
Diabetic Retinopathy
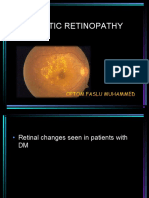
Diabetic Retinopathy
You might also like
- Biology Worksheet Sheep Heart DissectionDocument3 pagesBiology Worksheet Sheep Heart DissectionFluphie Bunny0% (1)
- Nclex MemorizeDocument7 pagesNclex MemorizeRoger Jones Jr.81% (16)
- Diabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeDocument63 pagesDiabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeNear DeathNo ratings yet
- Diabetic Retinopathy: Dwi Lestari PohanDocument72 pagesDiabetic Retinopathy: Dwi Lestari PohanKelvin MandelaNo ratings yet
- DIabetic REtinopathyDocument34 pagesDIabetic REtinopathyLuqman Khan YousafXaiNo ratings yet
- Diabetic-Retinopathy GGGHGHDocument50 pagesDiabetic-Retinopathy GGGHGHjegannancyNo ratings yet
- Diabetic RetinopathyDocument40 pagesDiabetic RetinopathyNaman MishraNo ratings yet
- Diabetic RetinopathyDocument67 pagesDiabetic RetinopathyFirstyIlminovia0% (1)
- Diabetic ThyDocument36 pagesDiabetic ThyItaNo ratings yet
- Diabetic RetinopathyDocument48 pagesDiabetic Retinopathykaran.A.K100% (1)
- AiraDocument17 pagesAiraPrincess Aira Bucag CarbonelNo ratings yet
- DR and Its ManagementDocument76 pagesDR and Its ManagementAravind KumarNo ratings yet
- Retinal Vascular Diseas E: Christine Anne D. EspejaDocument25 pagesRetinal Vascular Diseas E: Christine Anne D. EspejaPaolo QuezonNo ratings yet
- Diabetic Retinopathy: Johnson Marystella Rahul Imd 14 2 A Roll No 34Document17 pagesDiabetic Retinopathy: Johnson Marystella Rahul Imd 14 2 A Roll No 34J.m.RahulNo ratings yet
- Diabetic Retinopathy New-1Document99 pagesDiabetic Retinopathy New-1Sana AzimNo ratings yet
- Diabetic RetinopathyDocument101 pagesDiabetic RetinopathyMohiuddin AhmedNo ratings yet
- Diabetic RetinopatiDocument44 pagesDiabetic RetinopatiLaurensia MassariNo ratings yet
- Diabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Document41 pagesDiabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Baba YagaNo ratings yet
- Lecture 11 Retina 1Document44 pagesLecture 11 Retina 1ؤيؤييسيNo ratings yet
- A Deep Learning Approach For The Detection of Diabetic RetinopathyDocument55 pagesA Deep Learning Approach For The Detection of Diabetic RetinopathyjegannancyNo ratings yet
- Diabetic RetinopathyDocument44 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Diabetic RetinopathyDocument73 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Diabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerDocument32 pagesDiabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerCarlos HerreraNo ratings yet
- Diabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Document40 pagesDiabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Franky Frans SihombingNo ratings yet
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyDrSaid Hussein GediNo ratings yet
- Diabetic With The EyeDocument50 pagesDiabetic With The EyeJianhua ShiNo ratings yet
- Diabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaDocument13 pagesDiabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaMohamad Faizul Abu HanifaNo ratings yet
- Retinopatia Diabetica 2018Document34 pagesRetinopatia Diabetica 2018Fanny ParraNo ratings yet
- Ico Guidelines For Diabetic Eye CareDocument19 pagesIco Guidelines For Diabetic Eye CareMuhammad Usman Salim100% (1)
