
JTG Slides-Edited
JTG Slides-Edited
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gender SensitivityDocument10 pagesGender Sensitivityapi-3704562100% (10)
- Gender SensitivityDocument2 pagesGender Sensitivityapi-370456296% (26)
- Cognitive Observation Ece 252Document3 pagesCognitive Observation Ece 252api-291058148No ratings yet
- PulmoconDocument64 pagesPulmoconapi-3704562100% (1)
- SURGERYDocument36 pagesSURGERYapi-3704562No ratings yet
- Vasculitis SyndromesDocument9 pagesVasculitis Syndromesapi-3704562No ratings yet
- Kaplan Community EpidemDocument3 pagesKaplan Community Epidemapi-3704562No ratings yet
- Dr. JTG Presentation (Diarrheas)Document33 pagesDr. JTG Presentation (Diarrheas)api-3704562No ratings yet
- PlasticischwartsDocument3 pagesPlasticischwartsapi-3704562No ratings yet
- SLE SummaryDocument5 pagesSLE Summaryapi-3704562100% (1)
- Psych AdjustmentDocument2 pagesPsych Adjustmentapi-3704562No ratings yet
- Neurosurgery Case 1Document111 pagesNeurosurgery Case 1api-3704562No ratings yet
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562100% (1)
- CHAPTER 127 MENINGOCOCCAL INFECTIONS SummaryDocument3 pagesCHAPTER 127 MENINGOCOCCAL INFECTIONS Summaryapi-3704562No ratings yet
- Ringkasan MeningitisDocument2 pagesRingkasan Meningitisd17oNo ratings yet
- HUMAN HERPES VIRUS Types 6Document1 pageHUMAN HERPES VIRUS Types 6api-3704562100% (1)
- Employment Document Folder ListsDocument90 pagesEmployment Document Folder ListsIsna FauziahNo ratings yet
- Growing Up Spiritually - Kenneth E. Hagin (PDFDrive)Document163 pagesGrowing Up Spiritually - Kenneth E. Hagin (PDFDrive)chrisjephthah6No ratings yet
- HPP Frutta CreamDocument24 pagesHPP Frutta Creamimam purnamaNo ratings yet
- Unit 5. PHCDocument24 pagesUnit 5. PHCFenembar MekonnenNo ratings yet
- Botanical Orign: Peppermint OilDocument4 pagesBotanical Orign: Peppermint OilSidra TariqNo ratings yet
- Chapter 6 Food Handlers Safety HygieneDocument20 pagesChapter 6 Food Handlers Safety HygieneIrish MalabananNo ratings yet
- Modals of Obligation and Permission WorksheetDocument2 pagesModals of Obligation and Permission Worksheetyuleysi yuleysivelezmorogmail.comNo ratings yet
- Historia Tartarorum EcclesiasticaDocument4 pagesHistoria Tartarorum EcclesiasticaVladimir SaricNo ratings yet
- Eat Right For A Healthy Life (PE)Document15 pagesEat Right For A Healthy Life (PE)Yan100% (4)
- Shamanic HealingDocument41 pagesShamanic HealingMeraki Mary50% (2)
- NiBallast TM BWMS v-2021Document21 pagesNiBallast TM BWMS v-2021王杰No ratings yet
- P I Iso TP M v13 enDocument6 pagesP I Iso TP M v13 enPedro SepúlvedaNo ratings yet
- Introduction of Community MedicineDocument111 pagesIntroduction of Community MedicineSanjeet SahNo ratings yet
- UN SMA 2008 Bahasa Inggris: Kode Soal P44Document7 pagesUN SMA 2008 Bahasa Inggris: Kode Soal P44hestyNo ratings yet
- CSE499 Final Report 2023Document56 pagesCSE499 Final Report 2023sayem bin abdullah al mahfuzNo ratings yet
- Msds Heksana - 2 PDFDocument6 pagesMsds Heksana - 2 PDFGelisaNo ratings yet
- SavedrecsDocument615 pagesSavedrecsMARIBEL BARBECHONo ratings yet
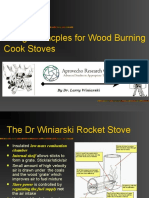
