Download as ppt, pdf, or txt
You might also like
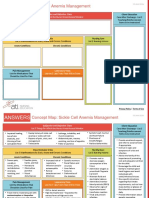
- NCC-SickleCellAnemiaManagement ConceptMap InteractivePDFDocument2 pagesNCC-SickleCellAnemiaManagement ConceptMap InteractivePDFLoggerz Arck100% (1)
- Diagnosa Banding Gangguan SomatisasiDocument3 pagesDiagnosa Banding Gangguan SomatisasiNena_mileyNo ratings yet
- Anxiety DisordersDocument45 pagesAnxiety DisordersAileen A. Monares100% (1)
- Anxiety DisordersDocument40 pagesAnxiety Disordersamal abdulrahmanNo ratings yet
- Psychiatry Lesson 1Document50 pagesPsychiatry Lesson 1chiyumbabeatriceNo ratings yet
- Panic & Bipolar Affective Disorders: Group 1Document33 pagesPanic & Bipolar Affective Disorders: Group 1AYO NELSONNo ratings yet
- Anxietydisorder LectureDocument37 pagesAnxietydisorder LecturesundariNo ratings yet
- Anxiety Disorders 2Document30 pagesAnxiety Disorders 2João Marco Rodrigues SantanaNo ratings yet
- Anxietydisorder LectureDocument37 pagesAnxietydisorder Lecturetazam94No ratings yet
- Anxiety DisordersDocument3 pagesAnxiety DisordersCamille Joy BaliliNo ratings yet
- Health and AnxietyDocument28 pagesHealth and AnxietyAmantle DutaNo ratings yet
- 01 Session 05 Anxiety and FearDocument62 pages01 Session 05 Anxiety and FearMalakatete Mwaipojele-fNo ratings yet
- Mental Health CH 2Document6 pagesMental Health CH 2Gina GiammalvoNo ratings yet
- Anxiety DisordersDocument116 pagesAnxiety DisordersusamanurahmedNo ratings yet
- General Psychology Chapter 7 SummerizedDocument38 pagesGeneral Psychology Chapter 7 Summerizedadisu defarNo ratings yet
- Anxiety DisordersDocument35 pagesAnxiety DisordersmulugetaNo ratings yet
- Anxiety DisordersDocument30 pagesAnxiety DisordersAbelNo ratings yet
- Anxiety DisordersDocument24 pagesAnxiety DisordersSusan MaglaquiNo ratings yet
- Anxiety DisordersDocument44 pagesAnxiety DisordersmanideepreddyNo ratings yet
- 7-Anxiety DisordersDocument26 pages7-Anxiety DisordersZ26No ratings yet
- Mental Health Chapter 1Document36 pagesMental Health Chapter 1Tarek QawasmehNo ratings yet
- Chapter 5 Anxiety Trauma and Stressor Related and Obsessive Compulsive and Related DisorderDocument43 pagesChapter 5 Anxiety Trauma and Stressor Related and Obsessive Compulsive and Related DisorderGabriel Jeremy OrtegaNo ratings yet
- Anxiety and Anxiety DisordersDocument34 pagesAnxiety and Anxiety Disordersshellacayetano2No ratings yet
- Chapter 4Document23 pagesChapter 4Eimun PurtiNo ratings yet
- Anxiety DisordersDocument70 pagesAnxiety DisordersNishantYadav100% (1)
- Anxiety Disorders Lesson PlanDocument32 pagesAnxiety Disorders Lesson PlanPedrosa NardNo ratings yet
- Psyc1002lecturetextbooknotes AbnormalpsychologyDocument5 pagesPsyc1002lecturetextbooknotes Abnormalpsychologypreeti vermaNo ratings yet
- ANXIETYDocument8 pagesANXIETYKimberly SungaNo ratings yet
- Anxiety DisorderDocument11 pagesAnxiety DisorderBiswas AruNo ratings yet
- Introduction To Mental HealthDocument36 pagesIntroduction To Mental HealthXo Yem100% (2)
- 1 Introduction To Psych NursingDocument41 pages1 Introduction To Psych NursingSamer TarekNo ratings yet
- Mental HealthDocument96 pagesMental HealthTinaHo100% (4)
- Intro Mental Health PrepDocument32 pagesIntro Mental Health PrepCarlos PampolinaNo ratings yet
- Diagnosis of Mental IllnessDocument66 pagesDiagnosis of Mental IllnessJorn Arvi ReyesNo ratings yet
- Chapter 14Document54 pagesChapter 14muhibNo ratings yet
- Practical 2 3P1Document16 pagesPractical 2 3P1Kz ZaidiNo ratings yet
- Anxiety Chapter EditedDocument19 pagesAnxiety Chapter EditedamarnehNo ratings yet
