Download as pptx, pdf, or txt
You might also like
- SEEK/Pulmonary Board ReviewDocument34 pagesSEEK/Pulmonary Board ReviewAzmachamberAzmacareNo ratings yet
- Structured Clinical Interview For DSM-IV Axis I DisordersDocument223 pagesStructured Clinical Interview For DSM-IV Axis I DisordersΕιρηνη Κουτσοδοντη100% (2)
- Upper GI BleedingDocument30 pagesUpper GI BleedingBibek GhimireNo ratings yet
- Upper GIB Lecture and Presentation.Document75 pagesUpper GIB Lecture and Presentation.Williams Emmanuel AdeyeyeNo ratings yet
- Hematemesis, Melena, HematoscheziaDocument48 pagesHematemesis, Melena, HematoscheziaSyarifah FauziahNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibdiaNo ratings yet
- Gi Emergencies SeminarDocument122 pagesGi Emergencies SeminarShubham gaurNo ratings yet
- Prepared by Inzar Yasin Ammar LabibDocument47 pagesPrepared by Inzar Yasin Ammar LabibJohn Clements Galiza100% (1)
- Gastrointestinal BleedingDocument35 pagesGastrointestinal Bleedingtheeba 19No ratings yet
- Upper Gi BleedDocument43 pagesUpper Gi BleedPreethi GudipalliNo ratings yet
- Liver CirrhosisDocument9 pagesLiver CirrhosismedsmracelisNo ratings yet
- UGIBDocument24 pagesUGIBayoub hasandNo ratings yet
- Upper Gastrointestinal Bleeding 2007Document43 pagesUpper Gastrointestinal Bleeding 2007Matthew ThompsonNo ratings yet
- Cholangitis: Reported By: R. DongaranDocument18 pagesCholangitis: Reported By: R. DongaranVishnu Karunakaran100% (1)
- AscitesDocument71 pagesAscitessohilaw210No ratings yet
- Management of Acute Upper GI Bleeding BM TijjaniDocument71 pagesManagement of Acute Upper GI Bleeding BM Tijjaniadamu mohammadNo ratings yet
- Clinical Clerk Seminar Series: Approach To Gi BleedsDocument11 pagesClinical Clerk Seminar Series: Approach To Gi BleedsAngel_Liboon_388No ratings yet
- Upper Gastrointestinal BleedingDocument46 pagesUpper Gastrointestinal BleedingRashed ShatnawiNo ratings yet
- Hematemesis Melena (Upper Gi Bleeding)Document134 pagesHematemesis Melena (Upper Gi Bleeding)Mardoni Efrijon100% (1)
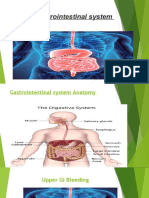
- Gastrointestinal SystemDocument26 pagesGastrointestinal SystemYazan HabaibyNo ratings yet
- Portal Hypertension: - DR Sunil Kumar .K.PDocument59 pagesPortal Hypertension: - DR Sunil Kumar .K.PSunil YalodahalliNo ratings yet
- Git BleedingDocument31 pagesGit BleedingWisdom NjumwaNo ratings yet
- Acute and Chronic Gastrointestinal BleedingDocument7 pagesAcute and Chronic Gastrointestinal BleedingMarwan M.100% (1)
- Acute AbdomenDocument60 pagesAcute AbdomenAnish DhamiNo ratings yet
- Massive Upper Gastrointestinal HemorrhageDocument73 pagesMassive Upper Gastrointestinal HemorrhageDONALD UNASHENo ratings yet
- Gi BleedingDocument74 pagesGi Bleedingponcus payNo ratings yet
- Gastroentrology بالشرحDocument103 pagesGastroentrology بالشرحMahmoud AbouelsoudNo ratings yet
- GIT BleedingDocument7 pagesGIT Bleedingفاطمة عبدالخالقNo ratings yet
- Case Report - GAVE On Chronic Kidney Disease and Chronic Hepatitis BDocument14 pagesCase Report - GAVE On Chronic Kidney Disease and Chronic Hepatitis BDolly JazmiNo ratings yet
- Gastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-IDocument74 pagesGastrointestinal Bleeding: Dr. Székely Hajnal 2nd Department of Internal Medicine 2015/16-ISutisna NisaNo ratings yet
- 6 Kuliah Liver CirrhosisDocument55 pages6 Kuliah Liver CirrhosisAnonymous vUEDx8100% (1)
