Download as pptx, pdf, or txt
You might also like
- Health AssessmentttDocument64 pagesHealth AssessmentttAudreySalvador100% (4)
- 16 Dental ImplantDocument9 pages16 Dental Implantallakami777yousefNo ratings yet
- Indian JDent Res 2018Document8 pagesIndian JDent Res 2018Deepalakshmi VenkatesanNo ratings yet
- BASIC IMPLANT SCIENCES.20.Sabtu, 29 April 2017Document27 pagesBASIC IMPLANT SCIENCES.20.Sabtu, 29 April 2017dehaaNo ratings yet
- G.01 Orthopaedic Implant - Brochure - 06.07.2021 - 4Document1 pageG.01 Orthopaedic Implant - Brochure - 06.07.2021 - 4mostafa adelNo ratings yet
- Jonge2008 OrganicInorganicSurfaceModificDocument13 pagesJonge2008 OrganicInorganicSurfaceModific김산No ratings yet
- Bone Biology & Healing: Maxillofacial RegionDocument28 pagesBone Biology & Healing: Maxillofacial Regionbran makmornNo ratings yet
- Unit 4Document50 pagesUnit 4himanshuprasad2004No ratings yet
- Osseointegration Short Review PDFDocument5 pagesOsseointegration Short Review PDFkryptonites1234No ratings yet
- Tripplett 2003 - Implant Materials and DesignsDocument18 pagesTripplett 2003 - Implant Materials and DesignsZhiyi LinNo ratings yet
- Omi 15 5 Sykara7Document16 pagesOmi 15 5 Sykara7dwinugrohojuandaNo ratings yet
- 2 Somer Albrektsson2016Document10 pages2 Somer Albrektsson2016jeffry Francisco Campusano TorresNo ratings yet
- Bio MaterialsDocument19 pagesBio MaterialserracticNo ratings yet
- Implant BiomaterialsDocument18 pagesImplant BiomaterialsPadma GnanamNo ratings yet
- Nanophase Ceramics: The Future Orthopedic and Dental Implant MaterialDocument42 pagesNanophase Ceramics: The Future Orthopedic and Dental Implant MaterialDario Bejarano RojasNo ratings yet
- Biodegradable Bone Implants in Orthopedic Applications: A ReviewDocument15 pagesBiodegradable Bone Implants in Orthopedic Applications: A ReviewGirish Chandra DewanganNo ratings yet
- Bone Remodeling - Basic Science - OrthobulletsDocument4 pagesBone Remodeling - Basic Science - OrthobulletsCindy Julia AmandaNo ratings yet
- Guided Tissue RegenerationDocument64 pagesGuided Tissue Regenerationshazil.21No ratings yet
- Laser Treatment For Bio MaterialsDocument6 pagesLaser Treatment For Bio MaterialsNandakumar M BasavarajNo ratings yet
- Lec.28 Dental Implants Basic Concepts 1Document72 pagesLec.28 Dental Implants Basic Concepts 1banenkareem18No ratings yet
- Literature Review & Preliminary Findings Qing King' Li's Knights of The Round TableDocument46 pagesLiterature Review & Preliminary Findings Qing King' Li's Knights of The Round Tablehmmh5811588No ratings yet
- Prof. Dr. David Buntoro Drg. MDS. SP-BMKDocument30 pagesProf. Dr. David Buntoro Drg. MDS. SP-BMKDipdha Arum SangoraNo ratings yet
- Bio-Materials in Implants: BY, DR - Siddarth SasDocument33 pagesBio-Materials in Implants: BY, DR - Siddarth SasNagappan Chockalingam100% (1)
- Osseo IntegrationDocument79 pagesOsseo Integrationasha docNo ratings yet
- Biology of Implant Osseointegration: A.F. Mavrogenis, R. Dimitriou, J. Parvizi, G.C. BabisDocument12 pagesBiology of Implant Osseointegration: A.F. Mavrogenis, R. Dimitriou, J. Parvizi, G.C. BabisTalitha NabilaNo ratings yet
- Is Primary Stability A Predictable Parameter For Loading Implant?Document5 pagesIs Primary Stability A Predictable Parameter For Loading Implant?Fernando AmadoNo ratings yet
- Osseointegration of Dental ImplantsDocument164 pagesOsseointegration of Dental ImplantsjubinNo ratings yet
- Bone and Metal An Orthopaedic Perspective On Osseointegration of MetalsDocument15 pagesBone and Metal An Orthopaedic Perspective On Osseointegration of MetalsClaudia UngureanuNo ratings yet
- Luka Ostojić Marija Pejakić Željka Perić Kačarević Marko MatijevićDocument1 pageLuka Ostojić Marija Pejakić Željka Perić Kačarević Marko MatijevićmpejakicNo ratings yet
- Implant MaterialsDocument16 pagesImplant MaterialsNikita Aggarwal100% (1)