- Anxiety Disorders Lesson PlanDocument32 pagesAnxiety Disorders Lesson Planapi-284104206No ratings yet
- Chapter 13: Anxiety, Anxiety Disorders, and Stress-Related IllnessDocument38 pagesChapter 13: Anxiety, Anxiety Disorders, and Stress-Related IllnessHershey Cordero BrionesNo ratings yet
- P$y C@$3 3Document11 pagesP$y C@$3 3Linds GoNo ratings yet
- PSY1011 - Psychological Disorders LectureDocument61 pagesPSY1011 - Psychological Disorders LectureeeNo ratings yet
- Chapter 5 Anxiety, Trauma and Stressor - Related, Obsessive Compulsive Related DisordersDocument16 pagesChapter 5 Anxiety, Trauma and Stressor - Related, Obsessive Compulsive Related DisordersAnnie SumacotNo ratings yet
- AngerDocument17 pagesAngerAamir Faiz100% (1)
- Mental Disorder: Psychological (Or Mental) DisordersDocument7 pagesMental Disorder: Psychological (Or Mental) DisordersEsha MeherNo ratings yet
- Chapter 4: Anxiety Disorders: Nature of Anxiety and FearDocument6 pagesChapter 4: Anxiety Disorders: Nature of Anxiety and FearIvaNova IvelinaNo ratings yet
- AnxietyDocument36 pagesAnxietyRobert RevillasNo ratings yet
- 6anxiety DisordersDocument40 pages6anxiety Disorderswwamed18No ratings yet
- Specific and Social Phobias OCDDocument19 pagesSpecific and Social Phobias OCDBryan Paul RamirezNo ratings yet
- PSY 112-Psychological Disorders IDocument55 pagesPSY 112-Psychological Disorders Ithivyaashini SellaNo ratings yet
- Ap Unit 4Document21 pagesAp Unit 4Vaishnavi RaveendranNo ratings yet
- Anxious Patient Amended 21.2.2011Document122 pagesAnxious Patient Amended 21.2.2011Yogesh Malam100% (1)
- Anxiety DisordersDocument4 pagesAnxiety DisordersCamille Joy BaliliNo ratings yet
- Health Assessment Midterm Exam ReviewerDocument25 pagesHealth Assessment Midterm Exam ReviewerJanna Niña ElementoNo ratings yet
- Anxiety DisordersDocument29 pagesAnxiety DisordersAli Raza GillNo ratings yet
- Trauma - and Stressor-Related DisordersDocument34 pagesTrauma - and Stressor-Related DisordersjenNo ratings yet
- U4L1 Student GuideDocument6 pagesU4L1 Student Guide-Esha-No ratings yet
- Disorder NotesDocument166 pagesDisorder NotesYasirali1999gmail.com YasiraliNo ratings yet
- AnxietyDocument55 pagesAnxietyAbelNo ratings yet
- Unraveling Anxiety: A Comprehensive Guide to Understanding and Overcoming AnxietyFrom EverandUnraveling Anxiety: A Comprehensive Guide to Understanding and Overcoming AnxietyNo ratings yet
- "Unraveling the Knot: Understanding and Overcoming Anxiety and Phobias"From Everand"Unraveling the Knot: Understanding and Overcoming Anxiety and Phobias"No ratings yet
- New York State Mandatory Training: Infection ControlDocument52 pagesNew York State Mandatory Training: Infection ControlLoggerz ArckNo ratings yet
- 2008 05 07 140531shadrina - TahilDocument91 pages2008 05 07 140531shadrina - TahilLoggerz ArckNo ratings yet
- Paper 16Document11 pagesPaper 16Loggerz ArckNo ratings yet
- Sensation AND PerceptionDocument24 pagesSensation AND PerceptionLoggerz ArckNo ratings yet
- Faculty Development ProgramDocument1 pageFaculty Development ProgramLoggerz ArckNo ratings yet
- Preventing Infections Related To Use of Intravascular DevicesDocument16 pagesPreventing Infections Related To Use of Intravascular DevicesLoggerz ArckNo ratings yet
- Lecture Notes For Mental Health Nursing Psych NursingDocument88 pagesLecture Notes For Mental Health Nursing Psych Nursingjg369097100% (1)
- Concepts of Neonatal Care: Reported By: Genevieve Manrique R.NDocument18 pagesConcepts of Neonatal Care: Reported By: Genevieve Manrique R.NLoggerz ArckNo ratings yet
