
Anaesthetic Management of Paediatric Emergencies Corrected 3
Anaesthetic Management of Paediatric Emergencies Corrected 3
You might also like
- Case Presentation On Neonatal Sepsis: BY-Anisha ManeDocument45 pagesCase Presentation On Neonatal Sepsis: BY-Anisha ManeAnisha Mane100% (5)
- Neonatal AnaesthesiaDocument61 pagesNeonatal AnaesthesianeneknoraNo ratings yet
- Classification of Newborn, - 130319150346Document45 pagesClassification of Newborn, - 130319150346Ez Ball100% (1)
- Special Considerations in The Premature and Ex-Premature InfantDocument30 pagesSpecial Considerations in The Premature and Ex-Premature InfanteryxspNo ratings yet
- Pediatric SurgeryDocument57 pagesPediatric SurgeryMusekhirNo ratings yet
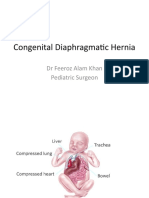
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocument21 pagesCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Common Newborn Problems (2) C1Document39 pagesCommon Newborn Problems (2) C1ZmNo ratings yet
- PREMATURITYDocument27 pagesPREMATURITYHamizi MD HanapiahNo ratings yet
- Assessment and Management of High Risk Neonates DrLawHN PDFDocument45 pagesAssessment and Management of High Risk Neonates DrLawHN PDFShiva KarthikeyanNo ratings yet
- 10 Newborn1Document129 pages10 Newborn1Gerlian Kyle QueridoNo ratings yet
- Preterm Its ProblemsDocument30 pagesPreterm Its ProblemsEnlighten usNo ratings yet
- Pediatric AnesthesiaDocument70 pagesPediatric AnesthesiaEliyan KhanimovNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- 6.1 High Risk New Born-1Document76 pages6.1 High Risk New Born-1ArbzNo ratings yet
- Birth AsphyxiaDocument12 pagesBirth Asphyxiaannu panchalNo ratings yet
- Neonatal Renal DiseaseDocument38 pagesNeonatal Renal Diseasesaieefzaman71No ratings yet
- Preoperative & Postoperative EvaluationDocument61 pagesPreoperative & Postoperative EvaluationSonntagsschule St. Antonius Kloster in KröffelbachNo ratings yet
- Pediatric NursingDocument105 pagesPediatric NursingPaida P. Abdulmalik75% (4)
- Pyloric StenosisDocument47 pagesPyloric StenosisgeethsreesatNo ratings yet
- Congenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalDocument17 pagesCongenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalChamika HuruggamuwaNo ratings yet
- Midterms-NCM-109-Pedia-Lec-Dean (Repaired)Document28 pagesMidterms-NCM-109-Pedia-Lec-Dean (Repaired)Drannel FajardoNo ratings yet
- Approach To Preterm BabyDocument28 pagesApproach To Preterm BabyMUHAMMAD DANIAL BIN HASAN FPSKNo ratings yet
- Common Neonatal DisordersDocument71 pagesCommon Neonatal DisordersRANJIT GOGOI100% (3)
- Resuscitation in PregnancyDocument24 pagesResuscitation in PregnancyHassan Al SinanNo ratings yet
- Duodenal Obstruction: Dr. Mochamad Reza FebrianDocument24 pagesDuodenal Obstruction: Dr. Mochamad Reza FebrianBoby ChandraNo ratings yet
- Anesthesia-in-fetoscopic-surgeriesDocument25 pagesAnesthesia-in-fetoscopic-surgeriesSathya PrabuNo ratings yet
- Neonatal SepsisDocument65 pagesNeonatal SepsisRomMy WiEn MicKhoNo ratings yet
- Respiratory DiseasesDocument58 pagesRespiratory DiseasesSarahNo ratings yet
- Respiratory Distress of The NewbornDocument66 pagesRespiratory Distress of The NewbornErik Catos LawijayaNo ratings yet
