Download as pptx, pdf, or txt
You might also like
- 15 - Children With Difficulty in Displaying Interpersonal BehaviorDocument3 pages15 - Children With Difficulty in Displaying Interpersonal BehaviorBarbado Arlene100% (7)
- Epidemiology of Mental HealthDocument15 pagesEpidemiology of Mental HealthClaire MolinaNo ratings yet
- Jon Thompson Naked Mentalism 3Document100 pagesJon Thompson Naked Mentalism 3AlaaFathey100% (7)
- Anxiety DisordersDocument39 pagesAnxiety DisordersAugene ToribioNo ratings yet
- Unit 2 Abnormal NotesDocument3 pagesUnit 2 Abnormal NotesKhushi BafnaNo ratings yet
- GAD, OCD and OCD Related DisordersDocument21 pagesGAD, OCD and OCD Related DisordersAkshita ZuzzanneNo ratings yet
- Psychological Disorders 2Document29 pagesPsychological Disorders 2ajithkumar2526No ratings yet
- Lesson 4Document50 pagesLesson 4Rhen DacugNo ratings yet
- Obsessive-Compulsive and Related DisordersDocument16 pagesObsessive-Compulsive and Related DisordersJoanNo ratings yet
- Lesson 6 STRESSDocument37 pagesLesson 6 STRESSjcaramat.dpnNo ratings yet
- Obsessive Compulsive Related Disorders: PSYC 340Document21 pagesObsessive Compulsive Related Disorders: PSYC 340Sana FatimaNo ratings yet
- Psychological DisordersREVDocument18 pagesPsychological DisordersREVlucas OmondiNo ratings yet
- Psychological Disorders and TreatmentDocument9 pagesPsychological Disorders and TreatmentSyed Masroor RinatNo ratings yet
- Biopsychology of Psychiatruc Disorders - PPTX Filename UTF 8biopsychology of Psychiatruc DisordersDocument50 pagesBiopsychology of Psychiatruc Disorders - PPTX Filename UTF 8biopsychology of Psychiatruc DisordersMary Claire Bagioen100% (1)
- Steps of Nursing Process Pertinent Nursing Diagnosis, Outcomes Apply QSEN PrinciplesDocument8 pagesSteps of Nursing Process Pertinent Nursing Diagnosis, Outcomes Apply QSEN Principlesjustjesko0lNo ratings yet
- Piyush Saurabh OCDDocument7 pagesPiyush Saurabh OCDhelalNo ratings yet
- Anxiety DisordersDocument41 pagesAnxiety Disorderskshavers2tougalooNo ratings yet
- Anxiety and AutismDocument37 pagesAnxiety and AutismMariela MonteroNo ratings yet
- Mental Health & Mental IllnessDocument18 pagesMental Health & Mental IllnessBonJovi Mojica Artista100% (1)
- Abnormal Psychology TestDocument19 pagesAbnormal Psychology TestJona MaeNo ratings yet
- Chapter 5 Anxiety Trauma and Stressor Related and Obsessive Compulsive and Related DisorderDocument43 pagesChapter 5 Anxiety Trauma and Stressor Related and Obsessive Compulsive and Related DisorderGabriel Jeremy OrtegaNo ratings yet
- Mental Health AwarenessDocument50 pagesMental Health AwarenessRari MirariNo ratings yet
- Ap Unit 4Document21 pagesAp Unit 4Vaishnavi RaveendranNo ratings yet
- Human Behavior and Crisis Managementfffff PDFDocument78 pagesHuman Behavior and Crisis Managementfffff PDFDan Lawrence Dela CruzNo ratings yet
- Psychology 1 TestDocument8 pagesPsychology 1 TestCarlos HurtadoNo ratings yet
- 4-Dissociation and FormDocument30 pages4-Dissociation and FormArmandoNo ratings yet
- CH 14 Psych DisordersDocument9 pagesCH 14 Psych Disordersюрий локтионовNo ratings yet
- Anxiety DisordersDocument49 pagesAnxiety DisordersMeena ViswaNo ratings yet
- Recognising Common Psychiatric IllnessesDocument22 pagesRecognising Common Psychiatric IllnessesAntonio BernardNo ratings yet
- Mental Health Well Being in Middle and LateDocument31 pagesMental Health Well Being in Middle and LateGemma Acorda BalaganNo ratings yet
- Abnormal PsychologyDocument33 pagesAbnormal PsychologyChristie SabgaNo ratings yet