- Diabetic RetinopathyDocument78 pagesDiabetic RetinopathyAnumeha Jindal100% (1)
- RetinopathyDocument64 pagesRetinopathySiti NcitNo ratings yet
- Diabetic Retinopathy Presentations (Can Still Use The Older Classification)Document6 pagesDiabetic Retinopathy Presentations (Can Still Use The Older Classification)gdudex118811No ratings yet
- Diabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDDocument55 pagesDiabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDadi amaliNo ratings yet
- Diabetic Eye Disease: Academic Unit of OphthalmologyDocument35 pagesDiabetic Eye Disease: Academic Unit of Ophthalmologyruwan555No ratings yet
- Diabetic RetinopathyDocument43 pagesDiabetic RetinopathyBrampp HimawanNo ratings yet
- Simpo 13.3 - DR Rova - How To Avoid Blindness in Diabetic Eye Disease - PIT IDI Jabar 2018Document51 pagesSimpo 13.3 - DR Rova - How To Avoid Blindness in Diabetic Eye Disease - PIT IDI Jabar 2018Nadar RizatullahNo ratings yet
- Refrat Retinopati-DiabetikDocument20 pagesRefrat Retinopati-DiabetikDea NabilaNo ratings yet
- Retinal Disorders Med VDocument66 pagesRetinal Disorders Med Vhenok birukNo ratings yet
- Kuliah Retina by Widi 2Document57 pagesKuliah Retina by Widi 2DERYGP96 GENIUSNo ratings yet
- Vascular Disorders of RetinaDocument46 pagesVascular Disorders of RetinaSubash BasnetNo ratings yet
- Kuliah VitreoretinaDocument30 pagesKuliah VitreoretinaMoch. NabilNo ratings yet
- RetinaDocument82 pagesRetinafebienaNo ratings yet
- Nonproliferative Diabetic Retinopathy and Diabetic Macular EdemaDocument37 pagesNonproliferative Diabetic Retinopathy and Diabetic Macular EdemaBhumika RathNo ratings yet
- Vitreo Retinal DisordersDocument47 pagesVitreo Retinal DisordersTabreez KhanNo ratings yet
- مح١٨Document44 pagesمح١٨جهاد إبراهيمNo ratings yet
- Diabetic Retinopathy DR KatariaDocument65 pagesDiabetic Retinopathy DR KatariaDr Sandeep Kataria100% (1)
- BCS 5.02 - Organ Pathology in Diabetes - DR Saeed Alshieban 2022Document39 pagesBCS 5.02 - Organ Pathology in Diabetes - DR Saeed Alshieban 2022MATHS By AbdulrahmanNo ratings yet
- ICOGuidelins For DiabeticEye CareDocument28 pagesICOGuidelins For DiabeticEye CareIrfan SadiqNo ratings yet
- DM ComplicationsDocument97 pagesDM ComplicationsElena Borş MorariNo ratings yet
- Vitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkiDocument45 pagesVitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkitusuksedotanNo ratings yet
- Retinal Diseases (Notes)Document76 pagesRetinal Diseases (Notes)khloud ywsefNo ratings yet
- Diabetes Mellitus ComplicationsDocument64 pagesDiabetes Mellitus ComplicationsAdria Putra FarhandikaNo ratings yet
- Acute Painless Loss of Vision: DR S P Mukherjee Ophthalmology, KPCMCHDocument17 pagesAcute Painless Loss of Vision: DR S P Mukherjee Ophthalmology, KPCMCHJayanti Neogi SardarNo ratings yet
- Chronic Complications of Diabetes MellitusDocument53 pagesChronic Complications of Diabetes MellitusAli Murtaza AbbasNo ratings yet
- Retinal Vascular DisordersDocument52 pagesRetinal Vascular Disorderssushma shresthaNo ratings yet
- Modified Management of Diabetic RetinopathyDocument54 pagesModified Management of Diabetic RetinopathyAnviNo ratings yet
