Download as ppt, pdf, or txt
You might also like
- Exam Preparatory Manual, Paediatrics, Snehal Patel, 2eDocument2,737 pagesExam Preparatory Manual, Paediatrics, Snehal Patel, 2eklen80% (5)
- Genentech Student Worksheet - ResultDocument10 pagesGenentech Student Worksheet - ResultArijit MajiNo ratings yet
- Sports PhysicalDocument6 pagesSports Physicalapi-671085061No ratings yet
- Physical AssessmentDocument19 pagesPhysical AssessmentMamerto Q. Flores IIINo ratings yet
- Pressure UlcerDocument35 pagesPressure Ulcerenam professor100% (1)
- Skin Care PowerpointDocument52 pagesSkin Care Powerpointisapatrick812667% (3)
- International PU Classification 2009Document2 pagesInternational PU Classification 2009metabolismeprotein100% (1)
- Pressure Ulcer DR MirfatDocument50 pagesPressure Ulcer DR MirfatDrmirfat AlkashifNo ratings yet
- Pressure Ulcers SimplifiedDocument8 pagesPressure Ulcers SimplifiedMsPocketbook HoarderNo ratings yet
- The Wound CareDocument51 pagesThe Wound CareIosefina DudeanuNo ratings yet
- Wound CareDocument7 pagesWound CareAbogadie Dione Blas ReyNo ratings yet
- Pressure Ulcers Hand OutDocument52 pagesPressure Ulcers Hand OutAdiAri RosiuNo ratings yet
- Pressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyDocument40 pagesPressure Sores (Bed Sores) : Presented By: Ms - Celine AntonyjyothiNo ratings yet
- S M D U: KIN Anagement Ecubitis LcerDocument77 pagesS M D U: KIN Anagement Ecubitis LcerabidNo ratings yet
- Pressure Sores & ManagementDocument15 pagesPressure Sores & Managementmupt77No ratings yet
- Decubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EDocument32 pagesDecubitus Ulcer: Presenters: Angod, Lady Aizahlyn I. Apat, Joselle Janina F. Araune, Trixie Mariel EXaxa AngodNo ratings yet
- Pressure Injuries: RLE Group 4: Iris Khan April Labrador Erika Lorenzana Blaise Lozano JM MatadosDocument17 pagesPressure Injuries: RLE Group 4: Iris Khan April Labrador Erika Lorenzana Blaise Lozano JM MatadosApril Mae Magos LabradorNo ratings yet
- Mpaired Skin Integrity.Document8 pagesMpaired Skin Integrity.Tamil VillardoNo ratings yet
- Wounds Part OneDocument15 pagesWounds Part Onemei robiwidodoNo ratings yet
- Basic Skin Care and Prevention of Pressure UlcersDocument9 pagesBasic Skin Care and Prevention of Pressure UlcersGeanieveve ElnasNo ratings yet
- Pressure UlcerDocument66 pagesPressure UlcerSwarnkar JayeshNo ratings yet
- Preskas Bedah Plastik NeonizaDocument30 pagesPreskas Bedah Plastik NeonizaRaNo ratings yet
- 1.RagragPreventing Pressure Sore.1Document18 pages1.RagragPreventing Pressure Sore.1alsamixersNo ratings yet
- Wound Assessment & CareDocument32 pagesWound Assessment & Caresami siddiqNo ratings yet
- Bedsores: Eligrace F. Fabian, RNDocument22 pagesBedsores: Eligrace F. Fabian, RNsweetsai05No ratings yet
- Assessment of Skin and Pressure Sore (Anp DemoDocument7 pagesAssessment of Skin and Pressure Sore (Anp DemoAnnette Baines100% (1)
- Skin IntegrityDocument112 pagesSkin IntegrityHerlina NababanNo ratings yet
- 022.pressure Sore (Bedsores) - 1Document21 pages022.pressure Sore (Bedsores) - 1Drsauga France100% (1)
