
Dyslipidemia CPG 2020 Review
Dyslipidemia CPG 2020 Review
You might also like
- The Ischemic ElectrocardiogramDocument16 pagesThe Ischemic ElectrocardiogramAdiel OjedaNo ratings yet
- Renal FailureDocument48 pagesRenal FailureCindy MamalangkasNo ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- DyslipidemiaDocument50 pagesDyslipidemialailahNo ratings yet
- (CPG) 2020 Clinical Practice Guidelines For The Management of Dyslipidemia in The PhilippinesDocument131 pages(CPG) 2020 Clinical Practice Guidelines For The Management of Dyslipidemia in The PhilippinesKai Chua0% (1)
- HIPERLIPIDEMIADocument10 pagesHIPERLIPIDEMIAMarianaNo ratings yet
- Metabolic DR - RehabDocument24 pagesMetabolic DR - RehabMohammed Saad NabhanNo ratings yet
- ATP IV HandoutDocument2 pagesATP IV Handouthafidzz1No ratings yet
- CPG DyslipidemiaDocument26 pagesCPG DyslipidemiaRenzy SalumbreNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Diabetes Mellitus: Geriatrics Evaluation & ManagementDocument4 pagesDiabetes Mellitus: Geriatrics Evaluation & ManagementAngeles SlzrNo ratings yet
- Atherosclerotic Cardiovascular Disease (ASCVD) Secondary Prevention GuidelineDocument19 pagesAtherosclerotic Cardiovascular Disease (ASCVD) Secondary Prevention GuidelinearieftomNo ratings yet
- RX For Selected PtsDocument22 pagesRX For Selected PtsBubu ToNo ratings yet
- Executive Summary of 2020 CPG For Dyslipidemia Management in The PhilippinesDocument3 pagesExecutive Summary of 2020 CPG For Dyslipidemia Management in The PhilippinesBrooke PabsNo ratings yet
- 2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3Document15 pages2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3CoolrobertizNo ratings yet
- Screening and Management of Lipids: Patient Population: ObjectiveDocument20 pagesScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyNo ratings yet
- LipidsupdateDocument23 pagesLipidsupdatedrshekarforyouNo ratings yet
- A Pragmatic View of The New Cholesterol Treatment GuidelinesDocument4 pagesA Pragmatic View of The New Cholesterol Treatment GuidelinesMaria Fernanda CoralNo ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Reviews: Statins in The Primary Prevention of Cardiovascular DiseaseDocument12 pagesReviews: Statins in The Primary Prevention of Cardiovascular DiseaseCrischentian BrinzaNo ratings yet
- Berkas 2 - 1Document60 pagesBerkas 2 - 1Green GeeksNo ratings yet
- PH Errata V1Document18 pagesPH Errata V1kelvinNo ratings yet
- Coronary Artery Disease (CAD) - DynaMedexDocument116 pagesCoronary Artery Disease (CAD) - DynaMedexIribuka JonathanNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Dyslipidemia in Diabetes Mellitus and Cardiovascular DiseaseDocument6 pagesDyslipidemia in Diabetes Mellitus and Cardiovascular DiseaseEward Rod SalNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- 2013 Acc Aha Guideline On The Treatment of Blood Cholesterol To Reduce Athersclerotic Risk 2Document67 pages2013 Acc Aha Guideline On The Treatment of Blood Cholesterol To Reduce Athersclerotic Risk 2HidayadNo ratings yet
- Prevenção Secundária AafpDocument9 pagesPrevenção Secundária AafpCamila Gomes Santos MoraesNo ratings yet
- Ongoing Therapy and MonitoringDocument1 pageOngoing Therapy and MonitoringDaveMartoneNo ratings yet