- Et. 2.perdarhan Saluran CernaDocument69 pagesEt. 2.perdarhan Saluran CernaMarpaung LizaNo ratings yet
- Gastroduodenal Disorders: Suazo, Trisha Mae S. 3BSN-ADocument12 pagesGastroduodenal Disorders: Suazo, Trisha Mae S. 3BSN-AKenneth OpinaNo ratings yet
- Gastrointestinal Bleeding - StatPearls - NCBI BookshelfDocument7 pagesGastrointestinal Bleeding - StatPearls - NCBI BookshelfAdam GenturNo ratings yet
- Upper Gi BleedingDocument37 pagesUpper Gi Bleedingfathima AlfasNo ratings yet
- 6868841Document35 pages6868841malik003No ratings yet
- GIT Portal HypertensionDocument24 pagesGIT Portal HypertensionDr.P.NatarajanNo ratings yet
- Litiasis VesicularDocument26 pagesLitiasis VesicularEULER FARADAY ALTAMIRANO FARFANNo ratings yet
- Upper GI Bleed - SymposiumDocument38 pagesUpper GI Bleed - SymposiumSopna ZenithNo ratings yet
- Jaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Document46 pagesJaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Nurlaila ElaNo ratings yet
- Biliary Emergencies: Murad AljiffryDocument50 pagesBiliary Emergencies: Murad AljiffryastridwiparamitaNo ratings yet
- Case Alcohol Abuse and Unusual Abdominal Pain in A 49-Year-OldDocument7 pagesCase Alcohol Abuse and Unusual Abdominal Pain in A 49-Year-OldPutri AmeliaNo ratings yet
- ULGIBDocument31 pagesULGIBEzraNo ratings yet
- The Diagnostic Work-Up in Patients With Ascites Current Guidelines and Future ProspectsDocument6 pagesThe Diagnostic Work-Up in Patients With Ascites Current Guidelines and Future ProspectsCAMILO FERRERO RESTREPONo ratings yet
- Ascietes by DR Naila MasoodDocument45 pagesAscietes by DR Naila MasoodmichelleNo ratings yet
- Day 10. Choledocholitiasis, CholangitisDocument26 pagesDay 10. Choledocholitiasis, Cholangitisهنادي رازمNo ratings yet
- 프레젠테이션 5Document8 pages프레젠테이션 5LEENo ratings yet
- Anemia Sec To UGIBDocument32 pagesAnemia Sec To UGIBJose Fernando Gregana ElpaNo ratings yet
- Lange Current Emergency Medicine - GI Bleed ChapterDocument3 pagesLange Current Emergency Medicine - GI Bleed ChaptercrystalsheNo ratings yet
- The Diagnostic Work-Up in Patients With Ascites: Current Guidelines and Future ProspectsDocument7 pagesThe Diagnostic Work-Up in Patients With Ascites: Current Guidelines and Future ProspectsRizqi AmaliaNo ratings yet
- Surgery CaseDocument4 pagesSurgery CaseVincent SomidoNo ratings yet
- AscitesDocument4 pagesAscitesmohannadNo ratings yet
- Acute Chronic PancreatitisDocument78 pagesAcute Chronic PancreatitisSirfaymons Sirfaymons Sirfaymons100% (2)
- Case Abdominal Pain in A 49-Year-OldDocument6 pagesCase Abdominal Pain in A 49-Year-OldPutri AmeliaNo ratings yet
- Jaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Document46 pagesJaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Edwin Jose SNo ratings yet
- GI Bleeding Team Work - 2nd EditionDocument9 pagesGI Bleeding Team Work - 2nd EditionUsman Ali AkbarNo ratings yet
- Surgery 2014.1Document25 pagesSurgery 2014.1Jayanti Neogi SardarNo ratings yet
- Upper Gi BleedingDocument30 pagesUpper Gi Bleedingiman naNo ratings yet
- Atul Sharma Uppergi Fcccm23Document47 pagesAtul Sharma Uppergi Fcccm23Atul SharmaNo ratings yet
- GI BleedDocument28 pagesGI BleedAnn Lan100% (1)
- Alert Medical Series: USMLE Alert I, II, IIIFrom EverandAlert Medical Series: USMLE Alert I, II, IIIRating: 2 out of 5 stars2/5 (1)
