Download as pptx, pdf, or txt
You might also like
- Charge Nurse WorksheetDocument1 pageCharge Nurse WorksheetFitz JaminitNo ratings yet
- Allergy Test ResultDocument10 pagesAllergy Test ResultBabukutty JacobNo ratings yet
- Imunnology CaseDocument20 pagesImunnology CaseRichard AriezkiNo ratings yet
- Fundamentals of Hair Coloring and Hair BleachingDocument18 pagesFundamentals of Hair Coloring and Hair BleachingBeatriz100% (9)
- Contact Dermatitis Concept MapDocument1 pageContact Dermatitis Concept MapAlexeve TabalNo ratings yet
- MainDocument15 pagesMainArini HikmahNo ratings yet
- Rhinitis: Sheryl BeardDocument14 pagesRhinitis: Sheryl BeardJohar TajudinNo ratings yet
- Patogenesis de La RinitisDocument39 pagesPatogenesis de La Rinitiskriss krammNo ratings yet
- Material To Read AlergologyDocument6 pagesMaterial To Read AlergologyLeo PaulNo ratings yet
- Allergic Rhinitis (AKBAR)Document5 pagesAllergic Rhinitis (AKBAR)Roni PahlawanNo ratings yet
- Allergic RhinitisDocument27 pagesAllergic RhinitisArvindhanNo ratings yet
- Allergic Rhinitis in ChildhoodDocument67 pagesAllergic Rhinitis in Childhoodmp1a1234No ratings yet
- Henry Milgrom Donald Y.M. Leung: Chapter 142 - Allergic RhinitisDocument11 pagesHenry Milgrom Donald Y.M. Leung: Chapter 142 - Allergic RhinitisSara Velásquez JNo ratings yet
- Allergic RhinitisDocument2 pagesAllergic RhinitisJamie IcabandiNo ratings yet
- Book-Based: Pathophysiology of Allergic RhinitisDocument2 pagesBook-Based: Pathophysiology of Allergic RhinitisJeraldine Corpuz PascualNo ratings yet
- Allergic Rhinitis - ClinicalKeyDocument18 pagesAllergic Rhinitis - ClinicalKeykatleenfreylevelasquezNo ratings yet
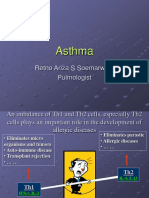
- Asthma: Retno Ariza S Soemarwoto PulmologistDocument18 pagesAsthma: Retno Ariza S Soemarwoto PulmologistImam BaihaqiNo ratings yet
- Seminar On Bronchial Asthma NewDocument42 pagesSeminar On Bronchial Asthma NewShabna SameerNo ratings yet
- AllergyDocument17 pagesAllergyHero TasinNo ratings yet
- International Health Services: AllergyDocument7 pagesInternational Health Services: AllergyIlyes FerenczNo ratings yet
- Bronhial AsthmaDocument63 pagesBronhial AsthmaGreeshma Shaji100% (1)
- ALLERGIESDocument13 pagesALLERGIESpravisankar1978No ratings yet
- Asthma (For RACP Exams)Document18 pagesAsthma (For RACP Exams)Sam HuntNo ratings yet
- Rinitis Alérgica: Anthony Toralva SantillanDocument22 pagesRinitis Alérgica: Anthony Toralva SantillanAnthony Toralva SantillanNo ratings yet
- Pediatri IIDocument25 pagesPediatri IImulNo ratings yet
- Allergic Rhinitis PDFDocument3 pagesAllergic Rhinitis PDFdrbilalmunirNo ratings yet
- Clinic and Diagnostics of House Dust Mite Allergy: Mini-ReviewDocument4 pagesClinic and Diagnostics of House Dust Mite Allergy: Mini-ReviewAnca DragoiNo ratings yet
- Allergic Rhinitis Slides 070926 PDFDocument57 pagesAllergic Rhinitis Slides 070926 PDFmhamad kabraNo ratings yet
- Allergic Rhinitis Is ADocument89 pagesAllergic Rhinitis Is AElena TutunaruNo ratings yet
- Allergy: What Is An Allergy?Document5 pagesAllergy: What Is An Allergy?aravindkkk999No ratings yet