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- Management of DyslipidemiaDocument35 pagesManagement of DyslipidemiaAmir MahmoudNo ratings yet
- Ascvd PrimaryDocument21 pagesAscvd Primaryprk prkNo ratings yet
- Atherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineDocument21 pagesAtherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineHeryanti PusparisaNo ratings yet
- Diabetes Manejo DislipidemiaDocument8 pagesDiabetes Manejo DislipidemiaLuis C Ribon VNo ratings yet
- Pastori - The Efficacy - 2015Document8 pagesPastori - The Efficacy - 2015Mong mong Bam bamNo ratings yet
- Diabetes & AgingDocument2 pagesDiabetes & AgingAnn DahngNo ratings yet
- Ham's Primary Care Geriatrics 6E 2014Document2 pagesHam's Primary Care Geriatrics 6E 2014AhmedNo ratings yet
- Quality Tip - ADA Guideline Updates - 2010: Diagnosis of DiabetesDocument7 pagesQuality Tip - ADA Guideline Updates - 2010: Diagnosis of Diabetesyunitaekawati1459No ratings yet
- Ischemic Heart Diease PDFDocument33 pagesIschemic Heart Diease PDFMahamed Wefkey OmranNo ratings yet
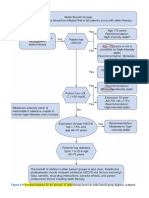
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Essential Messages - 2023 DiabetesDocument13 pagesEssential Messages - 2023 Diabetesimran karimNo ratings yet
- Dyslipidemia 2018Document8 pagesDyslipidemia 2018R JannahNo ratings yet
- Lipids JBDocument48 pagesLipids JBMuvenn KannanNo ratings yet
- Stable Coronary Artery DiseaseDocument7 pagesStable Coronary Artery DiseaseFreddy PanjaitanNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- 2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskDocument9 pages2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskGandri Ali Ma'suNo ratings yet
- Diretriz - Dislipidemia EndocrinologiaDocument70 pagesDiretriz - Dislipidemia EndocrinologiaSamara QueirozNo ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- CCRR 1 114 PDFDocument3 pagesCCRR 1 114 PDFBruno Mario AngelNo ratings yet
- Applicability of Recent Dyslipidemia Guidelines in Clinical PracticeDocument4 pagesApplicability of Recent Dyslipidemia Guidelines in Clinical PracticeDokter FebyanNo ratings yet
- 2020 Lipid Management in Patients With Endocrine Disorder An Endocrine Society Clinical PracticeDocument70 pages2020 Lipid Management in Patients With Endocrine Disorder An Endocrine Society Clinical PracticeViệt Cường TạNo ratings yet
- Pharma Cardio1Document28 pagesPharma Cardio1Star DustNo ratings yet
- 2nd Case Session ToT CPG HPTDocument127 pages2nd Case Session ToT CPG HPThakimahsNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- PAD Handout 4thDocument27 pagesPAD Handout 4thdawitNo ratings yet
- Dyslipedemia ShortDocument5 pagesDyslipedemia Shortذوالفقار أحمدNo ratings yet
- Jaha 116 004909 PDFDocument8 pagesJaha 116 004909 PDFLisbeth MarbunNo ratings yet
- Digitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008Document18 pagesDigitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008LenyNo ratings yet
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratNo ratings yet
- Perfusion Review - Nclex TipsDocument37 pagesPerfusion Review - Nclex TipsMichael S. PetryNo ratings yet
- A Study To Assess The Prevalence of TattDocument5 pagesA Study To Assess The Prevalence of Tatt高權梁No ratings yet
- International 2Document4 pagesInternational 2daffunkmadansyahNo ratings yet
