Download as pptx, pdf, or txt
You might also like
- Preclinical Pathology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1From EverandPreclinical Pathology Review 2023: For USMLE Step 1 and COMLEX-USA Level 1Rating: 5 out of 5 stars5/5 (1)
- Addison Disease: Diagnosis and Initial ManagementDocument4 pagesAddison Disease: Diagnosis and Initial ManagementTeguh RahNo ratings yet
- Types of Special NeedsDocument9 pagesTypes of Special NeedsThangaraj Msw100% (1)
- This Study Resource WasDocument3 pagesThis Study Resource WasSam CuevasNo ratings yet
- Alcohol Withdrawal Care PlanDocument1 pageAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- Insuficiencia AdrenalDocument5 pagesInsuficiencia AdrenalLuciana RafaelNo ratings yet
- Cushings SyndromeDocument18 pagesCushings SyndromeBijay SharmaNo ratings yet
- Adrenocortical DisordersDocument73 pagesAdrenocortical DisordersReunita ConstantiaNo ratings yet
- Depart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanDocument19 pagesDepart. Farmakologi Dan Terapeutik: Universitas Sumatera Utara-MedanMasyithah TetaNo ratings yet
- GroupA RenalDisordersDocument13 pagesGroupA RenalDisordersPaulNo ratings yet
- Addison SlidesDocument59 pagesAddison Slidesmarianatilla2016No ratings yet
- Liyon - Endocrine GlandDocument26 pagesLiyon - Endocrine GlandLiyon BasnetNo ratings yet
- Cushing SyndromeDocument8 pagesCushing SyndromeArun100% (1)
- Endo 2Document114 pagesEndo 2rediet shimekachNo ratings yet
- Adrenal Crisis FinalDocument10 pagesAdrenal Crisis FinalAmanda Scarlet100% (1)
- Tanpa JudulDocument14 pagesTanpa JudulAsrapia HubaisyingNo ratings yet
- Adrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing SyndromeDocument46 pagesAdrenal Gland: Adrenal Insufficiency, Addison Disease, Cushing Syndromeyuyu tuptupNo ratings yet
- 28-23 - Cushing Syndrome (Hypercortisolism)Document8 pages28-23 - Cushing Syndrome (Hypercortisolism)Sergio VasquezNo ratings yet
- Adrenal Diseases: Types Aetiology Diagnosis Complications TreatmentDocument29 pagesAdrenal Diseases: Types Aetiology Diagnosis Complications Treatmentgani7222No ratings yet
- Week 5 Endokrin WO - Michael GeraldilDocument5 pagesWeek 5 Endokrin WO - Michael GeraldilMichael GNo ratings yet
- Cushing SyndromeDocument5 pagesCushing Syndromearif mahammad bhuniyaNo ratings yet
- Cushing's SyndromeDocument9 pagesCushing's Syndromemuzamiljoyia07No ratings yet
- Updateonmanagementof Theoralandmaxillofacial Surgerypatienton CorticosteroidsDocument12 pagesUpdateonmanagementof Theoralandmaxillofacial Surgerypatienton CorticosteroidsFadi Al HajjiNo ratings yet
- Nbme 11 ExplainationDocument55 pagesNbme 11 Explainationazankhan9960% (10)
- Assignment of Adrenal CortexDocument12 pagesAssignment of Adrenal CortexWania AliNo ratings yet
- ENDO - Adrenal CrisisDocument8 pagesENDO - Adrenal CrisisHajime NakaegawaNo ratings yet
- Adrenal InsufficiencyDocument33 pagesAdrenal InsufficiencypukitagabNo ratings yet
- 30 Manuscript Addison's DiseaseDocument10 pages30 Manuscript Addison's Diseasekint manlangitNo ratings yet
- Adrenal Gland DisordersDocument31 pagesAdrenal Gland DisordersThe AbyssinicansNo ratings yet
- Addison Diseases LecDocument40 pagesAddison Diseases LecSalman RabbaniNo ratings yet
