Download as pptx, pdf, or txt
You might also like
- Inf. CasesDocument30 pagesInf. CasesAhmad SobihNo ratings yet
- The F CK You Buffet - Secret Family Recipes of Kids Betrayed by Their Homophobic Parents and A Few Recipes From Good and Kind People Because Balance Is KeyDocument37 pagesThe F CK You Buffet - Secret Family Recipes of Kids Betrayed by Their Homophobic Parents and A Few Recipes From Good and Kind People Because Balance Is KeyBecca60% (5)
- Urinary Tract InfectionDocument23 pagesUrinary Tract InfectionAs SyarifNo ratings yet
- Animals Are People TooDocument2 pagesAnimals Are People TooTashini LileeNo ratings yet
- Indian Plastic Industry, Plastic Industry in India, Plastic Industry, Plastic IndustriesDocument5 pagesIndian Plastic Industry, Plastic Industry in India, Plastic Industry, Plastic IndustriesPriyanshu ChokhaniNo ratings yet
- Configuration 1 TDJ-709015DEI-90FDocument1 pageConfiguration 1 TDJ-709015DEI-90FДмитрий100% (1)
- Urinary Tract Infection: Tbilisi Referral Hospital, Tbilisi, Georgia Nephrologist Nino MaglakelidzeDocument50 pagesUrinary Tract Infection: Tbilisi Referral Hospital, Tbilisi, Georgia Nephrologist Nino MaglakelidzePayal bhagatNo ratings yet
- Gyno Review: Final Surgery Exam 2011Document36 pagesGyno Review: Final Surgery Exam 2011Zee TeeNo ratings yet
- Chapter 36 The Urinary System in GynaecologyDocument19 pagesChapter 36 The Urinary System in Gynaecologypmj050gpNo ratings yet
- ####Bahan Kuliah ISK Blok 23 (Nov 2015)Document32 pages####Bahan Kuliah ISK Blok 23 (Nov 2015)ajengdmrNo ratings yet
- Renal Notes Step 2ckDocument34 pagesRenal Notes Step 2cksamreen100% (1)
- Urinary Tract Infection - Kuliah Mahasiswa - Ferbruari 2017 - EDITDocument52 pagesUrinary Tract Infection - Kuliah Mahasiswa - Ferbruari 2017 - EDITRahmawati HamudiNo ratings yet
- Rinary Ract Nfections: Classification Pathophysiology Risk Factors Clinical Manifestation DiagnosticsDocument27 pagesRinary Ract Nfections: Classification Pathophysiology Risk Factors Clinical Manifestation DiagnosticsDARYmagpantayNo ratings yet
- Urinary Tract Infection (UTI)Document39 pagesUrinary Tract Infection (UTI)Sabita TripathiNo ratings yet
- Pyelonephritis: Departemen Ilmu Penyakit Dalam FK Uii YogyakartaDocument33 pagesPyelonephritis: Departemen Ilmu Penyakit Dalam FK Uii YogyakartaAndaru Tri Setyo WibowoNo ratings yet
- UTI in PregnancyDocument33 pagesUTI in Pregnancyyusufkiduchu8No ratings yet
- Urinary Tract InfectionDocument50 pagesUrinary Tract Infectionpokhara gharipatan100% (1)
- Urinary Tract Infection-AnthieDocument25 pagesUrinary Tract Infection-AnthieGumarbio Setiadi ZakariaNo ratings yet
- Acute and Chronic PyelonephritisDocument7 pagesAcute and Chronic PyelonephritisMatthew Ryan100% (1)
- Im - Uti - Pgi SJ AgbayaniDocument62 pagesIm - Uti - Pgi SJ AgbayaniShareen Joyce AgbayaniNo ratings yet
- Management of Patients With Urinary DisordersDocument94 pagesManagement of Patients With Urinary DisordersJerome RarogalNo ratings yet
- Genitourinary Infections For ClassDocument74 pagesGenitourinary Infections For ClassKashif BurkiNo ratings yet
- An Individual Case Study ON Urinary Tract Infection (UTI) : Southern Isabela General HospitalDocument20 pagesAn Individual Case Study ON Urinary Tract Infection (UTI) : Southern Isabela General HospitalhanapotakoNo ratings yet
