Download as ppt, pdf, or txt
You might also like
- Ebook PDF Clinical Obstetrics and Gynaecology 4th Edition PDFDocument41 pagesEbook PDF Clinical Obstetrics and Gynaecology 4th Edition PDFcharles.macdonald43098% (43)
- Ray Brown - Bles For Basie Bass Transcription PDFDocument3 pagesRay Brown - Bles For Basie Bass Transcription PDFToms PoišsNo ratings yet
- Encyclopedia For Snare Drum - Forrest Clark PDFDocument118 pagesEncyclopedia For Snare Drum - Forrest Clark PDFMonica Gallego100% (3)
- 1880, Chas A. Sterlinger & Co, Detroit, US PDFDocument324 pages1880, Chas A. Sterlinger & Co, Detroit, US PDFHouse HistoriesNo ratings yet
- Uworld - SURGERYDocument55 pagesUworld - SURGERYNikxyNo ratings yet
- Florencio Medina's Report On Dr. Max Goldberger's Proposal For Catalytic ResearchDocument9 pagesFlorencio Medina's Report On Dr. Max Goldberger's Proposal For Catalytic ResearchVerafiles NewsroomNo ratings yet
- Nfor M Co: N Eri /ln9qDocument2 pagesNfor M Co: N Eri /ln9qfawwazi mulNo ratings yet
- E X Ercises: ExercisesDocument3 pagesE X Ercises: ExercisesPamelaDeLacruzZavalaNo ratings yet
- Adobe Scan Dec 14, 2020Document23 pagesAdobe Scan Dec 14, 2020A MesihaNo ratings yet
- Adobe Scan Apr 11, 2023Document6 pagesAdobe Scan Apr 11, 2023KunalNo ratings yet
- Adobe Scan Nov 21, 2023Document25 pagesAdobe Scan Nov 21, 2023Umesh JogeNo ratings yet
- Scan 26 Ago. 2018 PDFDocument3 pagesScan 26 Ago. 2018 PDFAlberto Lazo ManriqueNo ratings yet
- Trade LicenseDocument1 pageTrade LicenseISD OfficialNo ratings yet
- 2 PDocument20 pages2 PRajiniNo ratings yet
- Fountain of Light Christian Academy: Science WORKSHEET #9 Quarter Name: Date: May 5Document2 pagesFountain of Light Christian Academy: Science WORKSHEET #9 Quarter Name: Date: May 5Heidy CastellanosNo ratings yet
- Adobe Scan Apr 01, 2021Document14 pagesAdobe Scan Apr 01, 2021Aliza JabbarNo ratings yet
- f3.cr.t E.: 1tR '2laDocument4 pagesf3.cr.t E.: 1tR '2laaw awNo ratings yet
- Kedaar Phy 1.Document5 pagesKedaar Phy 1.myfreefire1kkNo ratings yet
- Torsion Pendulum LabDocument4 pagesTorsion Pendulum LabWomba LukamaNo ratings yet
- Win The PainDocument6 pagesWin The PainhardikNo ratings yet
- Medical Docs 4.5.20Document3 pagesMedical Docs 4.5.20Sanjay ThakkarNo ratings yet
- Brass ExcerptsDocument25 pagesBrass ExcerptsAddie ChannonNo ratings yet
- Scan 10-Dec-2019 PDFDocument8 pagesScan 10-Dec-2019 PDFManoj RajanNo ratings yet
- E Ferrovie Metropolitane: MetroDocument2 pagesE Ferrovie Metropolitane: MetroDiana Teodora HuzumNo ratings yet
- Pradeep CordinateDocument8 pagesPradeep CordinateJatinNo ratings yet
- Adobe Scan 03 Jun 2023Document15 pagesAdobe Scan 03 Jun 2023SS PSNo ratings yet
- EspectrofotometroDocument68 pagesEspectrofotometroRafa TejedaNo ratings yet
- Dutilleux SonatineDocument23 pagesDutilleux SonatineShaya EldarNo ratings yet
- CN Practical-3 en No-196400307133Document4 pagesCN Practical-3 en No-196400307133Hell GamingNo ratings yet
- Adobe Scan 29 Feb 2024Document1 pageAdobe Scan 29 Feb 2024deepalijain4No ratings yet
- Building Maintenance 1835Document16 pagesBuilding Maintenance 1835karunamoorthi_p2209No ratings yet
- Adobe Scan 11 May 2024Document12 pagesAdobe Scan 11 May 2024kj bull j rayNo ratings yet
- Escaneo 26 Jul 2019Document2 pagesEscaneo 26 Jul 2019Juanvi Lladosa ArnauNo ratings yet
- Workbook Units 9 & 10Document13 pagesWorkbook Units 9 & 10csi553006No ratings yet
- Brahms - Cello PartDocument11 pagesBrahms - Cello PartGlòria Expósito PérezNo ratings yet
- 第42課_本文_肉を食べるとDocument6 pages第42課_本文_肉を食べるとHaresvf HaresvfNo ratings yet