- Extremely LBW PRETERM Case PresentationDocument41 pagesExtremely LBW PRETERM Case PresentationShami PokhrelNo ratings yet
- Emergency Obstetrics2Document105 pagesEmergency Obstetrics2Alphine DalgoNo ratings yet
- 19 Nursing Care of A Child With Life Threatening ConditionsDocument31 pages19 Nursing Care of A Child With Life Threatening ConditionsBea Bianca CruzNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Asfiksia PerinatalDocument63 pagesAsfiksia PerinatalrantiadrianiNo ratings yet
- Neonatal PhysiologyDocument65 pagesNeonatal Physiologyunknownsince1986No ratings yet
- Neonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDocument10 pagesNeonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDr. Anish GolchhaNo ratings yet
- Special Neonatal ConditionsDocument37 pagesSpecial Neonatal ConditionsSanthosh.S.UNo ratings yet
- Necrotizing Enterocolitis: Janice Nicklay Catalan M.DDocument27 pagesNecrotizing Enterocolitis: Janice Nicklay Catalan M.DrianurjanahNo ratings yet
- Common Congenital Git Malformations FinDocument60 pagesCommon Congenital Git Malformations FinRuth DanielNo ratings yet
- Common Neonatal Conditions - Supplementary MaterialDocument25 pagesCommon Neonatal Conditions - Supplementary MaterialayunisallehNo ratings yet
- Acute Abdomen in PaediatricsDocument80 pagesAcute Abdomen in PaediatricsDaniel RajNo ratings yet
- High Risk NewbornDocument83 pagesHigh Risk Newbornbautil.jameelNo ratings yet
- Pediatric Surgery Day 1Document267 pagesPediatric Surgery Day 1ironbuangNo ratings yet
- High Risk Newborn - Study GuideDocument10 pagesHigh Risk Newborn - Study GuideMalou Yap Buot100% (1)
- Problems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightDocument88 pagesProblems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightNikky SilvestreNo ratings yet
- Postmature Infants 1Document13 pagesPostmature Infants 1LyssaMarieKathryneEge100% (1)
- Hirschsprung DiseaseDocument20 pagesHirschsprung DiseaseIvy DanNo ratings yet
- Fatur Reyhan MuradiDocument15 pagesFatur Reyhan MuradiFatur ReyhanNo ratings yet
- Pediatric Surgery Dr. A. IgamaDocument6 pagesPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNo ratings yet
- Lec 1Document52 pagesLec 1zainabd1964No ratings yet
- Pediatric Surgical ThemesDocument32 pagesPediatric Surgical ThemesDabessa MosissaNo ratings yet
- Pediatric SurgeryDocument60 pagesPediatric SurgeryAbdalla SamatarNo ratings yet
- Gynae EmerganciesDocument39 pagesGynae EmerganciesgibreilNo ratings yet
- GI DisordersDocument80 pagesGI DisordersjoycechicagoNo ratings yet
- Pyloric Stenosis Case StudyDocument37 pagesPyloric Stenosis Case StudyFaith Torralba100% (3)
- High Risk PediatricsDocument207 pagesHigh Risk Pediatricsruby cubionaNo ratings yet
- Genitourinary Alterations in Chldren: Heather BuccelloDocument46 pagesGenitourinary Alterations in Chldren: Heather BuccelloshanikaNo ratings yet
- 2.hypertrophic Pyloric StenosisDocument43 pages2.hypertrophic Pyloric Stenosischivorn.ch123No ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Phychem 2 - Lab Report 2Document9 pagesPhychem 2 - Lab Report 2Ralph EvidenteNo ratings yet