- PERDEVDocument3 pagesPERDEVZeraNo ratings yet
- Psycological DisordersDocument62 pagesPsycological DisordersProjjal SanyalNo ratings yet
- Personal Development: Lesson 7Document24 pagesPersonal Development: Lesson 7Nikka Irah Camarista100% (1)
- Mood Disorders2Document73 pagesMood Disorders2Crisia GungobNo ratings yet
- Psychological Disorders: AP Psychology Mr. HollandDocument20 pagesPsychological Disorders: AP Psychology Mr. Hollandyummywords1254No ratings yet
- Anxiety Disorder NewDocument48 pagesAnxiety Disorder NewIndah Permata SariNo ratings yet
- Module 4a Handouts - Trauma - Anxiety - OCRD - SSRDDocument33 pagesModule 4a Handouts - Trauma - Anxiety - OCRD - SSRDPauline Vanessa ReyesNo ratings yet
- Types of Anxiety DisorderDocument5 pagesTypes of Anxiety Disordernilda asmin100% (1)
- Mental Health, Stress Management & CounselingDocument34 pagesMental Health, Stress Management & Counselingzhucarmen20No ratings yet
- Understanding Mental Health Problems 2016Document36 pagesUnderstanding Mental Health Problems 2016api-273164510No ratings yet
- AnxietyDocument36 pagesAnxietyRobert RevillasNo ratings yet
- Anxiety DisordersDocument62 pagesAnxiety DisordersJOHN PAUL KEVIN ESTANo ratings yet
- Behavior Topic: (Basic Concept)Document16 pagesBehavior Topic: (Basic Concept)Marikit2012No ratings yet
- Lecture 5Document12 pagesLecture 5gabi-rabeloNo ratings yet
- PSYC 2300 040423 Lecture SlidesDocument20 pagesPSYC 2300 040423 Lecture SlidesCristinaNo ratings yet
- Mental Disorder: Psychological (Or Mental) DisordersDocument7 pagesMental Disorder: Psychological (Or Mental) DisordersEsha MeherNo ratings yet
- Anxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDDocument38 pagesAnxiety Disorder (Gangguan Cemas) : Ronny T Wirasto, MDadystiNo ratings yet
- Obsessive Compulsive DisorderDocument26 pagesObsessive Compulsive DisorderIshmarika 54No ratings yet
- Behavioral EmergenciesDocument65 pagesBehavioral EmergenciesPaulhotvw67100% (2)
- Understanding SchizophreniaDocument40 pagesUnderstanding SchizophreniarachelleallauiganNo ratings yet
- Anxiety DisordersDocument3 pagesAnxiety DisordersCamille Joy BaliliNo ratings yet
- Mental Health:: Anxiety DisorderDocument7 pagesMental Health:: Anxiety Disordergulshang786No ratings yet
- Mental Health Problems in Young People - Part 2Document71 pagesMental Health Problems in Young People - Part 2elaineNo ratings yet
- Anxiety DisordersDocument30 pagesAnxiety DisordersAbelNo ratings yet
- Final FY Presentation1Document45 pagesFinal FY Presentation1SamNo ratings yet
- Mental Health Chapter 1Document36 pagesMental Health Chapter 1Tarek QawasmehNo ratings yet
- Mental Health and Mental Disorder ReportDocument6 pagesMental Health and Mental Disorder ReportBonJovi Mojica ArtistaNo ratings yet
- Ocd MainDocument18 pagesOcd MainArushi SinghNo ratings yet
- 2009 Anxiety Disorders LectureDocument51 pages2009 Anxiety Disorders Lectureyanetp01No ratings yet
- The Ultimate Guide to Supporting Someone with Mental Illness: Managing Mental HealthFrom EverandThe Ultimate Guide to Supporting Someone with Mental Illness: Managing Mental HealthNo ratings yet
- Speech As Guild PresidentDocument3 pagesSpeech As Guild Presidentmujuni brianmjuNo ratings yet
- Characteristics of g3 - An Alternative To SF6Document5 pagesCharacteristics of g3 - An Alternative To SF6Abdul MoizNo ratings yet
- Mafia Ii 360 Download Manual EngDocument21 pagesMafia Ii 360 Download Manual EngJuan Camilo Payan GuerreroNo ratings yet
