Download as pptx, pdf, or txt
You might also like
- Longitudinal Section Thru "BB" Cross Section Thru "Aa": Proposed 3 Bedroom ResidentialDocument1 pageLongitudinal Section Thru "BB" Cross Section Thru "Aa": Proposed 3 Bedroom ResidentialChristian Sean PaglomutanNo ratings yet
- 913Document1 page913Brijesh ChandelNo ratings yet
- SiteDocument1 pageSitecRi SocietyNo ratings yet
- Layout Berlian ResidenceDocument1 pageLayout Berlian ResidenceDhevani Sri YulianiNo ratings yet
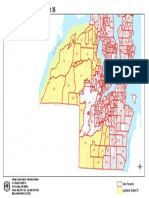
- Census Block GRP 2501-3Document1 pageCensus Block GRP 2501-3bfloblockclubsNo ratings yet
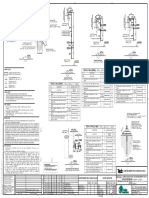
- SRE BNC V 203 0 - BkkNoiAbutDim PDFDocument1 pageSRE BNC V 203 0 - BkkNoiAbutDim PDFkeaoreNo ratings yet
- 1 PapercraftDocument21 pages1 Papercraftabraham flores bañosNo ratings yet
- SRS 222 23395 06 R5Document3 pagesSRS 222 23395 06 R5Mr. AliNo ratings yet
- Drangon Ojos AzulesDocument227 pagesDrangon Ojos AzulesElker José CamargoNo ratings yet
- Produced by An Autodesk Educational ProductDocument1 pageProduced by An Autodesk Educational ProductPAwan BasaniNo ratings yet
- 1025 K.IN Studio & HANAMORI's Office - 210525-E5Document1 page1025 K.IN Studio & HANAMORI's Office - 210525-E5KinoNo ratings yet
- 522067-A-Main Buildig - TOILET PDFDocument1 page522067-A-Main Buildig - TOILET PDFmonaliNo ratings yet
- Sass of Ono ContraltoDocument2 pagesSass of Ono ContraltofabioNo ratings yet
- Binder 1Document29 pagesBinder 1KoppahNo ratings yet
- Cash Flow PDFDocument1 pageCash Flow PDFbishu70No ratings yet
- c1 - StandardDocument1 pagec1 - StandardSibel KarasuNo ratings yet
- A Straight Pipe Details: T1 T2 T3 T4Document1 pageA Straight Pipe Details: T1 T2 T3 T4hoanghc98hn1 hoanghc98hn1No ratings yet
- Peta 10Document1 pagePeta 10Muh IchsanNo ratings yet
- DWG Add Fiberflow Pma Civil Bagian 1Document17 pagesDWG Add Fiberflow Pma Civil Bagian 1Hermon PakpahanNo ratings yet
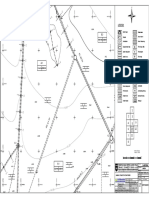
- Plano Topo SanyDocument1 pagePlano Topo SanyAlexandro TorresNo ratings yet
- Switch Floor PlanDocument1 pageSwitch Floor Plansishir mandalNo ratings yet
- Switch Floor PlanDocument1 pageSwitch Floor Plansishir mandalNo ratings yet
- Day 5 AssignmentDocument1 pageDay 5 Assignmentfilmy.photographyNo ratings yet
- 5th & 7th Floor Tower 1Document1 page5th & 7th Floor Tower 1Anthony Manalo FrondozoNo ratings yet
- Medeja KatalogDocument4 pagesMedeja KatalogJohanNo ratings yet
- DighiDocument1 pageDighiPradip MahajanNo ratings yet
- Service Kitchen Quartz Drawings-06-03-2024Document1 pageService Kitchen Quartz Drawings-06-03-2024Husen GhoriNo ratings yet
- Eep 000097 0102148005 3 ST Det 0684 R02Document1 pageEep 000097 0102148005 3 ST Det 0684 R02Vikram DalalNo ratings yet
- 02 Etage 1 GeneralDocument1 page02 Etage 1 GeneralAEMa CCCNo ratings yet
- 8013-TSA-016-DW-1462-M-510 Rev.235Document1 page8013-TSA-016-DW-1462-M-510 Rev.235raulNo ratings yet
- 3 Logshit Dayli DCS 2 Juni 2021 New.Document4 pages3 Logshit Dayli DCS 2 Juni 2021 New.Andhy AlfharoNo ratings yet
- GENERAL 04 TO LEVEL 07-Seting Out-ModelDocument1 pageGENERAL 04 TO LEVEL 07-Seting Out-ModelChamux skalNo ratings yet