- Health Module 3Document11 pagesHealth Module 3Mark Anthony MaquilingNo ratings yet
- Anjali Singh 9B HHWDocument10 pagesAnjali Singh 9B HHWsuhani singhNo ratings yet
- Akayesu - Rape Definition Only International LawDocument2 pagesAkayesu - Rape Definition Only International LawMaria Guila Renee BaldonadoNo ratings yet
- 3Document4 pages3Heeta PanchasaraNo ratings yet
- Asd Vs AdhdDocument3 pagesAsd Vs AdhdSudhakar PrasannaNo ratings yet
- Neurocritical Care in The General Intensive Care UnitDocument17 pagesNeurocritical Care in The General Intensive Care UnitdanielNo ratings yet
- Rijckborst, VincentDocument155 pagesRijckborst, VincentafifahayestinapelinggaNo ratings yet
- LCRN NIHR Local CRN Contacts MASTER - Updated 15 Aug 2014Document17 pagesLCRN NIHR Local CRN Contacts MASTER - Updated 15 Aug 2014Naga MuthuNo ratings yet
- 26.12 PEDIATRICS Childhood ImmunizationDocument5 pages26.12 PEDIATRICS Childhood ImmunizationLA BriguelaNo ratings yet
- f2 Home-Sci Simplified Notes SPDocument20 pagesf2 Home-Sci Simplified Notes SPmicah isabokeNo ratings yet
- Preeclampsia 2022Document16 pagesPreeclampsia 2022MedhumanNo ratings yet
- Breast Cancer PPT 1Document127 pagesBreast Cancer PPT 1ATEHAN BORDSNo ratings yet
- SB5-Questions 2Document5 pagesSB5-Questions 2hg eagleNo ratings yet
- Sas 26Document2 pagesSas 26Leaflor Ann ManghihilotNo ratings yet
- Chronic Renal Failure: Nursing GoalDocument3 pagesChronic Renal Failure: Nursing Goal006 shinta aprilia Ananda risnantoNo ratings yet
- CHApter 57Document18 pagesCHApter 572071317No ratings yet
- Kode ICD10Document27 pagesKode ICD10inaiNo ratings yet
- Best Practice & Research Clinical Anaesthesiology: SciencedirectDocument11 pagesBest Practice & Research Clinical Anaesthesiology: Sciencedirectrogelio cruzNo ratings yet
- BIRADSDocument32 pagesBIRADSMartin AmoresNo ratings yet
- 1 s2.0 S2468124523000086 MainDocument16 pages1 s2.0 S2468124523000086 MainDana MuraneviciNo ratings yet
- Thesis Report On: "Unveiling Chemical and Pharmacological Studies To Provide New Insights On Hibiscus MacrophyllusDocument149 pagesThesis Report On: "Unveiling Chemical and Pharmacological Studies To Provide New Insights On Hibiscus MacrophyllusShazedul Islam SajidNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument40 pagesChronic Obstructive Pulmonary DiseaseIVORY DIANE AMANCIONo ratings yet
- Knowledge, Risk Factors and Perceived Attitude TowardsDocument12 pagesKnowledge, Risk Factors and Perceived Attitude TowardsMatilda OtooNo ratings yet
- Pediatrics Community Acquired Pneumonia Case StudyDocument75 pagesPediatrics Community Acquired Pneumonia Case StudyAJAY MANDALNo ratings yet
- Spinal TuberculosisDocument54 pagesSpinal TuberculosisGagandeep YadavNo ratings yet
























































































Download as pptx, pdf, or txt
You might also like
- The Ischemic ElectrocardiogramDocument16 pagesThe Ischemic ElectrocardiogramAdiel OjedaNo ratings yet
- Renal FailureDocument48 pagesRenal FailureCindy MamalangkasNo ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- PSAP 2019 Dyslipidemia PDFDocument24 pagesPSAP 2019 Dyslipidemia PDFdellykets_323822919No ratings yet
- DyslipidemiaDocument50 pagesDyslipidemialailahNo ratings yet