- M1 - 02 Nature and Scope of BusinessDocument41 pagesM1 - 02 Nature and Scope of BusinessDiptendu RoyNo ratings yet
- MODBUS TCP/IP (0x/1x Range Adjustable) : HMI SettingDocument5 pagesMODBUS TCP/IP (0x/1x Range Adjustable) : HMI SettingÁnh VũNo ratings yet
- GPRS Evolution PH 2Document43 pagesGPRS Evolution PH 2Nur AfiyatNo ratings yet
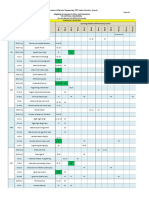
- Mapping PEC 2021-Oct-20 Annex-D Courses Vs PLO Vs TaxonomyDocument2 pagesMapping PEC 2021-Oct-20 Annex-D Courses Vs PLO Vs TaxonomyEngr.Mohsin ShaikhNo ratings yet
- MTA uniVAL Technical Data Sheet v00Document1 pageMTA uniVAL Technical Data Sheet v00muhammetNo ratings yet
- The Duality of Human Nature in Oscar Wilde's The Importance of Being EarnestDocument28 pagesThe Duality of Human Nature in Oscar Wilde's The Importance of Being EarnestSowmya ShreeNo ratings yet
- Quality Control Plan: ClientDocument7 pagesQuality Control Plan: ClienteliiiiiiNo ratings yet
- Perinatal Mental Health Policy BriefDocument3 pagesPerinatal Mental Health Policy BriefThe Wilson CenterNo ratings yet
- 4J10 CHUNG KA CHUN 4J10 - Untitled DocumentDocument1 page4J10 CHUNG KA CHUN 4J10 - Untitled Document4J10 CHUNG KA CHUN 4J10No ratings yet
- Competiveness of Sri Lankan Apparel IndustryDocument9 pagesCompetiveness of Sri Lankan Apparel IndustryDanuNo ratings yet
- Versatile, Efficient and Easy-To-Use Visual Imu-Rtk: Surveying & EngineeringDocument4 pagesVersatile, Efficient and Easy-To-Use Visual Imu-Rtk: Surveying & EngineeringMohanad MHPSNo ratings yet
- 02TP PrelimExam MITDocument2 pages02TP PrelimExam MITSnapShop by AJNo ratings yet
- Bahir Dar University College of Medicine and Health SciencesDocument21 pagesBahir Dar University College of Medicine and Health SciencesMegbaruNo ratings yet
- Distribution Channel of AMULDocument13 pagesDistribution Channel of AMULMeet JivaniNo ratings yet
- PHOTOCOPIABLE Gateway B1 Workbook AnswerDocument2 pagesPHOTOCOPIABLE Gateway B1 Workbook Answerhaler kolokNo ratings yet
- DT81 Data Logger DatasheetDocument2 pagesDT81 Data Logger DatasheetDuška JarčevićNo ratings yet
- Unit 1: A1 Coursebook AudioscriptsDocument39 pagesUnit 1: A1 Coursebook AudioscriptsRaul GaglieroNo ratings yet
- UN - HIV and Prison - Policy BriefDocument12 pagesUN - HIV and Prison - Policy BriefParomita2013No ratings yet
- A1 (2 3 4) F./... D 6905 Af/1Document3 pagesA1 (2 3 4) F./... D 6905 Af/1GERALD SIMONNo ratings yet
- Submarine Diesel EngineDocument106 pagesSubmarine Diesel EngineDharma Gita Surya PrayogaNo ratings yet
- En 13237-2003 Terms and Definitions For Equipment and Protective Systems Intended For Use in Potentially Explosive AtmospheresDocument26 pagesEn 13237-2003 Terms and Definitions For Equipment and Protective Systems Intended For Use in Potentially Explosive AtmospheresGargiulo AnitaNo ratings yet
- Sccan Resourcemanual Allpages Update v2Document154 pagesSccan Resourcemanual Allpages Update v2SiangNo ratings yet
- MIET2407 - OENG1181 - Final Report 2018Document4 pagesMIET2407 - OENG1181 - Final Report 2018Trần TínNo ratings yet
- A 201Document1 pageA 201AnuranjanNo ratings yet
- Story As World MakingDocument9 pagesStory As World MakingAugusto ChocobarNo ratings yet
- Supervisi Akademik Melalui Pendekatan Kolaboratif Oleh Kepala Sekolah Dalammeningkatkan Kualitas Pembelajarandisd Yari DwikurnaningsihDocument11 pagesSupervisi Akademik Melalui Pendekatan Kolaboratif Oleh Kepala Sekolah Dalammeningkatkan Kualitas Pembelajarandisd Yari DwikurnaningsihKhalid Ibnu SinaNo ratings yet