IntroductionDocument21 pagesAnatomy of The Abdomen (1) : - IntroductionMunachande KanondoNo ratings yet
- Stomach: DR Kavitha M Kjiar (Savli)Document52 pagesStomach: DR Kavitha M Kjiar (Savli)Dhaval Chauhan0% (1)
- Name - Asha SharmaDocument15 pagesName - Asha SharmapraveenkumarnitkkrNo ratings yet
- Digestive TractDocument51 pagesDigestive Tractnimonayoseph27No ratings yet
- Lecture 12Document4 pagesLecture 12A-Naeem To'mah Al-sawaieNo ratings yet
- AbdomenDocument26 pagesAbdomenOlivia Chandra DeviNo ratings yet
- Anatomy of The EsophagusDocument14 pagesAnatomy of The EsophagusroselynroukayaNo ratings yet
- Anatomy of Lower Digestive SystemDocument85 pagesAnatomy of Lower Digestive SystemjoshinafaccNo ratings yet
- Lecture 4-Stomach - Parts of StomachDocument34 pagesLecture 4-Stomach - Parts of Stomachsamiiikhan5264No ratings yet
- STOMACHDocument20 pagesSTOMACHChoudhary FahadNo ratings yet
- Gi AnatomyDocument67 pagesGi AnatomyasyanadhikaryNo ratings yet
- 1 Abdominal VisceraDocument45 pages1 Abdominal VisceraMero HamedNo ratings yet
- LEC. 4&5. Digestive SystemDocument65 pagesLEC. 4&5. Digestive Systemmay498550No ratings yet
- The StomachDocument3 pagesThe StomachSanjay KishoreNo ratings yet
- StomachDocument29 pagesStomachSupriti Verma Bhatnagar100% (1)
- 8.3rd-copyDocument19 pages8.3rd-copysarakhaled1104No ratings yet
- PeritoneumDocument39 pagesPeritoneumtuhinsinghNo ratings yet
- Abdominal CavityDocument78 pagesAbdominal Cavitytanishapatel1005No ratings yet
- Abdominal Plain Film Radiography For Emergency Cases: Preceptor: Dr. NOVITA Sp. RadDocument50 pagesAbdominal Plain Film Radiography For Emergency Cases: Preceptor: Dr. NOVITA Sp. RadViviAnisaPutriNo ratings yet
- Abdominal Assessment: Jonalyn S. Esco,.Rn.,ManDocument77 pagesAbdominal Assessment: Jonalyn S. Esco,.Rn.,ManClifford Subagan Patil-aoNo ratings yet
- Peritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianDocument24 pagesPeritoneum. Development of The Digestive System: Department of Human Anatomy Lecturer Dr. Globa LilianCristina GrajdeanNo ratings yet
- Digestive System Moath Nairat, MDDocument90 pagesDigestive System Moath Nairat, MDRaj KumarNo ratings yet
- Abdominal Organs Essay SolutionDocument77 pagesAbdominal Organs Essay SolutionEmmanuel IshiomaNo ratings yet
- 3.digestive SystemDocument103 pages3.digestive Systemokoti.omutanyi22No ratings yet
- Anatomy and Histology Gaster - DuodenumDocument149 pagesAnatomy and Histology Gaster - DuodenumRevila AuliaNo ratings yet
- Histology of Gastrointestinal TractDocument46 pagesHistology of Gastrointestinal Tractandreas kevinNo ratings yet
- Anatomy of OesophagusDocument57 pagesAnatomy of Oesophagusmel_anshul100% (1)
- Git Joy - 022307Document87 pagesGit Joy - 022307ayashanpNo ratings yet
- Digestive SystemDocument43 pagesDigestive SystemSimply MiniNo ratings yet
- Abdomen - Esophagus To ColonDocument42 pagesAbdomen - Esophagus To ColonBibek GajmerNo ratings yet
- 1 KidneyDocument49 pages1 Kidneywcbkk4vt9fNo ratings yet
- My StomachDocument24 pagesMy StomachPriya GKNo ratings yet
- Digestive System MLTDocument27 pagesDigestive System MLTAbdulrahman MohammedNo ratings yet
- Intestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandIntestinal Diseases, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- نموذج ميزانية تدريبDocument2 pagesنموذج ميزانية تدريبعمولةNo ratings yet
- Manual of Temporal Bone DissectionDocument82 pagesManual of Temporal Bone DissectionBungbu Tn100% (4)
- Cheadle Area Committee 15th March 2016Document176 pagesCheadle Area Committee 15th March 2016IainRobertsNo ratings yet