- Diabetes AND The Eye: Juliana Bentil Deborah AddoDocument50 pagesDiabetes AND The Eye: Juliana Bentil Deborah Addogideon A. owusuNo ratings yet
- Diabetic Retinopathy GradingDocument64 pagesDiabetic Retinopathy Gradingfadzil hamidNo ratings yet
- PSSS Mata Merah Visus Menurun PerlahanDocument44 pagesPSSS Mata Merah Visus Menurun PerlahandeyshieNo ratings yet
- Diabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDDocument56 pagesDiabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDmawar2505No ratings yet
- Retinopati Diabetik - 1Document19 pagesRetinopati Diabetik - 1Yoyada SitorusNo ratings yet
- Diabetic Retinopathy: Introduction to Novel Treatment StrategiesFrom EverandDiabetic Retinopathy: Introduction to Novel Treatment StrategiesNo ratings yet
- Viral ConjunctivitisDocument30 pagesViral ConjunctivitisDr Sravya M VNo ratings yet
- Siegel's SpeculumDocument12 pagesSiegel's SpeculumDr Sravya M VNo ratings yet
- Anatomy of EyelidsDocument25 pagesAnatomy of EyelidsDr Sravya M VNo ratings yet
- Kapala Rogas - ModernDocument23 pagesKapala Rogas - ModernDr Sravya M VNo ratings yet
- TinnitusDocument18 pagesTinnitusDr Sravya M VNo ratings yet
- Hearing LossDocument68 pagesHearing LossDr Sravya M VNo ratings yet
- Hearing EvaluationDocument151 pagesHearing EvaluationDr Sravya M VNo ratings yet
- Physiology of HearingDocument30 pagesPhysiology of HearingDr Sravya M VNo ratings yet
- Examination of EyeDocument39 pagesExamination of EyeDr Sravya M VNo ratings yet
- Risk For Decreased Cardiac Output NCPDocument2 pagesRisk For Decreased Cardiac Output NCPMae Denn LabordoNo ratings yet
- Congenital Heart DiseaseDocument37 pagesCongenital Heart Diseaseveralynnp100% (1)
- Biochem SGD 3Document4 pagesBiochem SGD 3Hemanth KokaNo ratings yet
- Full Download PDF of Medical Secrets 6th Edition Mary P. Harward - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Medical Secrets 6th Edition Mary P. Harward - Ebook PDF All Chapterphakhijayahr100% (7)
- Hematogenous Spread. Lymphatic Spread.: 275 Characteristics of Benign and Malignant NeoplasmsDocument4 pagesHematogenous Spread. Lymphatic Spread.: 275 Characteristics of Benign and Malignant NeoplasmsGin TokiNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval 25 (OH) VIT D2 ErgocalciferolDocument4 pagesLaboratory Test Report: Test Name Result Biological Reference Interval 25 (OH) VIT D2 ErgocalciferolEkta SinhaNo ratings yet
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDocument4 pagesInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaNo ratings yet
- GenogramDocument10 pagesGenogrammohamadNo ratings yet
- Internship Logbook 2020Document136 pagesInternship Logbook 2020MaleehaNo ratings yet
- DRUG STUDY: Metoprolol - BetalocDocument1 pageDRUG STUDY: Metoprolol - BetalocYum C100% (1)
- Doppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesDocument12 pagesDoppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesAbraham PaulNo ratings yet
- Pathophysiology of Respiratory System Feghiu I., Tacu L. Lutan VDocument55 pagesPathophysiology of Respiratory System Feghiu I., Tacu L. Lutan VLunguVictoriaNo ratings yet
- Hormonal TherapiesDocument39 pagesHormonal TherapiesJalal EltabibNo ratings yet
- National Emergency Nurses Association: Core CompetenciesDocument8 pagesNational Emergency Nurses Association: Core CompetenciesJordanian CopyNo ratings yet