- PCC Communities / Community Education Schedule - Summer 09Document64 pagesPCC Communities / Community Education Schedule - Summer 09portlandccNo ratings yet
- Tickler Final PDFDocument29 pagesTickler Final PDFSerious LeoNo ratings yet
- Jawaban Pma 1-100Document4 pagesJawaban Pma 1-100Agung KurniawanNo ratings yet
- ENG201 Mid Term Past Paper 2Document6 pagesENG201 Mid Term Past Paper 2malik100% (1)
- Spec Merlin Gerin MCCBDocument85 pagesSpec Merlin Gerin MCCBTen ApolinarioNo ratings yet
- Erasmus Presentation - 27 AbrilDocument11 pagesErasmus Presentation - 27 AbrilPaulo TavaresNo ratings yet
- (CSE3083) Lab Practical Assignment #7 (Updated)Document8 pages(CSE3083) Lab Practical Assignment #7 (Updated)Karan SikarwarNo ratings yet
- Syllabus Debate PDFDocument5 pagesSyllabus Debate PDFJeicel Ann BarairoNo ratings yet
- Module 2-English Worksheet-SourcesDocument2 pagesModule 2-English Worksheet-SourcesMarife GuadalupeNo ratings yet
- Gilmore (1960) A Proof Method For Quantification TheoryDocument8 pagesGilmore (1960) A Proof Method For Quantification TheoryLógica UsbNo ratings yet
- VijayawadaDocument62 pagesVijayawadakeerthiNo ratings yet
- Mel 5Document9 pagesMel 5Yhan SombilonNo ratings yet
- 11 - PC8000 - 6 ApplDocument37 pages11 - PC8000 - 6 Appljhon jairo trujillo100% (1)
- Causation Syllabus 2016Document4 pagesCausation Syllabus 2016Hana CurcicNo ratings yet
- People v. RiveraDocument36 pagesPeople v. RiveraAemel de LeonNo ratings yet
- MH. Mh. MH.: Septic Tank PlanDocument1 pageMH. Mh. MH.: Septic Tank PlanBess Adrane JurolanNo ratings yet
- Year 12 MockDocument5 pagesYear 12 MockAlvan MmaduwubaNo ratings yet
- SLP Unisa 2014 All CollegesDocument324 pagesSLP Unisa 2014 All CollegesWerner LouwNo ratings yet
- DVD Stereo System SC-VKX60: Operating InstructionsDocument27 pagesDVD Stereo System SC-VKX60: Operating InstructionsSeb FacuNo ratings yet
- Dinesh Khattar - Quantitative Aptitude For Campus Interview Vol II-Pearson Education (2016)Document434 pagesDinesh Khattar - Quantitative Aptitude For Campus Interview Vol II-Pearson Education (2016)Rough Work100% (1)
- Does The Media Impact Athletic PerformanceDocument2 pagesDoes The Media Impact Athletic PerformanceVaishnavi SinghNo ratings yet
- Coolnomixac 1Document2 pagesCoolnomixac 1Eko AdiNo ratings yet
- English 8 Q2M3Document5 pagesEnglish 8 Q2M3Mark Jhoriz VillafuerteNo ratings yet
- Prevention of Sexual Harassment at WorkplaceDocument62 pagesPrevention of Sexual Harassment at WorkplaceNitesh kumar singhNo ratings yet
- Q1. Choose The Correct Answer. 1X50 50Document7 pagesQ1. Choose The Correct Answer. 1X50 50Muhammad RizwanNo ratings yet
- Motherboard Asus X99 DeluxeDocument10 pagesMotherboard Asus X99 DeluxeAlexandar ŠkaraNo ratings yet
- 100 Questions On Water Biochemistry-1Document19 pages100 Questions On Water Biochemistry-1CnokelvinNo ratings yet
- Soundwel AE Product CatalogueDocument18 pagesSoundwel AE Product CatalogueHenry CruzNo ratings yet
- Miley Ped - RadiologyDocument52 pagesMiley Ped - RadiologyLukasNo ratings yet




















































































Download as pptx, pdf, or txt
You might also like
- Case Presentation On Neonatal Sepsis: BY-Anisha ManeDocument45 pagesCase Presentation On Neonatal Sepsis: BY-Anisha ManeAnisha Mane100% (5)