- K.S. Chalam 'Constitutional Status of Civil Service in India'Document6 pagesK.S. Chalam 'Constitutional Status of Civil Service in India'Sunaina LalNo ratings yet
- Salt Analysis FormatDocument2 pagesSalt Analysis FormatArchieNo ratings yet
- Scan 17 Oct 2021Document3 pagesScan 17 Oct 2021irannaNo ratings yet
- The First NoelDocument2 pagesThe First NoelAntonio KrisantoNo ratings yet
- Physio Tests BPSDocument9 pagesPhysio Tests BPSKaran SoniNo ratings yet
- Gen Chem NotesDocument4 pagesGen Chem Notes5403 Pranamya PradeepNo ratings yet
- Flute Concerto V1Document7 pagesFlute Concerto V1Victor Ricardo Gonzalez OrtizNo ratings yet
- Adobe Scan Jul 07, 2023Document9 pagesAdobe Scan Jul 07, 2023MartinNo ratings yet
- Liberty Gold Investments InvoicesDocument2 pagesLiberty Gold Investments InvoicesLeila DouganNo ratings yet
- 10 THDocument2 pages10 THashutosh nagaichNo ratings yet
- KHANIA CESSA YULINDRA - 1A TLM - BIOKIMIA VITAMIN 31 Maret 2023Document1 pageKHANIA CESSA YULINDRA - 1A TLM - BIOKIMIA VITAMIN 31 Maret 2023Khania YulindraNo ratings yet
- Domenico Scarlatti Five PiecesDocument6 pagesDomenico Scarlatti Five PiecesMarco PipernoNo ratings yet
- (Abridged) Forged in Battle - Soldier CareerDocument32 pages(Abridged) Forged in Battle - Soldier CareerMichael CragerNo ratings yet
- DeASI Score in DermatophytosisDocument3 pagesDeASI Score in DermatophytosisSwarnali MaitiNo ratings yet
- Imp Questions11Document6 pagesImp Questions11krsrao74No ratings yet
- Tamaño: Esta Por Partículas Las Roe - As. en f/1S. Arenas, Limos, ArcillasDocument4 pagesTamaño: Esta Por Partículas Las Roe - As. en f/1S. Arenas, Limos, ArcillasCinthya VargasNo ratings yet
- F'l..dt:/... : 'Jra.u1Document5 pagesF'l..dt:/... : 'Jra.u1Ohol Rohan BhaskarNo ratings yet
- Adobe Scan Jun 01, 2023Document1 pageAdobe Scan Jun 01, 2023acc.vinitjhaNo ratings yet
- Simple Pendulum LabDocument4 pagesSimple Pendulum LabWomba LukamaNo ratings yet
- Deanna Petherbridge: Primacy of DrawingDocument516 pagesDeanna Petherbridge: Primacy of DrawingGabriel CoelhoNo ratings yet
- Pagal, J. Q#2 MW AmDocument3 pagesPagal, J. Q#2 MW AmJayson PagalNo ratings yet
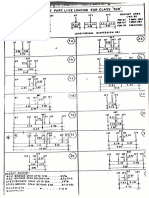
- L.lii: Parl Li Loaoini ClassDocument4 pagesL.lii: Parl Li Loaoini ClassStructural SpreadsheetsNo ratings yet
- King Mon1 Kut's University of Technology Thonburi: 1'111 EEE 111 Electric Circuit Analysis 9.00-12.00Document15 pagesKing Mon1 Kut's University of Technology Thonburi: 1'111 EEE 111 Electric Circuit Analysis 9.00-12.00CHAYANIN AKETANANUNNo ratings yet
- HZGEXK163664455Document89 pagesHZGEXK163664455Elgawda CairoNo ratings yet
- Labour Law - I by Ashok JainDocument172 pagesLabour Law - I by Ashok Jainghumu ghumuNo ratings yet
- Imagine Please: Early Radio Broadcasting in British ColumbiaFrom EverandImagine Please: Early Radio Broadcasting in British ColumbiaNo ratings yet
- 1.6 Million Head Injuries in US 250,000 Hospital Admissions: 70,000 90,000 Permanent Neurologic DisabilitiesDocument87 pages1.6 Million Head Injuries in US 250,000 Hospital Admissions: 70,000 90,000 Permanent Neurologic DisabilitiesDr shehwarNo ratings yet
- Invertogram 180604185707Document57 pagesInvertogram 180604185707Dr shehwar100% (1)
- SHC SurgProphylaxisGuidelinesDocument6 pagesSHC SurgProphylaxisGuidelinesDr shehwar100% (1)
- Efficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDocument4 pagesEfficacy of Dexamethasone For Reducing Postoperative Nausea and Vomiting and Analgesic Requirements After ThyroidectomyDr shehwarNo ratings yet
