Download as ppt, pdf, or txt
You might also like
- Oxford Handbook of CriminologyDocument15 pagesOxford Handbook of CriminologyRedAndSparkly71% (7)
- STUDENT COPD Pneumonia FUNDAMENTAL - Reasoning PDFDocument8 pagesSTUDENT COPD Pneumonia FUNDAMENTAL - Reasoning PDFYeny PenaNo ratings yet
- Intensive Care Nursery: House Staff ManualDocument187 pagesIntensive Care Nursery: House Staff ManualAna MariaNo ratings yet
- Relations and FunctionsDocument10 pagesRelations and Functionskiahjessie100% (6)
- Nursing Care PlanDocument2 pagesNursing Care PlanAl RizkyNo ratings yet
- Renal TransplantationDocument57 pagesRenal Transplantationapi-376028367% (3)
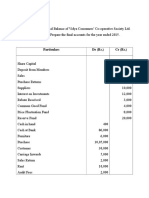
- Final AccountDocument7 pagesFinal Accountswati100% (3)
- Head Girl SpeechDocument1 pageHead Girl SpeechArtiBhalodia0% (1)
- ARDS Care Respiratory Care Plan PDFDocument2 pagesARDS Care Respiratory Care Plan PDFeric parlNo ratings yet
- Lecture 7 - Nosocomial PneumoniaDocument30 pagesLecture 7 - Nosocomial PneumoniaKartika Rezky100% (2)
- In The Name of ALLAH The Beneficent and MercifulDocument49 pagesIn The Name of ALLAH The Beneficent and Mercifulcute_honiya100% (1)
- ConstipationDocument80 pagesConstipationVilasineeAriHaraKumarNo ratings yet
- Physiology of Mechanical VentilationDocument12 pagesPhysiology of Mechanical VentilationCarlos ZepedaNo ratings yet
- PeritonitisDocument33 pagesPeritonitisnurulamaliahnutNo ratings yet
- Pathophysiology of AsthmaDocument71 pagesPathophysiology of AsthmaChin ChanNo ratings yet
- Sepsis Septic Shock The LectDocument95 pagesSepsis Septic Shock The LecthrmosalamNo ratings yet
- Your Body, Your Genes, Your Digestion, and Your MetabolismFrom EverandYour Body, Your Genes, Your Digestion, and Your MetabolismNo ratings yet
- Hospital Acquired PneumoniaDocument23 pagesHospital Acquired Pneumoniadarmarianto100% (1)
- A Simple Guide to Pneumothorax (Collapsed Lungs), Diagnosis, Treatment and Related ConditionsFrom EverandA Simple Guide to Pneumothorax (Collapsed Lungs), Diagnosis, Treatment and Related ConditionsNo ratings yet
- (MED II) 1.05 Emergencies in Cancer PatientsDocument17 pages(MED II) 1.05 Emergencies in Cancer PatientsJearwin AngelesNo ratings yet
- Chapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureDocument15 pagesChapter 42 - Sepsis, Septic Shock, and Multiple Organ FailureWorrawalun FuktongNo ratings yet
- Shock CorrectedDocument70 pagesShock CorrectedrajevikramNo ratings yet
- IM Clinics History 2Document4 pagesIM Clinics History 2LucyellowOttemoesoeNo ratings yet
- Infectious MononucleosisDocument35 pagesInfectious MononucleosisShv Naga100% (1)
- Rapid Sequence InductionDocument8 pagesRapid Sequence InductionAngela Mitchelle NyanganNo ratings yet
- Visual Guide to Neonatal CardiologyFrom EverandVisual Guide to Neonatal CardiologyErnerio T. AlbolirasNo ratings yet
- Nursing Care in Pediatric Respiratory DiseaseFrom EverandNursing Care in Pediatric Respiratory DiseaseConcettina TolomeoNo ratings yet
- Heart FailureDocument4 pagesHeart FailureBrynn MinaNo ratings yet
- Henoch Schonlein Purpura (IgA Vasculitis)Document15 pagesHenoch Schonlein Purpura (IgA Vasculitis)Emily Eresuma100% (1)
- Who Should Be Admitted To The Intensive Care UnitDocument5 pagesWho Should Be Admitted To The Intensive Care UnitKary VelazquezNo ratings yet
- COPD HarrisonsDocument45 pagesCOPD HarrisonsNogra CarlNo ratings yet
- 7..intravenous Anaesthesia 2Document23 pages7..intravenous Anaesthesia 2Mwiliza BrendaNo ratings yet
- Pulmonary Tuberculosis PharmacologyDocument48 pagesPulmonary Tuberculosis PharmacologyMarc Imhotep Cray, M.D.No ratings yet
- ModuleIV RespiratoryEmergencies CHF COPD AsthmaDocument96 pagesModuleIV RespiratoryEmergencies CHF COPD AsthmaSaiKiranNo ratings yet
- Management of Neonatal JaundiceDocument22 pagesManagement of Neonatal JaundiceSuhazeli Abdullah100% (1)
- Shock & Fluid TherapyDocument57 pagesShock & Fluid Therapyarnol3090No ratings yet