- Peripheral Vascular Disease and DiabetesDocument8 pagesPeripheral Vascular Disease and DiabetesChikezie OnwukweNo ratings yet
- Atrial FibrillationDocument20 pagesAtrial Fibrillationjack sawdaNo ratings yet
- Cardiovascular SystemDocument15 pagesCardiovascular SystemCapper RuedaNo ratings yet
- MSN Questions 100Document16 pagesMSN Questions 100Efreignz Mangay-at KinomesNo ratings yet
- How Animals Survive (Circulation and GasDocument24 pagesHow Animals Survive (Circulation and GasJohn Ted BañezNo ratings yet
- Chapter 15 - Cardiovascular SystemDocument89 pagesChapter 15 - Cardiovascular SystemOliver Namyalo100% (1)
- CC Lec Mod 3Document13 pagesCC Lec Mod 38wgmhh9ks9No ratings yet
- Ischemic StrokeDocument8 pagesIschemic StrokeSofía Maltés GarridoNo ratings yet
- Fact Sheeton Canola OilDocument15 pagesFact Sheeton Canola OilMonika ThadeaNo ratings yet
- Cardio System 2Document1 pageCardio System 2api-298312370No ratings yet
- General Medicine Lec4 Adrenal GlandsDocument9 pagesGeneral Medicine Lec4 Adrenal GlandsAli MONo ratings yet
- Lectura Previa3-Approach To The Patient With Abnormal Vital SignsDocument7 pagesLectura Previa3-Approach To The Patient With Abnormal Vital SignsEdwin Robles NorabuenaNo ratings yet
- 7 DkaDocument28 pages7 DkaFuad Aman AbjNo ratings yet
- Transplant and Dialysis Handbook 2nd Edition January 2017Document125 pagesTransplant and Dialysis Handbook 2nd Edition January 2017nathanielNo ratings yet


































































































Download as pptx, pdf, or txt
You might also like
- Biology Worksheet Sheep Heart DissectionDocument3 pagesBiology Worksheet Sheep Heart DissectionFluphie Bunny0% (1)
- Nclex MemorizeDocument7 pagesNclex MemorizeRoger Jones Jr.81% (16)
- Diabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeDocument63 pagesDiabetic Retinopathy: PRESENTED BY: Dr. Kawshik Nag MS Resident Phase A (Ophthalmology) Chittagong Medical CollegeNear DeathNo ratings yet
- Diabetic Retinopathy: Dwi Lestari PohanDocument72 pagesDiabetic Retinopathy: Dwi Lestari PohanKelvin MandelaNo ratings yet
- DIabetic REtinopathyDocument34 pagesDIabetic REtinopathyLuqman Khan YousafXaiNo ratings yet
- Diabetic-Retinopathy GGGHGHDocument50 pagesDiabetic-Retinopathy GGGHGHjegannancyNo ratings yet
- Diabetic RetinopathyDocument40 pagesDiabetic RetinopathyNaman MishraNo ratings yet
- Diabetic RetinopathyDocument67 pagesDiabetic RetinopathyFirstyIlminovia0% (1)
- Diabetic ThyDocument36 pagesDiabetic ThyItaNo ratings yet
- Diabetic RetinopathyDocument48 pagesDiabetic Retinopathykaran.A.K100% (1)
- AiraDocument17 pagesAiraPrincess Aira Bucag CarbonelNo ratings yet
- DR and Its ManagementDocument76 pagesDR and Its ManagementAravind KumarNo ratings yet
- Retinal Vascular Diseas E: Christine Anne D. EspejaDocument25 pagesRetinal Vascular Diseas E: Christine Anne D. EspejaPaolo QuezonNo ratings yet
- Diabetic Retinopathy: Johnson Marystella Rahul Imd 14 2 A Roll No 34Document17 pagesDiabetic Retinopathy: Johnson Marystella Rahul Imd 14 2 A Roll No 34J.m.RahulNo ratings yet
- Diabetic Retinopathy New-1Document99 pagesDiabetic Retinopathy New-1Sana AzimNo ratings yet