- ContentServer Asp-3Document16 pagesContentServer Asp-3Santiago Durango HurtadoNo ratings yet
- Dental Implant SurfacesDocument12 pagesDental Implant Surfacesmi.espaciodental20No ratings yet
- Evolution of Internal Fixation in Long Bone FracturesDocument18 pagesEvolution of Internal Fixation in Long Bone FracturesTraumatologia HEBANo ratings yet
- Bone S U Bstitute Materials and Tissue EngineeringDocument27 pagesBone S U Bstitute Materials and Tissue EngineeringdanielNo ratings yet
- The Clinical Application of A New Synthetic Bone Grafting Material in Oral and Maxillofacial SurgeryDocument5 pagesThe Clinical Application of A New Synthetic Bone Grafting Material in Oral and Maxillofacial SurgeryCloudcynaraaNo ratings yet
- 02 Lec 2Document14 pages02 Lec 2Mursalin SonnetNo ratings yet
- Molecular Control of Bioactivity in Sol-Gel GlassesDocument6 pagesMolecular Control of Bioactivity in Sol-Gel GlassesLcdaora TererelNo ratings yet
- Evolution of The Concepts of Implant Anchorage: Ahmadshams, Negar Ramezani Fatatouei, Mina Safari Saman, Neda Sherafat, SoniaDocument28 pagesEvolution of The Concepts of Implant Anchorage: Ahmadshams, Negar Ramezani Fatatouei, Mina Safari Saman, Neda Sherafat, SoniaGio BaywongNo ratings yet
- Optimization of Stress Distribution of Bone-Implant Interface (BII)Document14 pagesOptimization of Stress Distribution of Bone-Implant Interface (BII)د.محمد مليحةNo ratings yet
- Oseointegracion BuserDocument14 pagesOseointegracion BuserGaby MayaNo ratings yet
- Biomaterials 1Document50 pagesBiomaterials 1Lidia EscutiaNo ratings yet
- BCP BrochureDocument8 pagesBCP BrochuregfragolaNo ratings yet
- RetrieveDocument13 pagesRetrieveBruno MañonNo ratings yet
- Changes in Bone Metabolisim Around Osseointegrated Implants Under LoadingDocument17 pagesChanges in Bone Metabolisim Around Osseointegrated Implants Under LoadingAomChanumpornNo ratings yet
- Adem 201801215Document29 pagesAdem 201801215GUSTAVO LOPEZ MENDOZANo ratings yet
- Effect of Smoking in Dental ImplantsDocument8 pagesEffect of Smoking in Dental ImplantsAshish PandaNo ratings yet
- Me 471-Bio-Engineering / Bio-Medical Topics: Bone: Prepared ByDocument20 pagesMe 471-Bio-Engineering / Bio-Medical Topics: Bone: Prepared ByehteshamalhanifNo ratings yet
- Bridge Plating Kellam-1Document47 pagesBridge Plating Kellam-1BS3091No ratings yet
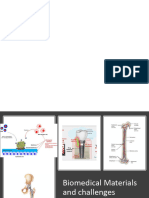
- Implant Surface TreatmemtDocument57 pagesImplant Surface TreatmemtNehal ElsherifNo ratings yet
- 2021-Advances in Implant Surface Modifications To Improve OsseointegrationDocument27 pages2021-Advances in Implant Surface Modifications To Improve Osseointegrationcamilo ortiz intriagoNo ratings yet
- Surface & Coatings Technology: SciencedirectDocument11 pagesSurface & Coatings Technology: SciencedirectYoselin GomezNo ratings yet
- 13.loading of Dental ImplantsDocument166 pages13.loading of Dental ImplantsHarpreet Singh100% (3)
- Bionanotechnology: Nanoengineering For Bionic ImplantsDocument23 pagesBionanotechnology: Nanoengineering For Bionic ImplantsZainab GodhrawalaNo ratings yet
- Trends and Perspectives in Modification of Zirconium Oxide For Dental ProstheticDocument17 pagesTrends and Perspectives in Modification of Zirconium Oxide For Dental Prostheticelbanuswatri1980No ratings yet
- Implanto Chapter 74-78Document104 pagesImplanto Chapter 74-78whatever200020100% (1)
- Classification of Osseointegrated Implant Surfaces: Materials, Chemistry and TopographyDocument9 pagesClassification of Osseointegrated Implant Surfaces: Materials, Chemistry and TopographytheblackalchemistNo ratings yet
- Bisht2021 Article AdvancesInTheFabricationOfScafDocument23 pagesBisht2021 Article AdvancesInTheFabricationOfScafOxy Dental Clinic MakassarNo ratings yet
- Mipo Aplication and Techiniques in Small AnimalsDocument8 pagesMipo Aplication and Techiniques in Small AnimalsmafercaavNo ratings yet