- Neonatal AnaesthesiaDocument61 pagesNeonatal AnaesthesianeneknoraNo ratings yet
- Classification of Newborn, - 130319150346Document45 pagesClassification of Newborn, - 130319150346Ez Ball100% (1)
- Special Considerations in The Premature and Ex-Premature InfantDocument30 pagesSpecial Considerations in The Premature and Ex-Premature InfanteryxspNo ratings yet
- Pediatric SurgeryDocument57 pagesPediatric SurgeryMusekhirNo ratings yet
- Congenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonDocument21 pagesCongenital Diaphragmatic Hernia: DR Feeroz Alam Khan Pediatric SurgeonPrabhat GuptaNo ratings yet
- Common Newborn Problems (2) C1Document39 pagesCommon Newborn Problems (2) C1ZmNo ratings yet
- PREMATURITYDocument27 pagesPREMATURITYHamizi MD HanapiahNo ratings yet
- Assessment and Management of High Risk Neonates DrLawHN PDFDocument45 pagesAssessment and Management of High Risk Neonates DrLawHN PDFShiva KarthikeyanNo ratings yet
- 10 Newborn1Document129 pages10 Newborn1Gerlian Kyle QueridoNo ratings yet
- Preterm Its ProblemsDocument30 pagesPreterm Its ProblemsEnlighten usNo ratings yet
- Pediatric AnesthesiaDocument70 pagesPediatric AnesthesiaEliyan KhanimovNo ratings yet
- Respiratory Distress SyndromeDocument41 pagesRespiratory Distress Syndromef.abrahamNo ratings yet
- 6.1 High Risk New Born-1Document76 pages6.1 High Risk New Born-1ArbzNo ratings yet
- Birth AsphyxiaDocument12 pagesBirth Asphyxiaannu panchalNo ratings yet
- Neonatal Renal DiseaseDocument38 pagesNeonatal Renal Diseasesaieefzaman71No ratings yet
- Preoperative & Postoperative EvaluationDocument61 pagesPreoperative & Postoperative EvaluationSonntagsschule St. Antonius Kloster in KröffelbachNo ratings yet
- Pediatric NursingDocument105 pagesPediatric NursingPaida P. Abdulmalik75% (4)
- Pyloric StenosisDocument47 pagesPyloric StenosisgeethsreesatNo ratings yet
- Congenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalDocument17 pagesCongenital Hypertrophic Pyloric Stenosis: Dr. Kundan Department of Surgery Patna Medical College & HospitalChamika HuruggamuwaNo ratings yet
- Midterms-NCM-109-Pedia-Lec-Dean (Repaired)Document28 pagesMidterms-NCM-109-Pedia-Lec-Dean (Repaired)Drannel FajardoNo ratings yet
- Approach To Preterm BabyDocument28 pagesApproach To Preterm BabyMUHAMMAD DANIAL BIN HASAN FPSKNo ratings yet
- Common Neonatal DisordersDocument71 pagesCommon Neonatal DisordersRANJIT GOGOI100% (3)
- Resuscitation in PregnancyDocument24 pagesResuscitation in PregnancyHassan Al SinanNo ratings yet
- Duodenal Obstruction: Dr. Mochamad Reza FebrianDocument24 pagesDuodenal Obstruction: Dr. Mochamad Reza FebrianBoby ChandraNo ratings yet
- Anesthesia-in-fetoscopic-surgeriesDocument25 pagesAnesthesia-in-fetoscopic-surgeriesSathya PrabuNo ratings yet
- Neonatal SepsisDocument65 pagesNeonatal SepsisRomMy WiEn MicKhoNo ratings yet
- Respiratory DiseasesDocument58 pagesRespiratory DiseasesSarahNo ratings yet
- Respiratory Distress of The NewbornDocument66 pagesRespiratory Distress of The NewbornErik Catos LawijayaNo ratings yet
- Extremely LBW PRETERM Case PresentationDocument41 pagesExtremely LBW PRETERM Case PresentationShami PokhrelNo ratings yet