- Diabetic RetinopathyDocument101 pagesDiabetic RetinopathyMohiuddin AhmedNo ratings yet
- Diabetic RetinopatiDocument44 pagesDiabetic RetinopatiLaurensia MassariNo ratings yet
- Diabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Document41 pagesDiabetic Retinopathy: Muhammed Aslam Ps Roll No. 43Baba YagaNo ratings yet
- Lecture 11 Retina 1Document44 pagesLecture 11 Retina 1ؤيؤييسيNo ratings yet
- A Deep Learning Approach For The Detection of Diabetic RetinopathyDocument55 pagesA Deep Learning Approach For The Detection of Diabetic RetinopathyjegannancyNo ratings yet
- Diabetic RetinopathyDocument44 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Diabetic RetinopathyDocument73 pagesDiabetic RetinopathyGetLyricsNo ratings yet
- Diabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerDocument32 pagesDiabetic Retinopathy: DR Paavan Kalra Department of Ophthalmology, S P Medical College, BikanerCarlos HerreraNo ratings yet
- Diabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Document40 pagesDiabetik Retinopati: Dr. Delfi, Mked (Oph), SPM (K)Franky Frans SihombingNo ratings yet
- Diabetic RetinopathyDocument55 pagesDiabetic RetinopathyDrSaid Hussein GediNo ratings yet
- Diabetic With The EyeDocument50 pagesDiabetic With The EyeJianhua ShiNo ratings yet
- Diabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaDocument13 pagesDiabetic Retinopathy: by Mohamad Faizul Abu Hanifa Tillai SharimalaMohamad Faizul Abu HanifaNo ratings yet
- Retinopatia Diabetica 2018Document34 pagesRetinopatia Diabetica 2018Fanny ParraNo ratings yet
- Ico Guidelines For Diabetic Eye CareDocument19 pagesIco Guidelines For Diabetic Eye CareMuhammad Usman Salim100% (1)
- Diabetic RetinopathyDocument78 pagesDiabetic RetinopathyAnumeha Jindal100% (1)
- RetinopathyDocument64 pagesRetinopathySiti NcitNo ratings yet
- Diabetic Retinopathy Presentations (Can Still Use The Older Classification)Document6 pagesDiabetic Retinopathy Presentations (Can Still Use The Older Classification)gdudex118811No ratings yet
- Diabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDDocument55 pagesDiabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDadi amaliNo ratings yet
- Diabetic Eye Disease: Academic Unit of OphthalmologyDocument35 pagesDiabetic Eye Disease: Academic Unit of Ophthalmologyruwan555No ratings yet
- Diabetic RetinopathyDocument43 pagesDiabetic RetinopathyBrampp HimawanNo ratings yet
- Simpo 13.3 - DR Rova - How To Avoid Blindness in Diabetic Eye Disease - PIT IDI Jabar 2018Document51 pagesSimpo 13.3 - DR Rova - How To Avoid Blindness in Diabetic Eye Disease - PIT IDI Jabar 2018Nadar RizatullahNo ratings yet
- Refrat Retinopati-DiabetikDocument20 pagesRefrat Retinopati-DiabetikDea NabilaNo ratings yet
- Retinal Disorders Med VDocument66 pagesRetinal Disorders Med Vhenok birukNo ratings yet
- Kuliah Retina by Widi 2Document57 pagesKuliah Retina by Widi 2DERYGP96 GENIUSNo ratings yet
- Vascular Disorders of RetinaDocument46 pagesVascular Disorders of RetinaSubash BasnetNo ratings yet
- Kuliah VitreoretinaDocument30 pagesKuliah VitreoretinaMoch. NabilNo ratings yet
- RetinaDocument82 pagesRetinafebienaNo ratings yet
- Nonproliferative Diabetic Retinopathy and Diabetic Macular EdemaDocument37 pagesNonproliferative Diabetic Retinopathy and Diabetic Macular EdemaBhumika RathNo ratings yet