- Acute PNDocument36 pagesAcute PNDaniel BondoroiNo ratings yet
- Symptoms: For Bladder InfectionsDocument5 pagesSymptoms: For Bladder InfectionsGene Ryuzaki SeseNo ratings yet
- A Urinary Tract InfectionDocument5 pagesA Urinary Tract InfectionSubodh BhargavNo ratings yet
- UTIs 1Document38 pagesUTIs 1Eduardo Valdez RodríguezNo ratings yet
- 8.urinary Tract Infections-1Document82 pages8.urinary Tract Infections-1fikirjohn8No ratings yet
- Approach To A Patient With Urinary Tract Infection UTI-2Document53 pagesApproach To A Patient With Urinary Tract Infection UTI-2maruf47774No ratings yet
- PielobefritisDocument9 pagesPielobefritisPutri DwiridalNo ratings yet
- Assaignment of UTIDocument11 pagesAssaignment of UTISusmita Mistry JuiNo ratings yet
- Urinary Tract InfectionDocument64 pagesUrinary Tract Infectionmiguel mendezNo ratings yet
- Urinary Ttract InfectionsDocument20 pagesUrinary Ttract InfectionsmohamedomarabdelNo ratings yet
- PyelonephritisDocument24 pagesPyelonephritisfatihahannisahumairaNo ratings yet
- Presentation On Dysuria 1Document25 pagesPresentation On Dysuria 1ankur acharyaNo ratings yet
- Urinary Tract Infection: Akhyar Albaar Haerani RasyidDocument49 pagesUrinary Tract Infection: Akhyar Albaar Haerani Rasyidrolly riksantoNo ratings yet
- Urinary System and Its PathologiesDocument23 pagesUrinary System and Its Pathologiesngachangong victorineNo ratings yet
- Uti RukayyyahDocument40 pagesUti Rukayyyahajusdabo95No ratings yet
- Non-Specific Infections of The Genitourinary SystemDocument47 pagesNon-Specific Infections of The Genitourinary SystemAngela RosaNo ratings yet
- UTI UKI Lecture May 2009 Rev 1Document27 pagesUTI UKI Lecture May 2009 Rev 1godlief leghu kondiNo ratings yet
- NCP Nursing Care Plan For Urinary Tract InfectionsDocument4 pagesNCP Nursing Care Plan For Urinary Tract InfectionsRaveen mayi89% (9)
- Urinary Tract InfectionsDocument71 pagesUrinary Tract Infectionsdayibon499No ratings yet
- Infections of The Urinary TractDocument41 pagesInfections of The Urinary TractGiri DharanNo ratings yet
- 8 Urinary Tract InfectionDocument4 pages8 Urinary Tract Infectionzainabd1964No ratings yet
- Urinary Tract Infections DR Moses KazevuDocument23 pagesUrinary Tract Infections DR Moses KazevuMoses Jr KazevuNo ratings yet
- Urinary EliminationDocument71 pagesUrinary EliminationFrances LiqueNo ratings yet
- Infectious and Inflammatory Disorders of The Urinary SystemDocument16 pagesInfectious and Inflammatory Disorders of The Urinary SystemBibi Renu100% (1)
- Lecture ISK UKI - Dr. Sahala Panggabean SP - PDDocument25 pagesLecture ISK UKI - Dr. Sahala Panggabean SP - PDBen HonorseekerNo ratings yet
- Paediatric UTIDocument24 pagesPaediatric UTIIlobun Faithful IziengbeNo ratings yet
- Urinary Tract InfectionDocument24 pagesUrinary Tract InfectionraddagNo ratings yet
- First Problem: Erwin Budi/405130151Document42 pagesFirst Problem: Erwin Budi/405130151Rilianda SimbolonNo ratings yet
- UTIsDocument25 pagesUTIsAnamul MasumNo ratings yet
- Asymptomatic BacteriuriaDocument23 pagesAsymptomatic BacteriuriaSabita PaudelNo ratings yet
- Pyelonephritis: Urinary Tract Infection Vesicoureteric RefluxDocument12 pagesPyelonephritis: Urinary Tract Infection Vesicoureteric Reflux3ling3No ratings yet