- Pressure Sore or Decubitus Ulcer or Bed SoreDocument20 pagesPressure Sore or Decubitus Ulcer or Bed SorePrecious BlessingNo ratings yet
- Pressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisDocument7 pagesPressure Injury Documentation and Assessment: A Guide To State-Of-The-Art Staging and Recording of PisAlexis TrivinoNo ratings yet
- Nursing Assessment On Integumentary System: by Evelin MalintiDocument49 pagesNursing Assessment On Integumentary System: by Evelin Malintiwinda friyantiNo ratings yet
- Wound Care: Presentation For ACC Lab March 22, 2006Document19 pagesWound Care: Presentation For ACC Lab March 22, 2006heka_amrongNo ratings yet
- Pdfill PDF Editor With Free Writer and Tools: Physical AssessmentDocument20 pagesPdfill PDF Editor With Free Writer and Tools: Physical Assessmentgheen215100% (1)
- B11. Manajemen Luka Tekan 2017 OkDocument38 pagesB11. Manajemen Luka Tekan 2017 OkendraNo ratings yet
- Pressure Sores: Tehmina Noreen Post RN 2 YearDocument21 pagesPressure Sores: Tehmina Noreen Post RN 2 Yearbilal haiderNo ratings yet
- Physical Assessment: Lecturer: Mark Fredderick R. Abejo R.N, M.A.NDocument20 pagesPhysical Assessment: Lecturer: Mark Fredderick R. Abejo R.N, M.A.NRyan Biwit100% (4)
- Skin Care and Management of Pressure UlcerDocument24 pagesSkin Care and Management of Pressure UlcerchellczyNo ratings yet
- Risk For Impaired Skin IntegrityDocument4 pagesRisk For Impaired Skin IntegrityArelys Rodriguez100% (2)
- Decubitus Ulcer / Pressure SoresDocument1 pageDecubitus Ulcer / Pressure SoresMabesNo ratings yet
- Case Study: La Consolacion College ManilaDocument9 pagesCase Study: La Consolacion College ManilaAr DamotNo ratings yet
- What Is Pressure Ulcer?: Signs and SymptomsDocument6 pagesWhat Is Pressure Ulcer?: Signs and Symptomsshenecajean carajayNo ratings yet
- How To Evaluate A Case of LeprosyDocument35 pagesHow To Evaluate A Case of LeprosyBarath Kumar SinghNo ratings yet
- Decubetic Ulcer (Bed Sores)Document22 pagesDecubetic Ulcer (Bed Sores)Jerry ZahidNo ratings yet
- Pressure Ulcers: by Mr. M. Shivanandha ReddyDocument35 pagesPressure Ulcers: by Mr. M. Shivanandha ReddyDr Ali100% (2)
- Pressure Sores: AssessmentDocument7 pagesPressure Sores: AssessmentXyzelle Kim Monteilo OrtizNo ratings yet
- What Is BedsoresDocument4 pagesWhat Is Bedsoresver_at_workNo ratings yet
- Unit 11 Skin Integrity and Wound CareDocument47 pagesUnit 11 Skin Integrity and Wound CareAshaNo ratings yet
- Wound Care Management 1Document99 pagesWound Care Management 1Jan Oliver YaresNo ratings yet
- PediatricsDocument11 pagesPediatricsAmanuelNo ratings yet
- Bedsores PDFDocument13 pagesBedsores PDFsimi yNo ratings yet
- Pressure UlcersDocument36 pagesPressure UlcershylenshacNo ratings yet
- Pressure Ulcers - Surgery I March 2019Document63 pagesPressure Ulcers - Surgery I March 2019daniyfondoNo ratings yet
- Skin IntegrityDocument56 pagesSkin IntegrityneehoshiNo ratings yet
- Skin and Pressure SoresDocument24 pagesSkin and Pressure SoresJennyNo ratings yet