- Vitreo Retinal DisordersDocument47 pagesVitreo Retinal DisordersTabreez KhanNo ratings yet
- مح١٨Document44 pagesمح١٨جهاد إبراهيمNo ratings yet
- Diabetic Retinopathy DR KatariaDocument65 pagesDiabetic Retinopathy DR KatariaDr Sandeep Kataria100% (1)
- BCS 5.02 - Organ Pathology in Diabetes - DR Saeed Alshieban 2022Document39 pagesBCS 5.02 - Organ Pathology in Diabetes - DR Saeed Alshieban 2022MATHS By AbdulrahmanNo ratings yet
- ICOGuidelins For DiabeticEye CareDocument28 pagesICOGuidelins For DiabeticEye CareIrfan SadiqNo ratings yet
- DM ComplicationsDocument97 pagesDM ComplicationsElena Borş MorariNo ratings yet
- Vitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkiDocument45 pagesVitreoretina: DR - Reinne Natali Christine, SPM Dept. Ilmu Penyakit Mata FK Uki / Rsu FK UkitusuksedotanNo ratings yet
- Retinal Diseases (Notes)Document76 pagesRetinal Diseases (Notes)khloud ywsefNo ratings yet
- Diabetes Mellitus ComplicationsDocument64 pagesDiabetes Mellitus ComplicationsAdria Putra FarhandikaNo ratings yet
- Acute Painless Loss of Vision: DR S P Mukherjee Ophthalmology, KPCMCHDocument17 pagesAcute Painless Loss of Vision: DR S P Mukherjee Ophthalmology, KPCMCHJayanti Neogi SardarNo ratings yet
- Chronic Complications of Diabetes MellitusDocument53 pagesChronic Complications of Diabetes MellitusAli Murtaza AbbasNo ratings yet
- Retinal Vascular DisordersDocument52 pagesRetinal Vascular Disorderssushma shresthaNo ratings yet
- Modified Management of Diabetic RetinopathyDocument54 pagesModified Management of Diabetic RetinopathyAnviNo ratings yet
- Diabetes AND The Eye: Juliana Bentil Deborah AddoDocument50 pagesDiabetes AND The Eye: Juliana Bentil Deborah Addogideon A. owusuNo ratings yet
- Diabetic Retinopathy GradingDocument64 pagesDiabetic Retinopathy Gradingfadzil hamidNo ratings yet
- PSSS Mata Merah Visus Menurun PerlahanDocument44 pagesPSSS Mata Merah Visus Menurun PerlahandeyshieNo ratings yet
- Diabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDDocument56 pagesDiabetic Retinopathy: Ines Serrano MD Evan Waxman MD PHDmawar2505No ratings yet
- Retinopati Diabetik - 1Document19 pagesRetinopati Diabetik - 1Yoyada SitorusNo ratings yet
- Diabetic Retinopathy: Introduction to Novel Treatment StrategiesFrom EverandDiabetic Retinopathy: Introduction to Novel Treatment StrategiesNo ratings yet
- Viral ConjunctivitisDocument30 pagesViral ConjunctivitisDr Sravya M VNo ratings yet
- Siegel's SpeculumDocument12 pagesSiegel's SpeculumDr Sravya M VNo ratings yet
- Anatomy of EyelidsDocument25 pagesAnatomy of EyelidsDr Sravya M VNo ratings yet
- Kapala Rogas - ModernDocument23 pagesKapala Rogas - ModernDr Sravya M VNo ratings yet
- TinnitusDocument18 pagesTinnitusDr Sravya M VNo ratings yet
- Hearing LossDocument68 pagesHearing LossDr Sravya M VNo ratings yet
- Hearing EvaluationDocument151 pagesHearing EvaluationDr Sravya M VNo ratings yet
- Physiology of HearingDocument30 pagesPhysiology of HearingDr Sravya M VNo ratings yet
- Examination of EyeDocument39 pagesExamination of EyeDr Sravya M VNo ratings yet
- Risk For Decreased Cardiac Output NCPDocument2 pagesRisk For Decreased Cardiac Output NCPMae Denn LabordoNo ratings yet
- Congenital Heart DiseaseDocument37 pagesCongenital Heart Diseaseveralynnp100% (1)