- Urinary Tract Disorders/Infectio NDocument44 pagesUrinary Tract Disorders/Infectio NrintyosoNo ratings yet
- BAHAN KULIAH - Urinary Tract InfectionDocument24 pagesBAHAN KULIAH - Urinary Tract Infectionevi_kkITNo ratings yet
- Predisposing FactorsDocument14 pagesPredisposing FactorsThomas GealonNo ratings yet
- Infeksi Sal KemihDocument41 pagesInfeksi Sal Kemihnovida situmorangNo ratings yet
- K10 - ISK AtasDocument39 pagesK10 - ISK AtasfelixNo ratings yet
- CystitisDocument13 pagesCystitisTin VidovićNo ratings yet
- PYELONEPHRITISDocument16 pagesPYELONEPHRITISshenecajean carajayNo ratings yet
- Acute Pyelonephritis - Salido, Reyes 3CDocument24 pagesAcute Pyelonephritis - Salido, Reyes 3Cmena inezNo ratings yet
- Infectious Diseases - 04Document21 pagesInfectious Diseases - 04Arthur YanezNo ratings yet
- Comprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsFrom EverandComprehensive Insights into Acute Cystitis: Understanding, Management, and Future DirectionsNo ratings yet
- Urinary Tract Infection in Children - Classification, Diagnosis and TreatmentFrom EverandUrinary Tract Infection in Children - Classification, Diagnosis and TreatmentNo ratings yet
- 11 Environmental HealthDocument49 pages11 Environmental HealthAhmad SobihNo ratings yet
- Physical Diagnosis - Learning ObjectivesDocument4 pagesPhysical Diagnosis - Learning ObjectivesAhmad SobihNo ratings yet
- Ahmad Soboh - Bridging PBL Midterm ExamDocument39 pagesAhmad Soboh - Bridging PBL Midterm ExamAhmad SobihNo ratings yet
- Obstetrics & Gynaecology - TopicsDocument5 pagesObstetrics & Gynaecology - TopicsAhmad SobihNo ratings yet
- Family Planning GynecologyDocument20 pagesFamily Planning GynecologyAhmad SobihNo ratings yet
- LobsDocument1 pageLobsAhmad SobihNo ratings yet
- BS IV Case 2 Spring 2024Document17 pagesBS IV Case 2 Spring 2024Ahmad SobihNo ratings yet
- 10 Mental HealthDocument39 pages10 Mental HealthAhmad SobihNo ratings yet
- Family Planning GynecologyDocument10 pagesFamily Planning GynecologyAhmad SobihNo ratings yet
- Efficacy of ContraceptionDocument2 pagesEfficacy of ContraceptionAhmad SobihNo ratings yet
- Cases RheumatologyDocument1 pageCases RheumatologyAhmad SobihNo ratings yet
- Ob Gy1Document9 pagesOb Gy1Ahmad SobihNo ratings yet
- DermatologyDocument8 pagesDermatologyAhmad SobihNo ratings yet
- Dermatology TopicsDocument2 pagesDermatology TopicsAhmad SobihNo ratings yet
- InfectionDocument42 pagesInfectionAhmad SobihNo ratings yet
- L2 - Disorders of The Kidney and Urinary TractDocument35 pagesL2 - Disorders of The Kidney and Urinary TractAhmad SobihNo ratings yet
- Iii PBL 1-6-18Document3 pagesIii PBL 1-6-18Ahmad SobihNo ratings yet
- Biopsy - NephrologyDocument3 pagesBiopsy - NephrologyAhmad SobihNo ratings yet
- Internal Medicine III - Infectious DiseasesDocument32 pagesInternal Medicine III - Infectious DiseasesAhmad SobihNo ratings yet
- DIabetic NephropathyDocument37 pagesDIabetic NephropathyAhmad SobihNo ratings yet
- Brain Stem2Document62 pagesBrain Stem2Ahmad SobihNo ratings yet
- NeurologyDocument1 pageNeurologyAhmad SobihNo ratings yet
- Renal Replacment TherapyDocument30 pagesRenal Replacment TherapyAhmad SobihNo ratings yet
- Nephrology All PPTsDocument399 pagesNephrology All PPTsAhmad SobihNo ratings yet