- Effect of PHDocument1 pageEffect of PHSushil PantNo ratings yet
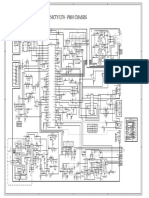
- Polar 54ctv3270 ph03 Chassis - Tda9361-Ea1, Ka5q0765rt, La SCH PDFDocument1 pagePolar 54ctv3270 ph03 Chassis - Tda9361-Ea1, Ka5q0765rt, La SCH PDFJULIONo ratings yet
- 22-AR - FINAL - BALANGO RESIDENCE-ModelDocument1 page22-AR - FINAL - BALANGO RESIDENCE-ModelJaspergroup 15No ratings yet
- I-A1-0150-Ground Floor General LayoutDocument1 pageI-A1-0150-Ground Floor General Layoutlinga2014No ratings yet
- Bucatarie Model Aplasarea CoalaDocument1 pageBucatarie Model Aplasarea CoalaGiulieta RaileanNo ratings yet
- Cdoo 01 95 23012 0001 A H03 - Hoja - de - Util PDFDocument1 pageCdoo 01 95 23012 0001 A H03 - Hoja - de - Util PDFsgtNo ratings yet
- Gerunung ProjectDocument7 pagesGerunung ProjectAlbi LuthfianNo ratings yet
- 35th LegDocument1 page35th LegmhazaniNo ratings yet
- 3G29 Rev01Document1 page3G29 Rev01Mahmoud TahaNo ratings yet
- DP13 Tge SHD RM3 303 THM 00 6001 00Document1 pageDP13 Tge SHD RM3 303 THM 00 6001 00noorgggggNo ratings yet
- Proposed New Borehole LocationDocument2 pagesProposed New Borehole LocationMuhammad NurhakeemNo ratings yet
- P Ple Als 220 30004 0Document1 pageP Ple Als 220 30004 0BadiNo ratings yet
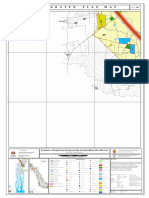
- IntegratedPlan - (1-3960) - B11Document1 pageIntegratedPlan - (1-3960) - B11SK Adnan IslamNo ratings yet
- Planos para Un Adicional de ObraDocument1 pagePlanos para Un Adicional de ObraGiomara LazoNo ratings yet
- HelmetDocument22 pagesHelmetScott RatliffNo ratings yet
- Vivan Los NoviosDocument1 pageVivan Los NoviosRaul PintoNo ratings yet
- PL AZ A: CR El PorvenirDocument1 pagePL AZ A: CR El PorvenirBODEGA CONSTRUGAS GONZALEZ GC SASNo ratings yet
- Executive Suite 1: W 2 W 1 D 3 W 2 W 3 W 1 W 1 D 4 D 3Document1 pageExecutive Suite 1: W 2 W 1 D 3 W 2 W 3 W 1 W 1 D 4 D 3Adrian PachecoNo ratings yet
- Intention B21 20200709 Clarinet 2Document1 pageIntention B21 20200709 Clarinet 2JasinNo ratings yet
- TELEPHONE1 Layout ApproedDocument1 pageTELEPHONE1 Layout Approedzafrikhan875No ratings yet
- Sheet - 10 - Ground Floor-Foundation LayoutDocument1 pageSheet - 10 - Ground Floor-Foundation LayoutNsikak EffiongNo ratings yet
- Projeto Luminotécnico e GessoDocument1 pageProjeto Luminotécnico e GessoEdilson do ValleNo ratings yet
- 4 Dennis Plano Planta y Perfil Km-tramo 04Document1 page4 Dennis Plano Planta y Perfil Km-tramo 04shunmydiaNo ratings yet
- Ejercicios RítmicosDocument2 pagesEjercicios RítmicosandreaNo ratings yet
- Pet Hu Chetty PetDocument1 pagePet Hu Chetty Petkalpanapugazh2No ratings yet
- House 12 DocumentationDocument1 pageHouse 12 DocumentationEva MaharjanNo ratings yet
- General SurgeryDocument6 pagesGeneral Surgerysdutta24680No ratings yet
- WebsiteReport JAN 2022Document224 pagesWebsiteReport JAN 2022sdutta24680No ratings yet
- Gown and Food PacketDocument13 pagesGown and Food Packetsdutta24680No ratings yet
- Flat CalcDocument2 pagesFlat Calcsdutta24680No ratings yet
- Surgery SR Rank ListDocument6 pagesSurgery SR Rank Listsdutta24680No ratings yet
- Final Registration ListDocument12 pagesFinal Registration Listsdutta24680No ratings yet