- MRI Forefoot - MRI Forefoot Protocol and PlanningDocument10 pagesMRI Forefoot - MRI Forefoot Protocol and Planningradiologi.rsgmNo ratings yet
- Cancer Pain HomeopathyDocument50 pagesCancer Pain HomeopathyKaran PurohitNo ratings yet
- Head InjuryDocument3 pagesHead InjuryItzel MahiyaNo ratings yet
- Moonwalk National High School: Schools Division of Parañaque CityDocument4 pagesMoonwalk National High School: Schools Division of Parañaque CityRowena TabisoraNo ratings yet
- SEIZURESDocument6 pagesSEIZURESRamgie AcuñaNo ratings yet
- BrainlanguageDocument30 pagesBrainlanguageAnmolNo ratings yet
- Science g6 q2 w2-3 Fillable - Jocoh Romero v.2Document7 pagesScience g6 q2 w2-3 Fillable - Jocoh Romero v.2Aljun Alag RollanNo ratings yet
- Group Care 360 Insurance Policy TNCDocument83 pagesGroup Care 360 Insurance Policy TNCArbaz KhanNo ratings yet
- Fetal Pig Dissection WorksheetDocument8 pagesFetal Pig Dissection Worksheetapi-233187566No ratings yet
- NP2 and NP3Document3 pagesNP2 and NP3Portia Dulce ToqueroNo ratings yet
- Case Presentation of Hemorrhagic Stroke (Subarachnoid Hemorrhage)Document69 pagesCase Presentation of Hemorrhagic Stroke (Subarachnoid Hemorrhage)verna88% (24)
- Long Term MemoryDocument4 pagesLong Term MemoryCamelia UrsanNo ratings yet
- Anatomy and Physiology of GITDocument4 pagesAnatomy and Physiology of GITyassyrnNo ratings yet
- 14 Osteopathic Manipulative Treatment - HVLA Procedure - Cervical Vertebrae - StatPearls - NCBI BookshelfDocument11 pages14 Osteopathic Manipulative Treatment - HVLA Procedure - Cervical Vertebrae - StatPearls - NCBI Bookshelfjaswant bhadaneNo ratings yet
- The Orbit: D.Hanan Darif 2016Document16 pagesThe Orbit: D.Hanan Darif 2016henry cazeNo ratings yet
- Case Study Breast CancerDocument16 pagesCase Study Breast CancerDanica Lorine Robino TaguinodNo ratings yet
- Pediatric TuberculosisDocument19 pagesPediatric TuberculosisRajath Kumar K R KNo ratings yet
- Inside The Living Body Video Cloze PassageDocument8 pagesInside The Living Body Video Cloze Passageapi-243860050No ratings yet
- Upper and Lower Motor NeuronDocument28 pagesUpper and Lower Motor NeuronDr Abdullah SubhanNo ratings yet
- Primary Chemotherapy: Adjuvant Chemotherapy: Neoadjuvant Chemotherapy: Treatment RegimensDocument7 pagesPrimary Chemotherapy: Adjuvant Chemotherapy: Neoadjuvant Chemotherapy: Treatment RegimensNoelani-Mei AscioNo ratings yet
- 6 Thrombosis MorphologyDocument20 pages6 Thrombosis MorphologySawera RaheemNo ratings yet
- Head Trauma: Khamim Thohari Rsud DR Muhammad Soewandhie SurabayaDocument33 pagesHead Trauma: Khamim Thohari Rsud DR Muhammad Soewandhie SurabayaJessica Alexandria WuNo ratings yet
- Pituitary Gland Anatomy: Embryologic DevelopmentDocument9 pagesPituitary Gland Anatomy: Embryologic DevelopmentRafaelPetitNo ratings yet
- Textbook Endocrine Surgery Second Edition Demetrius Pertsemlidis Ebook All Chapter PDFDocument53 pagesTextbook Endocrine Surgery Second Edition Demetrius Pertsemlidis Ebook All Chapter PDFwilliam.finan539100% (17)
- AnaPhy SAS 1Document5 pagesAnaPhy SAS 1Zylith NanaseNo ratings yet
- Pandora Poikilos - Excuse Me, My Brains Have Stepped OutDocument168 pagesPandora Poikilos - Excuse Me, My Brains Have Stepped OutAaliyah CsmrtNo ratings yet
- InfraTapp - Infra Tapp - Manual ENGDocument64 pagesInfraTapp - Infra Tapp - Manual ENGEliaNo ratings yet
- Anesthetics - and - Analgesics DOSE - Sheep and GOATDocument102 pagesAnesthetics - and - Analgesics DOSE - Sheep and GOATjiregnaNo ratings yet