- Presented By: Agamjeet Singh Batra, VI - NDocument27 pagesPresented By: Agamjeet Singh Batra, VI - NlovleshrubyNo ratings yet
- AllergicrhinitisDocument6 pagesAllergicrhinitisNurainiyyah MuhjaNo ratings yet
- Case Study - Allergic RhinitisDocument2 pagesCase Study - Allergic RhinitisBait-it Zennesah CarmelleNo ratings yet
- Atopy and Characteristics of AtopyDocument5 pagesAtopy and Characteristics of Atopyayisha thazyNo ratings yet
- AllergicrhinitisDocument6 pagesAllergicrhinitisMelati RNo ratings yet
- RhinitisDocument7 pagesRhinitisShen ParilNo ratings yet
- Hay FeverDocument5 pagesHay FeverOneCharuNo ratings yet
- Asthma: Retno Ariza S Soemarwoto PulmologistDocument18 pagesAsthma: Retno Ariza S Soemarwoto PulmologistAulidaweli DasrulNo ratings yet
- Allergic Rhinitis in Children: DDR - Yousf AhmedDocument45 pagesAllergic Rhinitis in Children: DDR - Yousf AhmedYousfNo ratings yet
- Allergic Rhinitis in Children: Dr. Yousf AhmedDocument45 pagesAllergic Rhinitis in Children: Dr. Yousf AhmedYousfNo ratings yet
- Shree Krishna Public SchoolDocument21 pagesShree Krishna Public Schoolharishparsai35No ratings yet
- Hipersensitivitas LingkunganDocument32 pagesHipersensitivitas LingkunganRamaNo ratings yet
- Allergic Rhinitis: Review Open AccessDocument8 pagesAllergic Rhinitis: Review Open AccessJuanNo ratings yet
- AsthmaDocument5 pagesAsthmaabenezer isayasNo ratings yet
- Allergic and Non Allergic RhinitisDocument76 pagesAllergic and Non Allergic RhinitisEmaan NoorNo ratings yet
- Allergy and AllergensDocument10 pagesAllergy and AllergensAieyan AsifNo ratings yet
- Allergic RhinitisDocument12 pagesAllergic RhinitisKrizha Maraj Inez ElequinNo ratings yet
- Allergy AutosavedDocument11 pagesAllergy AutosavedLeizel Gabin - MoratallaNo ratings yet
- Case Report RA SENODocument11 pagesCase Report RA SENOAnonymous XFDJfsGviNo ratings yet
- UpToDate Allergic Rhinitis - Clinical Manifestations, Epidemiology, and DiagnosisDocument26 pagesUpToDate Allergic Rhinitis - Clinical Manifestations, Epidemiology, and Diagnosishafidhatul aisyNo ratings yet
- Allergic Rhinitis: PathophysiologyDocument28 pagesAllergic Rhinitis: Pathophysiologysneh1509No ratings yet
- What Is An Allergy?: Clinical Aspects of Allergic DisordersDocument5 pagesWhat Is An Allergy?: Clinical Aspects of Allergic Disordersmaheen akramNo ratings yet
- AllergicDocument18 pagesAllergicChethranNo ratings yet
- Biology Investigatory ProjectDocument21 pagesBiology Investigatory ProjectCrazy about Jungles88% (32)
- Biology Investigatory ProjectDocument19 pagesBiology Investigatory ProjectDebkanti Gupta BhayaNo ratings yet
- RhinitisDocument23 pagesRhinitisDr. T. BalasubramanianNo ratings yet
- Secondary Health 7 q4 Module 1Document13 pagesSecondary Health 7 q4 Module 1FernandoNo ratings yet
- Immune System Allergen: Allergic RhinitisDocument1 pageImmune System Allergen: Allergic RhinitisLuphly TaluvtaNo ratings yet
- 03 Asthma FinalDocument50 pages03 Asthma FinalG SNo ratings yet
- Allergy: Samreen TanveerDocument82 pagesAllergy: Samreen Tanveermehwish qayyum0% (1)
- Allergy 191044034 PHN-313Document12 pagesAllergy 191044034 PHN-313AL ImranNo ratings yet