- Biochem SGD 3Document4 pagesBiochem SGD 3Hemanth KokaNo ratings yet
- Full Download PDF of Medical Secrets 6th Edition Mary P. Harward - Ebook PDF All ChapterDocument69 pagesFull Download PDF of Medical Secrets 6th Edition Mary P. Harward - Ebook PDF All Chapterphakhijayahr100% (7)
- Hematogenous Spread. Lymphatic Spread.: 275 Characteristics of Benign and Malignant NeoplasmsDocument4 pagesHematogenous Spread. Lymphatic Spread.: 275 Characteristics of Benign and Malignant NeoplasmsGin TokiNo ratings yet
- Laboratory Test Report: Test Name Result Biological Reference Interval 25 (OH) VIT D2 ErgocalciferolDocument4 pagesLaboratory Test Report: Test Name Result Biological Reference Interval 25 (OH) VIT D2 ErgocalciferolEkta SinhaNo ratings yet
- Insertion of An Intra-Aortic Balloon Catheter: PurposeDocument4 pagesInsertion of An Intra-Aortic Balloon Catheter: PurposeGloria KartikaNo ratings yet
- GenogramDocument10 pagesGenogrammohamadNo ratings yet
- Internship Logbook 2020Document136 pagesInternship Logbook 2020MaleehaNo ratings yet
- DRUG STUDY: Metoprolol - BetalocDocument1 pageDRUG STUDY: Metoprolol - BetalocYum C100% (1)
- Doppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesDocument12 pagesDoppler Systolic Signal Void in Hypertrophic Cardiomyopathy Apical Aneurysm and Severe Obstruction Without Elevated Intraventricular VelocitiesAbraham PaulNo ratings yet
- Pathophysiology of Respiratory System Feghiu I., Tacu L. Lutan VDocument55 pagesPathophysiology of Respiratory System Feghiu I., Tacu L. Lutan VLunguVictoriaNo ratings yet
- Hormonal TherapiesDocument39 pagesHormonal TherapiesJalal EltabibNo ratings yet
- National Emergency Nurses Association: Core CompetenciesDocument8 pagesNational Emergency Nurses Association: Core CompetenciesJordanian CopyNo ratings yet
- Peripheral Vascular Disease and DiabetesDocument8 pagesPeripheral Vascular Disease and DiabetesChikezie OnwukweNo ratings yet
- Atrial FibrillationDocument20 pagesAtrial Fibrillationjack sawdaNo ratings yet
- Cardiovascular SystemDocument15 pagesCardiovascular SystemCapper RuedaNo ratings yet
- MSN Questions 100Document16 pagesMSN Questions 100Efreignz Mangay-at KinomesNo ratings yet
- How Animals Survive (Circulation and GasDocument24 pagesHow Animals Survive (Circulation and GasJohn Ted BañezNo ratings yet
- Chapter 15 - Cardiovascular SystemDocument89 pagesChapter 15 - Cardiovascular SystemOliver Namyalo100% (1)
- CC Lec Mod 3Document13 pagesCC Lec Mod 38wgmhh9ks9No ratings yet
- Ischemic StrokeDocument8 pagesIschemic StrokeSofía Maltés GarridoNo ratings yet
- Fact Sheeton Canola OilDocument15 pagesFact Sheeton Canola OilMonika ThadeaNo ratings yet
- Cardio System 2Document1 pageCardio System 2api-298312370No ratings yet
- General Medicine Lec4 Adrenal GlandsDocument9 pagesGeneral Medicine Lec4 Adrenal GlandsAli MONo ratings yet
- Lectura Previa3-Approach To The Patient With Abnormal Vital SignsDocument7 pagesLectura Previa3-Approach To The Patient With Abnormal Vital SignsEdwin Robles NorabuenaNo ratings yet
- 7 DkaDocument28 pages7 DkaFuad Aman AbjNo ratings yet
- Transplant and Dialysis Handbook 2nd Edition January 2017Document125 pagesTransplant and Dialysis Handbook 2nd Edition January 2017nathanielNo ratings yet