- Corticosteroids and Anabolic SteroidsDocument32 pagesCorticosteroids and Anabolic SteroidsSudhakar LakavathNo ratings yet
- 8.GUS For AHN II 2023Document117 pages8.GUS For AHN II 2023merga wekwayaNo ratings yet
- Adrenal InsufficiencyDocument11 pagesAdrenal InsufficiencyAustine OsaweNo ratings yet
- Review: Irina Bancos, Stefanie Hahner, Jeremy Tomlinson, Wiebke ArltDocument11 pagesReview: Irina Bancos, Stefanie Hahner, Jeremy Tomlinson, Wiebke Arltinterna MANADONo ratings yet
- Corticosteroids and Anabolic SteroidsDocument32 pagesCorticosteroids and Anabolic SteroidsSudhakar LakavathNo ratings yet
- Unmasking The Silent Menace A Case Report of Aldosterone Secreting Adrenal Cortical AdenomaDocument6 pagesUnmasking The Silent Menace A Case Report of Aldosterone Secreting Adrenal Cortical AdenomaAthenaeum Scientific PublishersNo ratings yet
- Adrenal Disorders - ClassDocument71 pagesAdrenal Disorders - ClassabinetbantiNo ratings yet
- Addison Disease: Diagnosis and Initial ManagementDocument5 pagesAddison Disease: Diagnosis and Initial ManagementI Gede SubagiaNo ratings yet
- Adrenal DisordersDocument29 pagesAdrenal DisordersSuliman Garalleh100% (1)
- EN8 - HypercortisolismDocument11 pagesEN8 - Hypercortisolismsbobine.imsNo ratings yet
- AdrenalsDocument35 pagesAdrenalsMohammed MustafaNo ratings yet
- Cushing SyndromDocument12 pagesCushing SyndromIka AnisaNo ratings yet
- Endocrinology Part 1Document131 pagesEndocrinology Part 1LucjaNo ratings yet
- Adrenal InsufficiencyDocument25 pagesAdrenal InsufficiencyMustafa Salam M.NooriNo ratings yet
- Internal Medicine Form 2:: Answers With Explanations From UptodateDocument11 pagesInternal Medicine Form 2:: Answers With Explanations From UptodateSelena GajićNo ratings yet
- Cushing Syndrome: M.Sc. (N) 1 YearDocument30 pagesCushing Syndrome: M.Sc. (N) 1 YearRanjana SharmaNo ratings yet
- Addison Ian Crisis JoGanDocument32 pagesAddison Ian Crisis JoGanJoseph Gan Say SeongNo ratings yet
- EndokrinDocument27 pagesEndokrinSarah Putri AbellysaNo ratings yet
- ENDOCRINE DISORDERS (Autosaved)Document81 pagesENDOCRINE DISORDERS (Autosaved)Princewill SeiyefaNo ratings yet
- Cushing SyndromeDocument16 pagesCushing SyndromeHemant Singh SaudNo ratings yet
- 632 Ijar-5063Document6 pages632 Ijar-5063Putri Rahmadhani Ngakpaniklage AsdsNo ratings yet
- Acute Biological CrisisDocument107 pagesAcute Biological CrisisJenes CernaNo ratings yet
- Definition - Cushing's Syndrome Is The Combination of Symptoms and SignsDocument4 pagesDefinition - Cushing's Syndrome Is The Combination of Symptoms and SignsSuhas IngaleNo ratings yet
- DKA To CRFDocument4 pagesDKA To CRFMark Anthony YabresNo ratings yet
- Renal Disorders Kulimankudya VascoDocument385 pagesRenal Disorders Kulimankudya VascoIan MurrithiNo ratings yet
- Glomerulonephritis 1Document2 pagesGlomerulonephritis 1Riny KhurshidNo ratings yet
- Nbme 11Document102 pagesNbme 11Mohamed Nabil100% (36)
- Physiology for General Surgical Sciences Examination (GSSE)From EverandPhysiology for General Surgical Sciences Examination (GSSE)S. Ali MirjaliliNo ratings yet