- Quiz - Neurology - MidtermsDocument12 pagesQuiz - Neurology - MidtermsAhmad SobihNo ratings yet
- HemodyalisisDocument19 pagesHemodyalisisAhmad SobihNo ratings yet
- Internal Medicine II GRDocument86 pagesInternal Medicine II GRAhmad SobihNo ratings yet
- Rheumatology - All PPTsDocument495 pagesRheumatology - All PPTsAhmad SobihNo ratings yet
- Peritoneal DialysisDocument20 pagesPeritoneal DialysisAhmad SobihNo ratings yet
- Mikyas. 2020. Positive Science or Interpretive UnderstandingDocument16 pagesMikyas. 2020. Positive Science or Interpretive UnderstandingMikyas AberaNo ratings yet
- Alfonso Lopez CardiovascularDocument15 pagesAlfonso Lopez Cardiovascularjaniceli0207100% (1)
- Seamo Paper C 2016Document7 pagesSeamo Paper C 2016Sherlly HastriNo ratings yet
- 1524112628010product Manual Page - Forever Active Pro-BDocument2 pages1524112628010product Manual Page - Forever Active Pro-BJosé Antonio CabezaNo ratings yet
- Capt - Pradeep Correa - Growth of The India Economy and Ship BDocument33 pagesCapt - Pradeep Correa - Growth of The India Economy and Ship BacoopsNo ratings yet
- Phytosome: Presented byDocument14 pagesPhytosome: Presented bySari RamadhaniNo ratings yet
- Kenwood B62-2299-20Document2 pagesKenwood B62-2299-20King MaxNo ratings yet
- Bioelectromagnetism. 16. Vectorcardiographic Lead Systems: January 1995Document21 pagesBioelectromagnetism. 16. Vectorcardiographic Lead Systems: January 1995Insani Abdi BangsaNo ratings yet
- Behance EgyptDocument12 pagesBehance Egyptdeepakshi rajputNo ratings yet
- OK-LN SeriesDocument10 pagesOK-LN SeriesSuresh GoddetiNo ratings yet
- All India Aakash Test Series For NEET - 2021 TEST - 6 (Code-C)Document32 pagesAll India Aakash Test Series For NEET - 2021 TEST - 6 (Code-C)Kavyatharsheni S XI-B 46No ratings yet
- MS 1050 - Physics of Solids: - Ranjith RamaduraiDocument25 pagesMS 1050 - Physics of Solids: - Ranjith RamaduraiproNo ratings yet
- Desert Magazine 1942 FebruaryDocument68 pagesDesert Magazine 1942 Februarydm1937100% (5)
- KasaysayanDocument12 pagesKasaysayanJoed RodriguezNo ratings yet
- Invention of Memory RacetrackDocument6 pagesInvention of Memory Racetrackvishals_31No ratings yet
- September 4, 2019: Vladimir S. MiraranDocument16 pagesSeptember 4, 2019: Vladimir S. MiraranPinkz Trinidad TalionNo ratings yet
- De Cuong On He Mon Tieng Anh Lop 6 Len Lop 7Document14 pagesDe Cuong On He Mon Tieng Anh Lop 6 Len Lop 7Quang Hưng NguyễnNo ratings yet
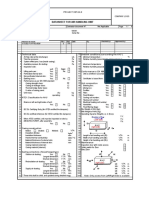
- PILE Cap ULS NDocument4 pagesPILE Cap ULS NKhirai HelpNo ratings yet
- CUK ConverterDocument13 pagesCUK ConverterpakalagopalNo ratings yet
- Guide To Slide in Bridge ConstructionDocument168 pagesGuide To Slide in Bridge ConstructionpassingtimeNo ratings yet
- Chapter-12 Hydro Generator and Excitation System TestsDocument13 pagesChapter-12 Hydro Generator and Excitation System TestsSe SamnangNo ratings yet
- Liver DiseaseDocument19 pagesLiver Diseasenishi kNo ratings yet
- AHU Datasheet Sample Detailed Page 1 of 6 1635440149Document1 pageAHU Datasheet Sample Detailed Page 1 of 6 1635440149alim khanNo ratings yet
- PFCR ManualDocument777 pagesPFCR ManualFlo WheelerNo ratings yet
- SHS 7020Document2 pagesSHS 7020Mariano Diego PosadasNo ratings yet
- PVTOLDocument14 pagesPVTOLJ Chesare Ortega MNo ratings yet