- By DR Mujahidah NaimDocument48 pagesBy DR Mujahidah NaimKlinik KodiangNo ratings yet
- Rapid Sequence IntubationDocument60 pagesRapid Sequence IntubationFlighterdoc100% (1)
- NIH Aids Info HIV Treatment Guidelines AdultandadolescentglDocument267 pagesNIH Aids Info HIV Treatment Guidelines Adultandadolescentglbmartindoyle6396No ratings yet
- Pyrexia of Unknown OriginDocument81 pagesPyrexia of Unknown OriginJithin Bhagavati Kalam100% (1)
- Peds Basic Principles Mechanical VentilationDocument39 pagesPeds Basic Principles Mechanical VentilationNav KovNo ratings yet
- Chronic Cough In Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandChronic Cough In Children, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Neonatal Circulation Changes / Unbalanced Circulation: Neonatal Cardiac Conditions: Medical and Surgical ManagementDocument4 pagesNeonatal Circulation Changes / Unbalanced Circulation: Neonatal Cardiac Conditions: Medical and Surgical ManagementAnita Maria UlfaNo ratings yet
- Pneumonia: Submitted To:Ms Lisette Cruz Submitted By: Ms. Mely Rose AbanadorDocument26 pagesPneumonia: Submitted To:Ms Lisette Cruz Submitted By: Ms. Mely Rose AbanadorJoyce Catherine Buquing UysecoNo ratings yet
- Approach To Neonatal JaundiceDocument36 pagesApproach To Neonatal JaundiceDrMubashir ShaikhNo ratings yet
- N.I.C.U.: Pocket Guide For Respiratory TherapistsDocument28 pagesN.I.C.U.: Pocket Guide For Respiratory Therapistsmichelleann_329No ratings yet
- Abdominal Masses in Pediatrics - 2015Document5 pagesAbdominal Masses in Pediatrics - 2015Jéssica VazNo ratings yet
- Respiratory EmergenciesDocument34 pagesRespiratory EmergenciesRoshana MallawaarachchiNo ratings yet
- Pediatric Incontinence: Evaluation and Clinical ManagementFrom EverandPediatric Incontinence: Evaluation and Clinical ManagementIsrael FrancoRating: 5 out of 5 stars5/5 (1)
- BronchiolitisDocument12 pagesBronchiolitisEz BallNo ratings yet
- Lecture#1 01-14-14 Why Is Nursing of Children Different?Document12 pagesLecture#1 01-14-14 Why Is Nursing of Children Different?nkuligowskiNo ratings yet
- PleurisyDocument25 pagesPleurisyAliNo ratings yet
- Pathophysiology of Birth AsphyxiaDocument14 pagesPathophysiology of Birth AsphyxiaEduardo Rios DuboisNo ratings yet
- Bronchial AsthmaDocument27 pagesBronchial AsthmachandrikaismailNo ratings yet
- Paediatrics Epileptiform DisordersDocument11 pagesPaediatrics Epileptiform DisordersayunisallehNo ratings yet
- Inhalation Therapy in Asthma and CopdDocument62 pagesInhalation Therapy in Asthma and Copdferi sulistyaNo ratings yet
- BronchiolitisDocument22 pagesBronchiolitisAlfani FajarNo ratings yet
- PNEUMONIADocument14 pagesPNEUMONIArogggNo ratings yet
- Neonatal Respiratory DistressDocument59 pagesNeonatal Respiratory DistressMohamad Saleh100% (7)
- Follow Up High Risk NBDocument36 pagesFollow Up High Risk NBinggrit anggrainiNo ratings yet
- Hepatobiliary DiseaseDocument52 pagesHepatobiliary DiseaseMelissa Laurenshia ThenataNo ratings yet
- Exenatide PDFDocument3 pagesExenatide PDFHam SotheaNo ratings yet
- I. Understanding The Disease and PathophysiologyDocument11 pagesI. Understanding The Disease and PathophysiologyFajer AleitanNo ratings yet
- Acute Respiratory Failure 1Document7 pagesAcute Respiratory Failure 1Trish 0019No ratings yet
- Asthma: Pio T. Esguerra II, MD, FPCP, FPCCP Pulmonary & Critical Care FEU-NRMF Medical CenterDocument98 pagesAsthma: Pio T. Esguerra II, MD, FPCP, FPCCP Pulmonary & Critical Care FEU-NRMF Medical CenteryayayanizaNo ratings yet
- Sleep Apnoea - Prof - DR K.K.PDocument44 pagesSleep Apnoea - Prof - DR K.K.PjialeongNo ratings yet
- Advanced Cardiac Life SupportDocument44 pagesAdvanced Cardiac Life Supporthafidh_hanifuddinNo ratings yet
- Update in Paediatric Resuscitation: 2005 International Guidelines: Recommendations From NRCDocument32 pagesUpdate in Paediatric Resuscitation: 2005 International Guidelines: Recommendations From NRCapi-3760283No ratings yet