- Wound Documentation Tips PDFDocument2 pagesWound Documentation Tips PDFWinnie LiNo ratings yet
- Pressure Ulcers: Jorge G. Ruiz, MD, FACPDocument71 pagesPressure Ulcers: Jorge G. Ruiz, MD, FACPRomilPatelNo ratings yet
- DR Mohit Gulati (PT)Document62 pagesDR Mohit Gulati (PT)Shubha DiwakarNo ratings yet
- Decubitus UlcersDocument4 pagesDecubitus UlcersNkk Aqnd MgdnglNo ratings yet
- Hips Back Ankles Buttocks HeelsDocument13 pagesHips Back Ankles Buttocks Heelsفرزدق الحسيناويNo ratings yet
- Tissue Integrity Outline Spring 2023Document25 pagesTissue Integrity Outline Spring 2023morganstorey0No ratings yet
- Wound Care: The BasicsDocument26 pagesWound Care: The Basicsomar abdulrauofNo ratings yet
- A Simple Guide To Pressure Injuries, Diagnosis, Treatment And Related ConditionsFrom EverandA Simple Guide To Pressure Injuries, Diagnosis, Treatment And Related ConditionsNo ratings yet
- The Dermatology Handbook: A Clinician's GuideFrom EverandThe Dermatology Handbook: A Clinician's GuideNeelam A. VashiNo ratings yet
- Lesson (12) Stoma CareDocument5 pagesLesson (12) Stoma CareDrmirfat AlkashifNo ratings yet
- Final Sheet POD (NRSG-3302)Document8 pagesFinal Sheet POD (NRSG-3302)Drmirfat AlkashifNo ratings yet
- Lesson (13) Collection of SpecimensDocument10 pagesLesson (13) Collection of SpecimensDrmirfat AlkashifNo ratings yet
- Lesson (6) Assessment of Gestational AgeDocument26 pagesLesson (6) Assessment of Gestational AgeDrmirfat AlkashifNo ratings yet
- A Randomised, Double-Blind, Placebo-Controlled Study: Acupressure Treatment of Morning Sickness in PregnancyDocument5 pagesA Randomised, Double-Blind, Placebo-Controlled Study: Acupressure Treatment of Morning Sickness in PregnancyDrmirfat AlkashifNo ratings yet
- Nwafoh FinalDocument86 pagesNwafoh FinalDrmirfat AlkashifNo ratings yet
- 766Document106 pages766Drmirfat AlkashifNo ratings yet
- Kylie Armstrong ThesisDocument369 pagesKylie Armstrong ThesisDrmirfat AlkashifNo ratings yet
- Thesis 2Document94 pagesThesis 2Drmirfat AlkashifNo ratings yet
- The Use of Fresh Ginger Herbs As A Home Remedy To Relieve Primary DysmenorrheaDocument10 pagesThe Use of Fresh Ginger Herbs As A Home Remedy To Relieve Primary DysmenorrheaDrmirfat AlkashifNo ratings yet
- Cover PageDocument7 pagesCover PageDrmirfat AlkashifNo ratings yet
- Course Spec NRSG 352 Sec Sem1441Document10 pagesCourse Spec NRSG 352 Sec Sem1441Drmirfat AlkashifNo ratings yet
- Skin Sutures and StaplesDocument4 pagesSkin Sutures and StaplesDrmirfat AlkashifNo ratings yet
- Blood SampleDocument12 pagesBlood SampleDrmirfat AlkashifNo ratings yet
- Blood TransfusionDocument28 pagesBlood TransfusionDrmirfat AlkashifNo ratings yet
- Evidence Based PracticeDocument26 pagesEvidence Based PracticeDrmirfat AlkashifNo ratings yet
- Clinical Handout - NGT Feeding .Document2 pagesClinical Handout - NGT Feeding .Drmirfat AlkashifNo ratings yet
- TractionDocument24 pagesTractionDrmirfat AlkashifNo ratings yet
- 3.6.2020 Final Final Manual - Logbook For Students For Adult 2Document34 pages3.6.2020 Final Final Manual - Logbook For Students For Adult 2Drmirfat AlkashifNo ratings yet