- Ethics in Healthcare Setting (Therapy)Document10 pagesEthics in Healthcare Setting (Therapy)Milcah ShabanjiNo ratings yet
- Definition of Terms Mine SurveyingDocument2 pagesDefinition of Terms Mine Surveyingaquariuspj25100% (3)
- Tendon Transfers in Foot Drop: Sridhar Krishnamurthy Mohamed IbrahimDocument9 pagesTendon Transfers in Foot Drop: Sridhar Krishnamurthy Mohamed IbrahimHuseyinSahinNo ratings yet
- Wastewater Characteristics: Table 7.1.5 Table 7.1.6Document4 pagesWastewater Characteristics: Table 7.1.5 Table 7.1.6Amin EnviroNo ratings yet
- Learning & Teaching MethodologyDocument17 pagesLearning & Teaching MethodologyVaidya Gautham M33% (6)
- Domestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentDocument35 pagesDomestic Dogs: Temporal Range: at Least 14,200 Years Ago - PresentirayoNo ratings yet
- Supreme Court Case Analysis - Vishaka and Ors v. State of Rajasthan and Ors by - Kavisha Gupta - Latest LawsDocument2 pagesSupreme Court Case Analysis - Vishaka and Ors v. State of Rajasthan and Ors by - Kavisha Gupta - Latest LawsAdv Akshay KshirsagarNo ratings yet
- Three Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphDocument10 pagesThree Main Parts of An Essay: An Introductory Paragraph A Body A Concluding ParagraphLuluk NafisahNo ratings yet
- Review of Agriculture Robotics: Practicality and FeasibilityDocument6 pagesReview of Agriculture Robotics: Practicality and Feasibilityaldy faleraNo ratings yet
- 2 2 Bioaivers ExperienceDocument80 pages2 2 Bioaivers Experienceblashyrkh_79No ratings yet
- Vibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsDocument44 pagesVibrant Yet Under-Resourced: The State of Lesbian, Bisexual, and Queer MovementsSeres KozmicNo ratings yet
- Annex 3 - 5-Revised EMFDocument3 pagesAnnex 3 - 5-Revised EMFVholts Villa VitugNo ratings yet
- Epaper 20 October 2022Document22 pagesEpaper 20 October 2022Tauya DauramanziNo ratings yet
- Final DraftDocument37 pagesFinal DraftMorareng MariettaNo ratings yet
- Astrological Study of Infertility - ConclusionDocument9 pagesAstrological Study of Infertility - ConclusionAnamika SNo ratings yet
- E Mannual Temperate Fruits 1Document44 pagesE Mannual Temperate Fruits 1gamerrr.mahiNo ratings yet
- Supply Chain Risk Management - A Literature Review (Final)Document55 pagesSupply Chain Risk Management - A Literature Review (Final)Rizki Agam SyahputraNo ratings yet
- Set3 PDFDocument36 pagesSet3 PDFvishwas100% (1)
- Barrel Firing - Paul WandlessDocument9 pagesBarrel Firing - Paul WandlessStefan Van Cleemput0% (1)
- 1A Innledning - EPS - Flyer - 2 - Jan - VaslestadDocument4 pages1A Innledning - EPS - Flyer - 2 - Jan - VaslestadNCS40 Trương Quốc BảoNo ratings yet
- Mushroom BoardsDocument4 pagesMushroom BoardsRemyaNo ratings yet
- Sala Ta Orn Dam Bill of QuantitiesDocument38 pagesSala Ta Orn Dam Bill of QuantitiesSothearaThengNo ratings yet
- Nutri QuizDocument26 pagesNutri QuizChona Candace Christian AndalNo ratings yet
- Build 443Document5 pagesBuild 443mh_tadayonNo ratings yet
- Clinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What IsDocument5 pagesClinical Liver Disease - 2022 - Memel - Intermittent Fasting As A Treatment For Nonalcoholic Fatty Liver Disease What Isarranguezjr5991No ratings yet
- CPM 0250 Water Pumping System Using River Force DevDocument9 pagesCPM 0250 Water Pumping System Using River Force DevmanjunathNo ratings yet
- TLE Cookery10 Q4 W3 V4Document7 pagesTLE Cookery10 Q4 W3 V4Maria Rose Tariga Aquino100% (2)