- (CPG) 2020 Clinical Practice Guidelines For The Management of Dyslipidemia in The PhilippinesDocument131 pages(CPG) 2020 Clinical Practice Guidelines For The Management of Dyslipidemia in The PhilippinesKai Chua0% (1)
- HIPERLIPIDEMIADocument10 pagesHIPERLIPIDEMIAMarianaNo ratings yet
- Metabolic DR - RehabDocument24 pagesMetabolic DR - RehabMohammed Saad NabhanNo ratings yet
- ATP IV HandoutDocument2 pagesATP IV Handouthafidzz1No ratings yet
- CPG DyslipidemiaDocument26 pagesCPG DyslipidemiaRenzy SalumbreNo ratings yet
- Li 2017Document32 pagesLi 2017akshayNo ratings yet
- Diabetes Mellitus: Geriatrics Evaluation & ManagementDocument4 pagesDiabetes Mellitus: Geriatrics Evaluation & ManagementAngeles SlzrNo ratings yet
- Atherosclerotic Cardiovascular Disease (ASCVD) Secondary Prevention GuidelineDocument19 pagesAtherosclerotic Cardiovascular Disease (ASCVD) Secondary Prevention GuidelinearieftomNo ratings yet
- RX For Selected PtsDocument22 pagesRX For Selected PtsBubu ToNo ratings yet
- Executive Summary of 2020 CPG For Dyslipidemia Management in The PhilippinesDocument3 pagesExecutive Summary of 2020 CPG For Dyslipidemia Management in The PhilippinesBrooke PabsNo ratings yet
- 2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3Document15 pages2013 Cholesterol Guidelines at A Glance: - Robert Barnes, M3CoolrobertizNo ratings yet
- Screening and Management of Lipids: Patient Population: ObjectiveDocument20 pagesScreening and Management of Lipids: Patient Population: ObjectiveKatie Kroll BradyNo ratings yet
- LipidsupdateDocument23 pagesLipidsupdatedrshekarforyouNo ratings yet
- A Pragmatic View of The New Cholesterol Treatment GuidelinesDocument4 pagesA Pragmatic View of The New Cholesterol Treatment GuidelinesMaria Fernanda CoralNo ratings yet
- 2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"Document51 pages2013 ACC/AHA Blood Cholesterol Treatment Guidelines: "Intensity of Statin Therapy"dr_yasserNo ratings yet
- Reviews: Statins in The Primary Prevention of Cardiovascular DiseaseDocument12 pagesReviews: Statins in The Primary Prevention of Cardiovascular DiseaseCrischentian BrinzaNo ratings yet
- Berkas 2 - 1Document60 pagesBerkas 2 - 1Green GeeksNo ratings yet
- PH Errata V1Document18 pagesPH Errata V1kelvinNo ratings yet
- Coronary Artery Disease (CAD) - DynaMedexDocument116 pagesCoronary Artery Disease (CAD) - DynaMedexIribuka JonathanNo ratings yet
- 2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsDocument37 pages2013 ACC/AHA Guideline On The Treatment of Blood Cholesterol To Reduce Atherosclerotic Cardiovascular Risk in AdultsIman SaksoukNo ratings yet
- Dyslipidemia in Diabetes Mellitus and Cardiovascular DiseaseDocument6 pagesDyslipidemia in Diabetes Mellitus and Cardiovascular DiseaseEward Rod SalNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- 2013 Acc Aha Guideline On The Treatment of Blood Cholesterol To Reduce Athersclerotic Risk 2Document67 pages2013 Acc Aha Guideline On The Treatment of Blood Cholesterol To Reduce Athersclerotic Risk 2HidayadNo ratings yet
- Prevenção Secundária AafpDocument9 pagesPrevenção Secundária AafpCamila Gomes Santos MoraesNo ratings yet
- Ongoing Therapy and MonitoringDocument1 pageOngoing Therapy and MonitoringDaveMartoneNo ratings yet
- Clinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Document61 pagesClinical Pharmacy Department Clinical Pharmacy and Drug Information PL 504Bassant Ahmed Mahmoud Ragab Abdallah AyaadNo ratings yet