- Lewis: Medical-Surgical Nursing, 10 Edition: Sleep and Sleep Disorders Key Points SleepDocument4 pagesLewis: Medical-Surgical Nursing, 10 Edition: Sleep and Sleep Disorders Key Points Sleepsophia onu100% (2)
- Fmed 07 571154Document13 pagesFmed 07 571154Mita AdrianiNo ratings yet
- Problem List Med WardDocument5 pagesProblem List Med WardJoshNo ratings yet
- Cap. Delirium - Bradley's Neurology in Clinical PracticDocument11 pagesCap. Delirium - Bradley's Neurology in Clinical PracticArthur André RegovichiNo ratings yet
- Impaired Mood - NCPDocument2 pagesImpaired Mood - NCPIsaac papicaNo ratings yet
- PsychiatryDocument19 pagesPsychiatryAnet Augustine AnetNo ratings yet
- A Case of Psychotic Disorder Due To Dengue FeverDocument4 pagesA Case of Psychotic Disorder Due To Dengue FeverHoney SarmientoNo ratings yet
- Schizophrenia: Ms. Jaital Rathod (B.Sc. Nursing)Document11 pagesSchizophrenia: Ms. Jaital Rathod (B.Sc. Nursing)jaital rathodNo ratings yet
- Communication Disorders: SymptomsDocument3 pagesCommunication Disorders: SymptomsNoor Ul Hudda MemonNo ratings yet
- Foreign-Body Airway ObstructionDocument17 pagesForeign-Body Airway ObstructionDessy Christiani Part IINo ratings yet
- Countr State: KatsinaDocument9 pagesCountr State: KatsinaSalihu MustaphaNo ratings yet
- Undifferentiated SchizophreniaDocument7 pagesUndifferentiated SchizophreniaVincent GarciaNo ratings yet
- The Relationship Between Attention Deficit Hyperactivity Hassan AEH 2015Document7 pagesThe Relationship Between Attention Deficit Hyperactivity Hassan AEH 2015al_dhi_01No ratings yet
- PEC11 Chap 19 Seizures and SyncopeDocument55 pagesPEC11 Chap 19 Seizures and SyncopeRyanNo ratings yet
- Final-OPIDO (SN) - BSN 407 - CPRDocument1 pageFinal-OPIDO (SN) - BSN 407 - CPRrodolfo opidoNo ratings yet
- WHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureDocument3 pagesWHO List of Conditions Treated by Acupuncture - Healthy Family AcupunctureSreekanth KrishnamurthyNo ratings yet
- Good Ideas Ver 2Document2 pagesGood Ideas Ver 2testNo ratings yet
- Metabolic EncephalopathyDocument22 pagesMetabolic Encephalopathytricia isabellaNo ratings yet
- Web Quiz Somatoform and Dissociative Disorders Chapter 6Document4 pagesWeb Quiz Somatoform and Dissociative Disorders Chapter 6IvaNova IvelinaNo ratings yet
- Drug Study HaloperidolDocument3 pagesDrug Study HaloperidolKrizzia FosterNo ratings yet
- Maya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewDocument18 pagesMaya Semrau - Service User and Caregiver Involvement in Mental Health System Strengthening in Low - and Middle-Income Countries Systematic ReviewsukmarahastriNo ratings yet
- Antepartum & Postpartum Hemorrhage (APH &PPH) : Basim Abu-RafeaDocument81 pagesAntepartum & Postpartum Hemorrhage (APH &PPH) : Basim Abu-RafeaSheilla ElfiraNo ratings yet
- BMJ 334 7593 CR 00579Document10 pagesBMJ 334 7593 CR 00579RonaMaulidiaBakhitaNo ratings yet
- Psych History StudyHub GuideDocument14 pagesPsych History StudyHub GuideAboubakar Moalim Mahad moh'dNo ratings yet
- 4 5814470955174463831Document45 pages4 5814470955174463831random personsaNo ratings yet
- Treatment of PTSD and Comorbid Disorders: DescriptionDocument8 pagesTreatment of PTSD and Comorbid Disorders: DescriptionMelly T CiakraNo ratings yet
- Risk For Deficient Fluid VolumeDocument2 pagesRisk For Deficient Fluid VolumeMariella BadongenNo ratings yet
- Cannabis Psychosis Fact Sheet PDFDocument1 pageCannabis Psychosis Fact Sheet PDFricardo_balau8081No ratings yet
- Strategies For Managing Impairing Emotional OutburstsDocument2 pagesStrategies For Managing Impairing Emotional OutburstsAndreia RossiNo ratings yet