- Implant Micromotion Is Related To Peak Insertion Torque and Bone DensityDocument5 pagesImplant Micromotion Is Related To Peak Insertion Torque and Bone DensityRoja AllampallyNo ratings yet
- Graft ImplantDocument8 pagesGraft ImplantswagataNo ratings yet
- Staphylococci PDFDocument9 pagesStaphylococci PDFGianina YlnNo ratings yet
- Should I Ask My Friends If They AreDocument3 pagesShould I Ask My Friends If They AreMike ReyesNo ratings yet
- PharynxDocument18 pagesPharynxzenith parmarNo ratings yet
- The Functional Anatomy of PhonationDocument15 pagesThe Functional Anatomy of PhonationCarolyn BensonNo ratings yet
- Erik Van Woensel Classical Homeopathy Evidence Based Medicine Vol. 2Document23 pagesErik Van Woensel Classical Homeopathy Evidence Based Medicine Vol. 2Sohail LatifNo ratings yet
- Introduction of The ResearchDocument3 pagesIntroduction of The Researchcristine baldazoNo ratings yet
- Hipocrates - VOLUME 6Document400 pagesHipocrates - VOLUME 6Heitor Murillo CarnioNo ratings yet
- Ranch Management Plan-Darien Holdings PDFDocument12 pagesRanch Management Plan-Darien Holdings PDFKealeboga Duece Thobolo100% (1)
- Aspirin: October 6 University Faculty of PharmacyDocument10 pagesAspirin: October 6 University Faculty of PharmacyMido PopNo ratings yet
- Obsessive - Compulsive and Related Disorders by Dr. Noor AbdulamirDocument25 pagesObsessive - Compulsive and Related Disorders by Dr. Noor Abdulamirاحمد الهاشميNo ratings yet
- Functional FoodsDocument52 pagesFunctional FoodsMade DesmantaNo ratings yet
- ThesisDocument35 pagesThesisMuhdFaris67% (3)
- Inquisitor 3Document12 pagesInquisitor 3Psygnosis Reddevils100% (2)
- Case Study: Tibial FractureDocument45 pagesCase Study: Tibial FractureJM RomiasNo ratings yet
- UntitledDocument337 pagesUntitledGulzar AhmadNo ratings yet
- Villarin - Lesson Plan in DrugsDocument3 pagesVillarin - Lesson Plan in DrugsJeraldine RepolloNo ratings yet
- Resources, Conservation & Recycling: ReviewDocument18 pagesResources, Conservation & Recycling: ReviewIsabellaNo ratings yet
- Competency Appraisal 2Document42 pagesCompetency Appraisal 2Frances Sofia DuranNo ratings yet
- Roxana Flavia Ilies, Andreea CatanaDocument1 pageRoxana Flavia Ilies, Andreea CatanaLaura CristinaNo ratings yet
- 1-Day Hormone Reset PlanDocument20 pages1-Day Hormone Reset PlanPaola Soto100% (3)
- Chapter 11 - Pathology The Clinical Description of Hum - 2009 - Molecular Patho PDFDocument11 pagesChapter 11 - Pathology The Clinical Description of Hum - 2009 - Molecular Patho PDFSELNo ratings yet
- Senbazuru Details and InstructionsDocument10 pagesSenbazuru Details and InstructionsShoeb KarimNo ratings yet
- 31 LaboratoryDocument38 pages31 Laboratorymahaboob khanNo ratings yet
- Advanced Cardiac Life Support (ACLS)Document17 pagesAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapNo ratings yet
- Emory Cardiology Newsletter June 2009Document9 pagesEmory Cardiology Newsletter June 2009hnaguNo ratings yet
- Full Download Emergency Care 13th Edition Limmer Test BankDocument35 pagesFull Download Emergency Care 13th Edition Limmer Test BanksaabatmandearnestusNo ratings yet
- Growing ApricotDocument9 pagesGrowing ApricotRajNo ratings yet
- Read online textbook A Compendium Of Neuropsychological Tests Fundamentals Of Neuropsychological Assessment And Test Reviews For Clinical Practice 4E Sep 21 2021_0199856184_Oxford University Press 4Th Edition Sh ebook all chapter pdfDocument23 pagesRead online textbook A Compendium Of Neuropsychological Tests Fundamentals Of Neuropsychological Assessment And Test Reviews For Clinical Practice 4E Sep 21 2021_0199856184_Oxford University Press 4Th Edition Sh ebook all chapter pdflisa.roper448100% (9)
- B Modalities of RRT PDF 6542344047Document309 pagesB Modalities of RRT PDF 6542344047srihandayani1984No ratings yet