- Management of DyslipidemiaDocument35 pagesManagement of DyslipidemiaAmir MahmoudNo ratings yet
- Ascvd PrimaryDocument21 pagesAscvd Primaryprk prkNo ratings yet
- Atherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineDocument21 pagesAtherosclerotic Cardiovascular Disease (ASCVD) Primary Prevention GuidelineHeryanti PusparisaNo ratings yet
- Diabetes Manejo DislipidemiaDocument8 pagesDiabetes Manejo DislipidemiaLuis C Ribon VNo ratings yet
- Pastori - The Efficacy - 2015Document8 pagesPastori - The Efficacy - 2015Mong mong Bam bamNo ratings yet
- Diabetes & AgingDocument2 pagesDiabetes & AgingAnn DahngNo ratings yet
- Ham's Primary Care Geriatrics 6E 2014Document2 pagesHam's Primary Care Geriatrics 6E 2014AhmedNo ratings yet
- Quality Tip - ADA Guideline Updates - 2010: Diagnosis of DiabetesDocument7 pagesQuality Tip - ADA Guideline Updates - 2010: Diagnosis of Diabetesyunitaekawati1459No ratings yet
- Ischemic Heart Diease PDFDocument33 pagesIschemic Heart Diease PDFMahamed Wefkey OmranNo ratings yet
- Recommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (AdaptedDocument8 pagesRecommendations For The Intensity of Statin Therapy Based On Statin Benefit Group Diagram. (Adaptedعزالدين الطيارNo ratings yet
- Essential Messages - 2023 DiabetesDocument13 pagesEssential Messages - 2023 Diabetesimran karimNo ratings yet
- Dyslipidemia 2018Document8 pagesDyslipidemia 2018R JannahNo ratings yet
- Lipids JBDocument48 pagesLipids JBMuvenn KannanNo ratings yet
- Stable Coronary Artery DiseaseDocument7 pagesStable Coronary Artery DiseaseFreddy PanjaitanNo ratings yet
- Management of Blood Cholesterol 2019Document2 pagesManagement of Blood Cholesterol 2019Luis Alberto Alvarez AnkassNo ratings yet
- 2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskDocument9 pages2013 ACC or AHA Cholesterol Treatment Guideline Paradigm Shifts in Managing Atherosclerotic Cardiovascular Disease RiskGandri Ali Ma'suNo ratings yet
- Diretriz - Dislipidemia EndocrinologiaDocument70 pagesDiretriz - Dislipidemia EndocrinologiaSamara QueirozNo ratings yet
- Preventing Cardiovascular Disease in Patients With.2 PDFDocument3 pagesPreventing Cardiovascular Disease in Patients With.2 PDFbacharelado2010No ratings yet
- CCRR 1 114 PDFDocument3 pagesCCRR 1 114 PDFBruno Mario AngelNo ratings yet
- Applicability of Recent Dyslipidemia Guidelines in Clinical PracticeDocument4 pagesApplicability of Recent Dyslipidemia Guidelines in Clinical PracticeDokter FebyanNo ratings yet
- 2020 Lipid Management in Patients With Endocrine Disorder An Endocrine Society Clinical PracticeDocument70 pages2020 Lipid Management in Patients With Endocrine Disorder An Endocrine Society Clinical PracticeViệt Cường TạNo ratings yet
- Pharma Cardio1Document28 pagesPharma Cardio1Star DustNo ratings yet
- 2nd Case Session ToT CPG HPTDocument127 pages2nd Case Session ToT CPG HPThakimahsNo ratings yet
- Lower Is Better - FinalDocument91 pagesLower Is Better - FinalJamsidul Hassan RajibNo ratings yet
- PAD Handout 4thDocument27 pagesPAD Handout 4thdawitNo ratings yet
- Dyslipedemia ShortDocument5 pagesDyslipedemia Shortذوالفقار أحمدNo ratings yet
- Jaha 116 004909 PDFDocument8 pagesJaha 116 004909 PDFLisbeth MarbunNo ratings yet
- Digitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008Document18 pagesDigitekâ® (Digoxin Tablets, Usp) Recalled (Actavis Totowa LLC) - April 28, 2008LenyNo ratings yet
- Dyslipidaemia 2019Document61 pagesDyslipidaemia 2019fatima.shqeratNo ratings yet
- Perfusion Review - Nclex TipsDocument37 pagesPerfusion Review - Nclex TipsMichael S. PetryNo ratings yet
- A Study To Assess The Prevalence of TattDocument5 pagesA Study To Assess The Prevalence of Tatt高權梁No ratings yet
- International 2Document4 pagesInternational 2daffunkmadansyahNo ratings yet
- Health Module 3Document11 pagesHealth Module 3Mark Anthony MaquilingNo ratings yet
- Anjali Singh 9B HHWDocument10 pagesAnjali Singh 9B HHWsuhani singhNo ratings yet
- Akayesu - Rape Definition Only International LawDocument2 pagesAkayesu - Rape Definition Only International LawMaria Guila Renee BaldonadoNo ratings yet
- 3Document4 pages3Heeta PanchasaraNo ratings yet
- Asd Vs AdhdDocument3 pagesAsd Vs AdhdSudhakar PrasannaNo ratings yet
- Neurocritical Care in The General Intensive Care UnitDocument17 pagesNeurocritical Care in The General Intensive Care UnitdanielNo ratings yet
- Rijckborst, VincentDocument155 pagesRijckborst, VincentafifahayestinapelinggaNo ratings yet
- LCRN NIHR Local CRN Contacts MASTER - Updated 15 Aug 2014Document17 pagesLCRN NIHR Local CRN Contacts MASTER - Updated 15 Aug 2014Naga MuthuNo ratings yet
- 26.12 PEDIATRICS Childhood ImmunizationDocument5 pages26.12 PEDIATRICS Childhood ImmunizationLA BriguelaNo ratings yet
- f2 Home-Sci Simplified Notes SPDocument20 pagesf2 Home-Sci Simplified Notes SPmicah isabokeNo ratings yet
- Preeclampsia 2022Document16 pagesPreeclampsia 2022MedhumanNo ratings yet
- Breast Cancer PPT 1Document127 pagesBreast Cancer PPT 1ATEHAN BORDSNo ratings yet
- SB5-Questions 2Document5 pagesSB5-Questions 2hg eagleNo ratings yet
- Sas 26Document2 pagesSas 26Leaflor Ann ManghihilotNo ratings yet
- Chronic Renal Failure: Nursing GoalDocument3 pagesChronic Renal Failure: Nursing Goal006 shinta aprilia Ananda risnantoNo ratings yet
- CHApter 57Document18 pagesCHApter 572071317No ratings yet
- Kode ICD10Document27 pagesKode ICD10inaiNo ratings yet
- Best Practice & Research Clinical Anaesthesiology: SciencedirectDocument11 pagesBest Practice & Research Clinical Anaesthesiology: Sciencedirectrogelio cruzNo ratings yet
- BIRADSDocument32 pagesBIRADSMartin AmoresNo ratings yet
- 1 s2.0 S2468124523000086 MainDocument16 pages1 s2.0 S2468124523000086 MainDana MuraneviciNo ratings yet
- Thesis Report On: "Unveiling Chemical and Pharmacological Studies To Provide New Insights On Hibiscus MacrophyllusDocument149 pagesThesis Report On: "Unveiling Chemical and Pharmacological Studies To Provide New Insights On Hibiscus MacrophyllusShazedul Islam SajidNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument40 pagesChronic Obstructive Pulmonary DiseaseIVORY DIANE AMANCIONo ratings yet
- Knowledge, Risk Factors and Perceived Attitude TowardsDocument12 pagesKnowledge, Risk Factors and Perceived Attitude TowardsMatilda OtooNo ratings yet
- Pediatrics Community Acquired Pneumonia Case StudyDocument75 pagesPediatrics Community Acquired Pneumonia Case StudyAJAY MANDALNo ratings yet
- Spinal TuberculosisDocument54 pagesSpinal TuberculosisGagandeep YadavNo ratings yet