- Design Princples For Wood Burning Cook StovesDocument20 pagesDesign Princples For Wood Burning Cook Stoveshana temesegenNo ratings yet
- Sonia Research ProposalDocument59 pagesSonia Research Proposalmullamuskaan95No ratings yet
- Vaxigrip Tetra Pi Nh19-20Document2 pagesVaxigrip Tetra Pi Nh19-20A. shahizaNo ratings yet
- 1st and 2nd Assignment of PDDDocument2 pages1st and 2nd Assignment of PDDYash Bhardwaj FitnessNo ratings yet
- Managing People - AssignmentDocument10 pagesManaging People - AssignmentayeshaNo ratings yet
- Electronic Cash Register Programming-ManualDocument27 pagesElectronic Cash Register Programming-ManualRendy Adam FarhanNo ratings yet
- PCAR Contractors ManualDocument219 pagesPCAR Contractors ManualDefendAChildNo ratings yet
- Natural Remedies For Heart DiseaseDocument8 pagesNatural Remedies For Heart DiseaseNur HowladerNo ratings yet
- IPC Medium-Pressure Internal Gear Pumps: Technical Data SheetDocument20 pagesIPC Medium-Pressure Internal Gear Pumps: Technical Data SheetNutrición SaludableNo ratings yet
- CP SYSTEM - DESIGN DOCUMENT (Rev.01)Document46 pagesCP SYSTEM - DESIGN DOCUMENT (Rev.01)suman ghosh100% (1)
- Cost of The DietDocument68 pagesCost of The DietSomao JoeNo ratings yet
- Venezuelan Food Christmas EditionDocument5 pagesVenezuelan Food Christmas Editionapi-584143560No ratings yet




















































































Download as ppt, pdf, or txt
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5822)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1093)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (852)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (898)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (349)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (403)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Gender SensitivityDocument10 pagesGender Sensitivityapi-3704562100% (10)
- Gender SensitivityDocument2 pagesGender Sensitivityapi-370456296% (26)
- Cognitive Observation Ece 252Document3 pagesCognitive Observation Ece 252api-291058148No ratings yet
- PulmoconDocument64 pagesPulmoconapi-3704562100% (1)
- SURGERYDocument36 pagesSURGERYapi-3704562No ratings yet
- Vasculitis SyndromesDocument9 pagesVasculitis Syndromesapi-3704562No ratings yet
- Kaplan Community EpidemDocument3 pagesKaplan Community Epidemapi-3704562No ratings yet
- Dr. JTG Presentation (Diarrheas)Document33 pagesDr. JTG Presentation (Diarrheas)api-3704562No ratings yet
- PlasticischwartsDocument3 pagesPlasticischwartsapi-3704562No ratings yet
- SLE SummaryDocument5 pagesSLE Summaryapi-3704562100% (1)
- Psych AdjustmentDocument2 pagesPsych Adjustmentapi-3704562No ratings yet
- Neurosurgery Case 1Document111 pagesNeurosurgery Case 1api-3704562No ratings yet
- Bacterial and Viral MeningitisDocument12 pagesBacterial and Viral Meningitisapi-3704562100% (1)
- CHAPTER 127 MENINGOCOCCAL INFECTIONS SummaryDocument3 pagesCHAPTER 127 MENINGOCOCCAL INFECTIONS Summaryapi-3704562No ratings yet
- Ringkasan MeningitisDocument2 pagesRingkasan Meningitisd17oNo ratings yet