- Assistive Devices Supportive DevicesDocument29 pagesAssistive Devices Supportive DevicesDrmirfat AlkashifNo ratings yet
- Nasogastric TubeDocument9 pagesNasogastric TubeDrmirfat AlkashifNo ratings yet
- Hemophilia رهفDocument3 pagesHemophilia رهفDrmirfat AlkashifNo ratings yet
- Case Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDocument7 pagesCase Study: Congestive Heart Failure By: Daniel Angelo E. ArangoDaniel Angelo ArangoNo ratings yet
- Myopia & StrabismusDocument1 pageMyopia & StrabismusBaebee LouNo ratings yet
- Unit 2 - Medical Coding ScenariosDocument2 pagesUnit 2 - Medical Coding ScenariosJonna Legaspo OdtojanNo ratings yet
- Sugaton Clinical Duty Forms Guide 2nddayDocument12 pagesSugaton Clinical Duty Forms Guide 2nddayPrincess Faniega SugatonNo ratings yet
- Hepatorenal Syndrome - Introduction and DiagnosisDocument38 pagesHepatorenal Syndrome - Introduction and DiagnosisbornflaxNo ratings yet
- Cardiovascular Pathology FINALDocument45 pagesCardiovascular Pathology FINALIanNo ratings yet
- Mosquito Borne DiseasesDocument24 pagesMosquito Borne DiseasesSidney BowenNo ratings yet
- Covid PregnancyDocument3 pagesCovid PregnancyDianeNo ratings yet
- CH 073 Shock in Office PracticeDocument8 pagesCH 073 Shock in Office PracticeLaxmikant RathiNo ratings yet
- 12 Engcore Readingunseenpassage tp03Document4 pages12 Engcore Readingunseenpassage tp03Bhargavi SaxenaNo ratings yet
- June 2020 DNB Question BankDocument3 pagesJune 2020 DNB Question Bankvittal iNo ratings yet
- Macro PneumohemoDocument28 pagesMacro PneumohemoSiti AishahNo ratings yet
- Blaylock Arthritis 25Document12 pagesBlaylock Arthritis 25mohanp71No ratings yet
- Asco Treatment Summary and Survivorship Care PlanDocument2 pagesAsco Treatment Summary and Survivorship Care PlanFriska Permatasari NababanNo ratings yet
- Genetic Mutation and DisorderDocument31 pagesGenetic Mutation and Disorderabrielle dytucoNo ratings yet
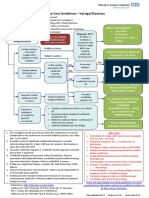
- ENT Vertigo FINAL v0.41Document1 pageENT Vertigo FINAL v0.41Farmasi BhamadaNo ratings yet
- NN 2Document10 pagesNN 2Thành ĐinhNo ratings yet
- Needle Stick InjuriesDocument24 pagesNeedle Stick InjuriesSarthak LaboratoryNo ratings yet
- AnaphylaxisDocument22 pagesAnaphylaxischitra gayenNo ratings yet
- ICD 10 CM Coding - DiabetesDocument68 pagesICD 10 CM Coding - Diabeteschaitanya varmaNo ratings yet
- LeptospirosisDocument26 pagesLeptospirosisDinesh KumarNo ratings yet
- GlaucomaDocument1 pageGlaucomaFam GdtNo ratings yet
- Vac Form 2 ReportsDocument1 pageVac Form 2 ReportsBetty LaoangNo ratings yet
- Unit 1 AnswerDocument22 pagesUnit 1 Answerii Dr3slNo ratings yet
- The Vijayanagar Empire History Project Class 12 C 2Document4 pagesThe Vijayanagar Empire History Project Class 12 C 2vanshchitkara2No ratings yet
- Pediatrics Rapid RevisionDocument72 pagesPediatrics Rapid RevisionWorld MedclickzNo ratings yet
- Copy of Q3-PPT-HEALTH 9 (Dressing and Bandages)Document36 pagesCopy of Q3-PPT-HEALTH 9 (Dressing and Bandages)ADRIAN ELISEONo ratings yet