- FishboneDocument1 pageFishboneSheila Marie PanulayaNo ratings yet
- Malabon National High School: My Thoughts On COVID-19Document5 pagesMalabon National High School: My Thoughts On COVID-19Marry Jane SiosonNo ratings yet
- No VaccinationDocument2 pagesNo VaccinationChi BasNo ratings yet
- VaksinDocument1 pageVaksinnaimhasrulnaimNo ratings yet
- Certificate For COVID-19 Vaccination: Beneficiary DetailsDocument1 pageCertificate For COVID-19 Vaccination: Beneficiary DetailsPrabhat KumarNo ratings yet
- 01 2021 Eo Organizing-BhertDocument3 pages01 2021 Eo Organizing-BhertMalic PusdanNo ratings yet
- TEDET65 Math G6Document6 pagesTEDET65 Math G6AnuphaNo ratings yet
- Certification: Republic of The PhilippinesDocument2 pagesCertification: Republic of The PhilippinesBalugsNo ratings yet
- Jhang HistoryDocument16 pagesJhang HistoryAwais AnwarNo ratings yet
- Certificate - 2022-12-23T121112.931Document1 pageCertificate - 2022-12-23T121112.931Hasan JamalNo ratings yet
- Health Pass SertifikaDocument2 pagesHealth Pass SertifikaBenay SahinNo ratings yet
- Janab Sayda Bibi KahaniDocument1 pageJanab Sayda Bibi KahaniZAHID SAIFINo ratings yet
- Mauritius All-in-One Travel Digital FormDocument1 pageMauritius All-in-One Travel Digital FormJerry Danielas100% (1)
- Coronavirus Update (Live) : 1,080,846 Cases and 58,120 Deaths From COVID-19 Virus Outbreak - WorldometerDocument20 pagesCoronavirus Update (Live) : 1,080,846 Cases and 58,120 Deaths From COVID-19 Virus Outbreak - Worldometernilton lialungaNo ratings yet
- Vaccination Certificate Patrick MorganDocument1 pageVaccination Certificate Patrick Morganantoinne.jburton0827No ratings yet
- Health Pass SertifikaDocument2 pagesHealth Pass SertifikaburcingulecNo ratings yet
- Covid 19Document4 pagesCovid 19Jayve BasconNo ratings yet
- Verify - Gov.sg 2Document4 pagesVerify - Gov.sg 2Tha OoNo ratings yet
- F2F PlanDocument3 pagesF2F Planismael delosreyesNo ratings yet
- International COVID-19 Vaccination Certificate: Yamuta, Ruth Padilla 1963-12-24 F PA1034999Document1 pageInternational COVID-19 Vaccination Certificate: Yamuta, Ruth Padilla 1963-12-24 F PA1034999Ruth Polimar YamutaNo ratings yet
- SohailDocument1 pageSohailfamliyli670No ratings yet
- The Boons and Banes of Academic Freeze in Time of PandemicDocument2 pagesThe Boons and Banes of Academic Freeze in Time of PandemicChretien Aeza JovenNo ratings yet
- CertificateDocument1 pageCertificateZainab KhanNo ratings yet
- Re-Deployment Requirements Series 4-06032020Document1 pageRe-Deployment Requirements Series 4-06032020Clarabelle Mae Dela RosaNo ratings yet
- Lampiran 7 Borang Pengisytiharan KesihatanDocument2 pagesLampiran 7 Borang Pengisytiharan KesihatanGorin GorinNo ratings yet
- History 4Document2 pagesHistory 4mohammed hamzaNo ratings yet
- Coronavirus (COVID-19) RecordsDocument3 pagesCoronavirus (COVID-19) RecordsMarioNo ratings yet
- G 12 STEM HRPTA Minutes of The MeetingDocument3 pagesG 12 STEM HRPTA Minutes of The MeetingAlvin Ray GarciaNo ratings yet
- Certificate of Consent - ADocument1 pageCertificate of Consent - Aren whahahhaNo ratings yet
- CG Covid Risk Assessment - Hirers - Nov 2021Document8 pagesCG Covid Risk Assessment - Hirers - Nov 2021hibaNo ratings yet