- Field Visit Presentation by Jasmine Laila WingSeeDocument53 pagesField Visit Presentation by Jasmine Laila WingSeeapi-3760283No ratings yet
- Surgical Management of VSDDocument56 pagesSurgical Management of VSDapi-3760283100% (1)
- Singapore Defibrillation Guidelines 2006Document19 pagesSingapore Defibrillation Guidelines 2006api-3760283No ratings yet
- GI Bleeding - NursesDocument71 pagesGI Bleeding - Nursesapi-3760283100% (6)
- Model Aliansi Untuk Peningkatan Kualitas Pembelajaran Dan Penyerapan Kerja AlumniDocument16 pagesModel Aliansi Untuk Peningkatan Kualitas Pembelajaran Dan Penyerapan Kerja Alumniagung djibranNo ratings yet
- Dep Trai Loi Tai AiDocument192 pagesDep Trai Loi Tai AiHoàng Hồng DươngNo ratings yet
- Strategi Positioning Radio Mandiri 98,3 FM Sebagai Radio News and Business PekanbaruDocument8 pagesStrategi Positioning Radio Mandiri 98,3 FM Sebagai Radio News and Business PekanbaruAlipPervectSeihaNo ratings yet
- GAD When Did GAD Came Into Being?Document3 pagesGAD When Did GAD Came Into Being?John Alvin de LaraNo ratings yet
- Young - Coco Chanel Enseñanzas ModaDocument151 pagesYoung - Coco Chanel Enseñanzas ModaLuis Ángel Bejarano MaluquishNo ratings yet
- HCP Final DraftDocument9 pagesHCP Final Draftapi-439819651No ratings yet
- Week 1 TutorialDocument2 pagesWeek 1 TutorialsherlynNo ratings yet
- Mathematics: Quarter 2 - Module 4: Laws Involving Integral ExponentsDocument18 pagesMathematics: Quarter 2 - Module 4: Laws Involving Integral ExponentsShawee Gucor SaquilabonNo ratings yet
- A Failure of Focus - KodakDocument30 pagesA Failure of Focus - KodakchangumanguNo ratings yet
- Cover Letter For Job InterviewDocument8 pagesCover Letter For Job Interviewafdmgoqxi100% (1)
- Ann FLDocument102 pagesAnn FLdpkfatnani05No ratings yet
- GirlRising TeachersGuide Final PDFDocument93 pagesGirlRising TeachersGuide Final PDFCla RiseNo ratings yet
- Superstar Stamina How To Get Hard and Stay Hard GET YOUR BODY INTO SHAPE SO YOU'LL LOVE ITDocument78 pagesSuperstar Stamina How To Get Hard and Stay Hard GET YOUR BODY INTO SHAPE SO YOU'LL LOVE ITdominique marshallNo ratings yet
- Ilovepdf MergedDocument13 pagesIlovepdf Mergedbrendanyip1129No ratings yet
- 5 21 20 New York V Commerce OpinionDocument23 pages5 21 20 New York V Commerce OpinionLaw&CrimeNo ratings yet
- Hobsbawm and Ranger - The Invention of TraditionDocument330 pagesHobsbawm and Ranger - The Invention of TraditionIván Parada Hernández75% (4)
- Full Download Race and Ethnicity in The United States 8th Edition Schaefer Test Bank PDF Full ChapterDocument36 pagesFull Download Race and Ethnicity in The United States 8th Edition Schaefer Test Bank PDF Full Chaptertortuous.osmiousr3v45i100% (23)
- PDF Advaned 1 Exam 3Document3 pagesPDF Advaned 1 Exam 3Anthony Paul Goyes QuintanillaNo ratings yet
- 07.error Detection and CorrectionDocument54 pages07.error Detection and CorrectionKaynz Skuea100% (1)
- Storification - The Next Big Content Marketing Trend and 3 Benefits Marketers Shouldn't Miss Out OnDocument3 pagesStorification - The Next Big Content Marketing Trend and 3 Benefits Marketers Shouldn't Miss Out OnKetan JhaNo ratings yet
- Business Research ReportDocument16 pagesBusiness Research Reportapi-454197312No ratings yet
- Lifestyle Upper Intermediate CB 2012 177p PDFDocument177 pagesLifestyle Upper Intermediate CB 2012 177p PDFԿորյուն ՕհանյանNo ratings yet
- Crashing Pert Networks: A Simulation ApproachDocument15 pagesCrashing Pert Networks: A Simulation ApproachRavindra BharathiNo ratings yet
- Michelangelo Research Paper OutlineDocument4 pagesMichelangelo Research Paper Outlinecampsxek100% (1)
- Pharmaceutical Document Manager in NYC Philadelphia PA Resume Christopher ReillyDocument2 pagesPharmaceutical Document Manager in NYC Philadelphia PA Resume Christopher ReillyChristopherReillyNo ratings yet
- 1044-472013 Bagrut Module F Answers To Rules of The GameDocument9 pages1044-472013 Bagrut Module F Answers To Rules of The Gamegaya friedmanNo ratings yet