- Addison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandAddison’s Disease, A Simple Guide To The Condition, Treatment And Related ConditionsNo ratings yet
- Giant Cell Arteritis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandGiant Cell Arteritis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- 1 Moderna Clinical Study Report 16.2.7 Adverse Event Listing May 2021 11505 PagesDocument11,505 pages1 Moderna Clinical Study Report 16.2.7 Adverse Event Listing May 2021 11505 PagesPeeb SmithNo ratings yet
- Session Module DesignDocument7 pagesSession Module DesignLohrhen Lheighh CahreeniyowNo ratings yet
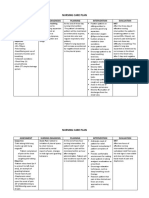
- Nursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationDocument4 pagesNursing Care Plan: Assessment Nursing Diagnosis Planning Intervention EvaluationGiddel Guerra PapellerasNo ratings yet
- Antibiotik Profilaksis DR Eko Setijanto 06032020 EditDocument40 pagesAntibiotik Profilaksis DR Eko Setijanto 06032020 EditFitria AgustianiNo ratings yet
- KNH 413 - Case Study 14Document17 pagesKNH 413 - Case Study 14api-301118772No ratings yet
- MnaDocument6 pagesMnaRanitya Hardian YunitaNo ratings yet
- Nine ExamDocument6 pagesNine ExamRoderick Beltran Lutang100% (1)
- Gayoso Position PaperDocument8 pagesGayoso Position PaperJayvee GayosoNo ratings yet
- Chapter IIDocument31 pagesChapter IIyssa_03No ratings yet
- Travel Clinics AustraliaDocument1 pageTravel Clinics AustraliaerkaNo ratings yet
- Phenylephrine HydrochlorideDocument5 pagesPhenylephrine HydrochlorideSean Amir S. Savellano100% (1)
- Vitamin D HandoutDocument2 pagesVitamin D Handoutapi-239305061No ratings yet
- NSTG EnglishDocument255 pagesNSTG EnglishMohammad SaidNo ratings yet
- Infection Control Policy ProceduresDocument8 pagesInfection Control Policy Proceduresdefa reyNo ratings yet
- Diabetes Management Through YogaDocument5 pagesDiabetes Management Through YogaDr. sireesh anumulaNo ratings yet
- Anti-HAV IgMDocument3 pagesAnti-HAV IgMHassan GillNo ratings yet
- STS Video ScriptDocument2 pagesSTS Video ScriptCynthia Y De VeraNo ratings yet
- Physical Education and HealthDocument6 pagesPhysical Education and HealthDiane BarbadoNo ratings yet
- 5.6a First Aid Box Treatment - Inspection RegisterDocument1 page5.6a First Aid Box Treatment - Inspection RegisterSn Ahsan100% (1)
- BSN 2-4 - 2V - MCN CASE STUDY (Final)Document100 pagesBSN 2-4 - 2V - MCN CASE STUDY (Final)Angeline ShackletonNo ratings yet
- Roleplay Admission - Kelompok 1 - Reg BDocument3 pagesRoleplay Admission - Kelompok 1 - Reg BQonitaaNo ratings yet
- 1 3 1 A SR AutopsyreportfDocument3 pages1 3 1 A SR Autopsyreportfapi-242811957No ratings yet
- Infections of Lacrimal PassagesDocument8 pagesInfections of Lacrimal PassagesgeorginaNo ratings yet
- A Drug Study On: Furosemide TabletDocument7 pagesA Drug Study On: Furosemide TabletRaijenne VersolaNo ratings yet
- Classification of Age-Related CataractDocument16 pagesClassification of Age-Related CataracttataNo ratings yet
- Pulse Rate ChecklistDocument2 pagesPulse Rate ChecklistPatrick SantosNo ratings yet
- Phelbotomy Technique: STEP 1: Prepare Accessioning Order For The PatientDocument13 pagesPhelbotomy Technique: STEP 1: Prepare Accessioning Order For The PatientNunai SalipadaNo ratings yet