- Orthopaedic Instruments ImagesDocument40 pagesOrthopaedic Instruments ImagesKannan KannanNo ratings yet
- Mercury GroupDocument27 pagesMercury GroupAnjum AbbasiNo ratings yet
- Ped Surgery PPT 13th FebDocument46 pagesPed Surgery PPT 13th FebKASATSANo ratings yet
- Limb Defciency and Phantom Limb QuestionnaireDocument5 pagesLimb Defciency and Phantom Limb Questionnairenadia kurniaNo ratings yet
- Pe5 Lesson2Document27 pagesPe5 Lesson2LMChulipahNo ratings yet
- Cutaneous Larva MigransDocument5 pagesCutaneous Larva MigransdnoksNo ratings yet
- Coin in The Esophagus: General ConsiderationsDocument3 pagesCoin in The Esophagus: General ConsiderationsFreddy PanjaitanNo ratings yet
- Malignant NephrosclerosisDocument3 pagesMalignant NephrosclerosisIsfahan MasulotNo ratings yet
- CASE REPORT Hipokalemia HipokalsemiaDocument24 pagesCASE REPORT Hipokalemia HipokalsemiaRaraNo ratings yet
- Att 1446693658204 المذكرة-الذهبيةDocument80 pagesAtt 1446693658204 المذكرة-الذهبيةShady KhamisNo ratings yet
- Tocotrienols Science White Paper 1.12 en ALLDocument14 pagesTocotrienols Science White Paper 1.12 en ALLGreenshieldNo ratings yet
- Open Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Document3 pagesOpen Prostatectomy For Huge Prostates Our Experience in A Developing Country 2329 9088.1000132Ahmed Ben BellaNo ratings yet
- Overview of Guillain-Barré Syndrome: I. Literature ReviewDocument10 pagesOverview of Guillain-Barré Syndrome: I. Literature ReviewS Dian RNo ratings yet
- Case Presentation: - Vuppu BhavaniDocument53 pagesCase Presentation: - Vuppu BhavaniLohith Kumar MenchuNo ratings yet
- 5 08 5+sutadisastraDocument9 pages5 08 5+sutadisastradr daraNo ratings yet
- Test Bank For Physical Agents Theory and Practice 3rd Edition Barbara J Behrens Holly Beinert DownloadDocument11 pagesTest Bank For Physical Agents Theory and Practice 3rd Edition Barbara J Behrens Holly Beinert Downloadryanparker18011988fno100% (25)
- PALS Precourse Self-Assessment Score ReportDocument3 pagesPALS Precourse Self-Assessment Score ReportMaya LaPradeNo ratings yet
- Eye LidDocument8 pagesEye LidasmaelgathafiNo ratings yet
- Chain of Survival: Adult and Pediatric Out of Hospital Cardiac ArrestDocument10 pagesChain of Survival: Adult and Pediatric Out of Hospital Cardiac ArrestJapeth John M. FloresNo ratings yet
- StudiesDocument130 pagesStudiesShruti100% (2)
- HypertensionDocument11 pagesHypertensionArmina LagumbayNo ratings yet
- CT ScanDocument4 pagesCT Scant a khanNo ratings yet
- ALSANGEDY BULLETS FOR PACES HypogammaglobulinemiaDocument2 pagesALSANGEDY BULLETS FOR PACES HypogammaglobulinemiaushapadminivadivelswamyNo ratings yet
- Cephalosporins in Animals - DosagesDocument7 pagesCephalosporins in Animals - DosagesSunilNo ratings yet
- Brand Name: Dilantin Generic Name: Phenytoin Indication: Dilantin Is IndicatedDocument4 pagesBrand Name: Dilantin Generic Name: Phenytoin Indication: Dilantin Is Indicatedianecunar100% (1)
- 36.3C 60 CPM 3.5 KG 54 CM: Physical Examination and Review of SystemsDocument3 pages36.3C 60 CPM 3.5 KG 54 CM: Physical Examination and Review of SystemsDale ResurreccionNo ratings yet
- Benign Involuted Fibroadenoma NotesDocument3 pagesBenign Involuted Fibroadenoma NotesisensepanicNo ratings yet
- EMS Tens Pain Relief GuideDocument34 pagesEMS Tens Pain Relief GuideFrank Martin100% (4)