- HUMAN HERPES VIRUS Types 6Document1 pageHUMAN HERPES VIRUS Types 6api-3704562100% (1)
- Employment Document Folder ListsDocument90 pagesEmployment Document Folder ListsIsna FauziahNo ratings yet
- Growing Up Spiritually - Kenneth E. Hagin (PDFDrive)Document163 pagesGrowing Up Spiritually - Kenneth E. Hagin (PDFDrive)chrisjephthah6No ratings yet
- HPP Frutta CreamDocument24 pagesHPP Frutta Creamimam purnamaNo ratings yet
- Unit 5. PHCDocument24 pagesUnit 5. PHCFenembar MekonnenNo ratings yet
- Botanical Orign: Peppermint OilDocument4 pagesBotanical Orign: Peppermint OilSidra TariqNo ratings yet
- Chapter 6 Food Handlers Safety HygieneDocument20 pagesChapter 6 Food Handlers Safety HygieneIrish MalabananNo ratings yet
- Modals of Obligation and Permission WorksheetDocument2 pagesModals of Obligation and Permission Worksheetyuleysi yuleysivelezmorogmail.comNo ratings yet
- Historia Tartarorum EcclesiasticaDocument4 pagesHistoria Tartarorum EcclesiasticaVladimir SaricNo ratings yet
- Eat Right For A Healthy Life (PE)Document15 pagesEat Right For A Healthy Life (PE)Yan100% (4)
- Shamanic HealingDocument41 pagesShamanic HealingMeraki Mary50% (2)
- NiBallast TM BWMS v-2021Document21 pagesNiBallast TM BWMS v-2021王杰No ratings yet
- P I Iso TP M v13 enDocument6 pagesP I Iso TP M v13 enPedro SepúlvedaNo ratings yet
- Introduction of Community MedicineDocument111 pagesIntroduction of Community MedicineSanjeet SahNo ratings yet
- UN SMA 2008 Bahasa Inggris: Kode Soal P44Document7 pagesUN SMA 2008 Bahasa Inggris: Kode Soal P44hestyNo ratings yet
- CSE499 Final Report 2023Document56 pagesCSE499 Final Report 2023sayem bin abdullah al mahfuzNo ratings yet
- Msds Heksana - 2 PDFDocument6 pagesMsds Heksana - 2 PDFGelisaNo ratings yet
- SavedrecsDocument615 pagesSavedrecsMARIBEL BARBECHONo ratings yet
- Design Princples For Wood Burning Cook StovesDocument20 pagesDesign Princples For Wood Burning Cook Stoveshana temesegenNo ratings yet
- Sonia Research ProposalDocument59 pagesSonia Research Proposalmullamuskaan95No ratings yet
- Vaxigrip Tetra Pi Nh19-20Document2 pagesVaxigrip Tetra Pi Nh19-20A. shahizaNo ratings yet
- 1st and 2nd Assignment of PDDDocument2 pages1st and 2nd Assignment of PDDYash Bhardwaj FitnessNo ratings yet
- Managing People - AssignmentDocument10 pagesManaging People - AssignmentayeshaNo ratings yet
- Electronic Cash Register Programming-ManualDocument27 pagesElectronic Cash Register Programming-ManualRendy Adam FarhanNo ratings yet
- PCAR Contractors ManualDocument219 pagesPCAR Contractors ManualDefendAChildNo ratings yet
- Natural Remedies For Heart DiseaseDocument8 pagesNatural Remedies For Heart DiseaseNur HowladerNo ratings yet
- IPC Medium-Pressure Internal Gear Pumps: Technical Data SheetDocument20 pagesIPC Medium-Pressure Internal Gear Pumps: Technical Data SheetNutrición SaludableNo ratings yet
- CP SYSTEM - DESIGN DOCUMENT (Rev.01)Document46 pagesCP SYSTEM - DESIGN DOCUMENT (Rev.01)suman ghosh100% (1)
- Cost of The DietDocument68 pagesCost of The DietSomao JoeNo ratings yet
- Venezuelan Food Christmas EditionDocument5 pagesVenezuelan Food Christmas Editionapi-584143560No ratings yet