- Emergency Obstetrics2Document105 pagesEmergency Obstetrics2Alphine DalgoNo ratings yet
- 19 Nursing Care of A Child With Life Threatening ConditionsDocument31 pages19 Nursing Care of A Child With Life Threatening ConditionsBea Bianca CruzNo ratings yet
- Hirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshDocument48 pagesHirschsprun G'S Disease: Dr. Manish Kumar Gupta Assistant Professor Department of Paediatric Surgery AIIMS, RishikeshArchana Mahata100% (1)
- Asfiksia PerinatalDocument63 pagesAsfiksia PerinatalrantiadrianiNo ratings yet
- Neonatal PhysiologyDocument65 pagesNeonatal Physiologyunknownsince1986No ratings yet
- Neonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDocument10 pagesNeonatal Anaesthesia 2 Anaesthesia For Neonates With Abdominal Wall DefectsDr. Anish GolchhaNo ratings yet
- Special Neonatal ConditionsDocument37 pagesSpecial Neonatal ConditionsSanthosh.S.UNo ratings yet
- Necrotizing Enterocolitis: Janice Nicklay Catalan M.DDocument27 pagesNecrotizing Enterocolitis: Janice Nicklay Catalan M.DrianurjanahNo ratings yet
- Common Congenital Git Malformations FinDocument60 pagesCommon Congenital Git Malformations FinRuth DanielNo ratings yet
- Common Neonatal Conditions - Supplementary MaterialDocument25 pagesCommon Neonatal Conditions - Supplementary MaterialayunisallehNo ratings yet
- Acute Abdomen in PaediatricsDocument80 pagesAcute Abdomen in PaediatricsDaniel RajNo ratings yet
- High Risk NewbornDocument83 pagesHigh Risk Newbornbautil.jameelNo ratings yet
- Pediatric Surgery Day 1Document267 pagesPediatric Surgery Day 1ironbuangNo ratings yet
- High Risk Newborn - Study GuideDocument10 pagesHigh Risk Newborn - Study GuideMalou Yap Buot100% (1)
- Problems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightDocument88 pagesProblems Related To Prematurity, Post Maturity, Problems Related To Gestational WeightNikky SilvestreNo ratings yet
- Postmature Infants 1Document13 pagesPostmature Infants 1LyssaMarieKathryneEge100% (1)
- Hirschsprung DiseaseDocument20 pagesHirschsprung DiseaseIvy DanNo ratings yet
- Fatur Reyhan MuradiDocument15 pagesFatur Reyhan MuradiFatur ReyhanNo ratings yet
- Pediatric Surgery Dr. A. IgamaDocument6 pagesPediatric Surgery Dr. A. IgamaMarco Paulo Reyes NaoeNo ratings yet
- Lec 1Document52 pagesLec 1zainabd1964No ratings yet
- Pediatric Surgical ThemesDocument32 pagesPediatric Surgical ThemesDabessa MosissaNo ratings yet
- Pediatric SurgeryDocument60 pagesPediatric SurgeryAbdalla SamatarNo ratings yet
- Gynae EmerganciesDocument39 pagesGynae EmerganciesgibreilNo ratings yet
- GI DisordersDocument80 pagesGI DisordersjoycechicagoNo ratings yet
- Pyloric Stenosis Case StudyDocument37 pagesPyloric Stenosis Case StudyFaith Torralba100% (3)
- High Risk PediatricsDocument207 pagesHigh Risk Pediatricsruby cubionaNo ratings yet
- Genitourinary Alterations in Chldren: Heather BuccelloDocument46 pagesGenitourinary Alterations in Chldren: Heather BuccelloshanikaNo ratings yet
- 2.hypertrophic Pyloric StenosisDocument43 pages2.hypertrophic Pyloric Stenosischivorn.ch123No ratings yet
- Dysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsFrom EverandDysphagia, A Simple Guide To The Condition, Treatment And Related ConditionsRating: 5 out of 5 stars5/5 (1)