- Holistic Allergy Management: Self-Care, Diet, and HomeopathyFrom EverandHolistic Allergy Management: Self-Care, Diet, and HomeopathyNo ratings yet
- TrainingDocument44 pagesTrainingMeghanath PandhikondaNo ratings yet
- Case Study 1Document4 pagesCase Study 1Noreen CaballeroNo ratings yet
- IgE II.V9Document4 pagesIgE II.V9Abdullah ZobayerNo ratings yet
- Allergic Disease: Prof. Rusudan Karseladze Iv. Javakhishvili Tbilisi State University Institute of PediatricsDocument144 pagesAllergic Disease: Prof. Rusudan Karseladze Iv. Javakhishvili Tbilisi State University Institute of PediatricspalNo ratings yet
- Web 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyDocument38 pagesWeb 24 - Teti Madiadipoera - Treatment and Management of Rhinitis AllergyEdzhar HasiholanNo ratings yet
- Clustered Knowledge Assessment: Resubmission FeedbackDocument65 pagesClustered Knowledge Assessment: Resubmission FeedbackRaxya BaralNo ratings yet
- Focus3 2E Test Unit6 GroupA 1kolDocument5 pagesFocus3 2E Test Unit6 GroupA 1kolMagdaNo ratings yet
- Work Environment Questionnaire 1Document2 pagesWork Environment Questionnaire 1Tr RoseNo ratings yet
- Allergy Testing: How The Test Is PerformedDocument4 pagesAllergy Testing: How The Test Is PerformedJudianto TanaNo ratings yet
- Anaphylaxis: How To Give AnapenDocument1 pageAnaphylaxis: How To Give AnapenmemeNo ratings yet
- Allergic Contact Dermatitis Caused by PEG 22dodecyl GlycolDocument2 pagesAllergic Contact Dermatitis Caused by PEG 22dodecyl GlycolFreddy RojasNo ratings yet
- Phadiatop Rev 051605Document1 pagePhadiatop Rev 051605Kat Chique BNo ratings yet
- Mouth Throat Nose and Sinuses Assessment FindingsDocument5 pagesMouth Throat Nose and Sinuses Assessment FindingsChris SmithNo ratings yet
- Preparing and Administering Intradermal Injection PurposeDocument10 pagesPreparing and Administering Intradermal Injection PurposeLRBNo ratings yet
- Do Not Copy: Combination Therapy in Allergic Rhinitis: What Works and What Does Not WorkDocument6 pagesDo Not Copy: Combination Therapy in Allergic Rhinitis: What Works and What Does Not WorkZero IDNo ratings yet
- Devolutiva Do Caso Clínico Do Dia 22.09Document10 pagesDevolutiva Do Caso Clínico Do Dia 22.09Luís Fernando TrevisanNo ratings yet
- Cleaning Allergen Polyurethane 1Document128 pagesCleaning Allergen Polyurethane 1Yudhi AdiNo ratings yet
- Sanjeevini Combination Sheet For SSC 2 AllergiesDocument1 pageSanjeevini Combination Sheet For SSC 2 AllergiesEduardoNo ratings yet
- Alergenos Lateral Flow RomerDocument2 pagesAlergenos Lateral Flow RomerStefhany R. DíazNo ratings yet
- Report NaveenDocument3 pagesReport NaveennaveenNo ratings yet
- Anzcor Guideline 9 2 7 Anaphylaxis Aug16Document3 pagesAnzcor Guideline 9 2 7 Anaphylaxis Aug16Md. AlamgirNo ratings yet
- Penguard HB Comp ADocument12 pagesPenguard HB Comp AMuhammad hussainNo ratings yet
- Allergic Rhinitis VASDocument5 pagesAllergic Rhinitis VASxtineNo ratings yet
- Dermatitis KuliahDocument17 pagesDermatitis KuliahFirda LudfiyahNo ratings yet
- Enzyme Potentiated DesensitizationDocument4 pagesEnzyme Potentiated DesensitizationdescataNo ratings yet
- Session 8 Rle - OdquierDocument18 pagesSession 8 Rle - OdquierAndrea Mae OdquierNo ratings yet