- Phychem 2 - Lab Report 2Document9 pagesPhychem 2 - Lab Report 2Ralph EvidenteNo ratings yet
- PCC Communities / Community Education Schedule - Summer 09Document64 pagesPCC Communities / Community Education Schedule - Summer 09portlandccNo ratings yet
- Tickler Final PDFDocument29 pagesTickler Final PDFSerious LeoNo ratings yet
- Jawaban Pma 1-100Document4 pagesJawaban Pma 1-100Agung KurniawanNo ratings yet
- ENG201 Mid Term Past Paper 2Document6 pagesENG201 Mid Term Past Paper 2malik100% (1)
- Spec Merlin Gerin MCCBDocument85 pagesSpec Merlin Gerin MCCBTen ApolinarioNo ratings yet
- Erasmus Presentation - 27 AbrilDocument11 pagesErasmus Presentation - 27 AbrilPaulo TavaresNo ratings yet
- (CSE3083) Lab Practical Assignment #7 (Updated)Document8 pages(CSE3083) Lab Practical Assignment #7 (Updated)Karan SikarwarNo ratings yet
- Syllabus Debate PDFDocument5 pagesSyllabus Debate PDFJeicel Ann BarairoNo ratings yet
- Module 2-English Worksheet-SourcesDocument2 pagesModule 2-English Worksheet-SourcesMarife GuadalupeNo ratings yet
- Gilmore (1960) A Proof Method For Quantification TheoryDocument8 pagesGilmore (1960) A Proof Method For Quantification TheoryLógica UsbNo ratings yet
- VijayawadaDocument62 pagesVijayawadakeerthiNo ratings yet
- Mel 5Document9 pagesMel 5Yhan SombilonNo ratings yet
- 11 - PC8000 - 6 ApplDocument37 pages11 - PC8000 - 6 Appljhon jairo trujillo100% (1)
- Causation Syllabus 2016Document4 pagesCausation Syllabus 2016Hana CurcicNo ratings yet
- People v. RiveraDocument36 pagesPeople v. RiveraAemel de LeonNo ratings yet
- MH. Mh. MH.: Septic Tank PlanDocument1 pageMH. Mh. MH.: Septic Tank PlanBess Adrane JurolanNo ratings yet
- Year 12 MockDocument5 pagesYear 12 MockAlvan MmaduwubaNo ratings yet
- SLP Unisa 2014 All CollegesDocument324 pagesSLP Unisa 2014 All CollegesWerner LouwNo ratings yet
- DVD Stereo System SC-VKX60: Operating InstructionsDocument27 pagesDVD Stereo System SC-VKX60: Operating InstructionsSeb FacuNo ratings yet
- Dinesh Khattar - Quantitative Aptitude For Campus Interview Vol II-Pearson Education (2016)Document434 pagesDinesh Khattar - Quantitative Aptitude For Campus Interview Vol II-Pearson Education (2016)Rough Work100% (1)
- Does The Media Impact Athletic PerformanceDocument2 pagesDoes The Media Impact Athletic PerformanceVaishnavi SinghNo ratings yet
- Coolnomixac 1Document2 pagesCoolnomixac 1Eko AdiNo ratings yet
- English 8 Q2M3Document5 pagesEnglish 8 Q2M3Mark Jhoriz VillafuerteNo ratings yet
- Prevention of Sexual Harassment at WorkplaceDocument62 pagesPrevention of Sexual Harassment at WorkplaceNitesh kumar singhNo ratings yet
- Q1. Choose The Correct Answer. 1X50 50Document7 pagesQ1. Choose The Correct Answer. 1X50 50Muhammad RizwanNo ratings yet
- Motherboard Asus X99 DeluxeDocument10 pagesMotherboard Asus X99 DeluxeAlexandar ŠkaraNo ratings yet
- 100 Questions On Water Biochemistry-1Document19 pages100 Questions On Water Biochemistry-1CnokelvinNo ratings yet
- Soundwel AE Product CatalogueDocument18 pagesSoundwel AE Product CatalogueHenry CruzNo ratings yet
- Miley Ped - RadiologyDocument52 pagesMiley Ped - RadiologyLukasNo ratings yet