Download as pptx, pdf, or txt
You might also like
- DR Henry G Bieler Lines of Defense Against DiseaseDocument6 pagesDR Henry G Bieler Lines of Defense Against DiseasebonifacesilveiraNo ratings yet
- Neuromusculr Blocking Drugs&Reversal Agents and Courses of Delayed RecoveryDocument44 pagesNeuromusculr Blocking Drugs&Reversal Agents and Courses of Delayed RecoverysanjibNo ratings yet
- Skeletal Muscle RelaxantDocument44 pagesSkeletal Muscle RelaxantAhmar HasanNo ratings yet
- Pelumpuh OtotDocument55 pagesPelumpuh OtotWebinar AnestesiNo ratings yet
- Neuromuscular BlockersDocument49 pagesNeuromuscular Blockerssongo sorshimaNo ratings yet
- Skeletal Muscle Relaxants 1Document21 pagesSkeletal Muscle Relaxants 1pooja sureshNo ratings yet
- SMR 1Document20 pagesSMR 1Ahmar HasanNo ratings yet
- Neuromuscular Blcoking DrugsDocument30 pagesNeuromuscular Blcoking DrugsksNo ratings yet
- Perioperatif Antiemesis - Aiwi JapanesaDocument24 pagesPerioperatif Antiemesis - Aiwi JapanesafebrinasugiantoNo ratings yet
- DRUG PRESENTATION On Emergency and CPR DrugsDocument39 pagesDRUG PRESENTATION On Emergency and CPR DrugsShibi BennyNo ratings yet
- Lecture 15 Cholinergic TransmissionDocument20 pagesLecture 15 Cholinergic TransmissionSamer FarhanNo ratings yet
- Muscle RelaxantDocument46 pagesMuscle RelaxantJeremy HermantoNo ratings yet
- 2 AnticholinesterasesDocument55 pages2 AnticholinesterasesSudhakar LakavathNo ratings yet
- Cholinergic Agonists: Dr. Pramod P Bhalerao (M.D.) Asst. Professor Dept. of PharmacologyDocument48 pagesCholinergic Agonists: Dr. Pramod P Bhalerao (M.D.) Asst. Professor Dept. of Pharmacologypramod bhalerao0% (1)
- Rapid Sequence IntubationDocument58 pagesRapid Sequence IntubationArya VikneshNo ratings yet
- Introduction To General AnaesthesiaDocument77 pagesIntroduction To General AnaesthesiaAmirhossein SheikhiNo ratings yet
- Pharmacology of Autonomic Nervous SystemDocument29 pagesPharmacology of Autonomic Nervous SystemTahir AzizNo ratings yet
- L8 - Cholinergic Neurotransmission and The Skeletal NMJDocument8 pagesL8 - Cholinergic Neurotransmission and The Skeletal NMJlaylahd2003No ratings yet
- Neuromuscular Blocking Agents: DR - Jagadish JenaDocument109 pagesNeuromuscular Blocking Agents: DR - Jagadish Jenavvb_frndNo ratings yet
- Chrono Pharmaco LDocument46 pagesChrono Pharmaco LJaved AliNo ratings yet
- SKELETAL MUSCLE RELAXANTS NursingDocument63 pagesSKELETAL MUSCLE RELAXANTS NursingAbdur RafayNo ratings yet
- Generalanaesthesia Drdhriti 111223120647 Phpapp01Document64 pagesGeneralanaesthesia Drdhriti 111223120647 Phpapp01Ridha Surya NugrahaNo ratings yet
- PONV 30 Mar 2010 AmitDocument46 pagesPONV 30 Mar 2010 AmitAmit KochetaNo ratings yet
- Local Anaesthesia in DentistryDocument149 pagesLocal Anaesthesia in DentistryARNOLD OBINo ratings yet
- Drugs Acting On ANS: Presentation by Shreeya SharmaDocument12 pagesDrugs Acting On ANS: Presentation by Shreeya SharmaShreeya SharmaNo ratings yet
- VPHM50 Part3 2021Document173 pagesVPHM50 Part3 2021John Joshua J. MingiNo ratings yet
- L-19 Skeletal Muscle RelaxantDocument26 pagesL-19 Skeletal Muscle RelaxantZakiyahulfahdwNo ratings yet
- CholinomimeticsDocument64 pagesCholinomimeticsMariyam HanifNo ratings yet
- Pharmacology of AnaestheticsDocument28 pagesPharmacology of AnaestheticsRahaf AliNo ratings yet
- Learning Objectives: Drugs That Enhance Cholinergic TransmissionDocument3 pagesLearning Objectives: Drugs That Enhance Cholinergic TransmissionSamer FarhanNo ratings yet
- Anticholinergic Drugs 1Document29 pagesAnticholinergic Drugs 1Samarpita RoyNo ratings yet
- AnesthesiaDocument6 pagesAnesthesiaSamyuktha NatarajanNo ratings yet
- Drugs Acting On ANS: Presentation by ShreeyasharmaDocument12 pagesDrugs Acting On ANS: Presentation by ShreeyasharmaShreeya SharmaNo ratings yet
- Pharma Nca1 Notes MidtermDocument8 pagesPharma Nca1 Notes MidtermAICEL A. ABILNo ratings yet
- Biliary Tract SujanDocument25 pagesBiliary Tract SujanBikash SubediNo ratings yet
- Mpharm Year 1 Integrated Therapeutics Workshop 3Document29 pagesMpharm Year 1 Integrated Therapeutics Workshop 3Thao NguyenNo ratings yet
- Anaesthesia For Ect March 2020Document120 pagesAnaesthesia For Ect March 2020Sangkaran KumarNo ratings yet
- Skeletal Muscle Relaxants: DR RC AnakwueDocument24 pagesSkeletal Muscle Relaxants: DR RC AnakwuetemitopeNo ratings yet
- Drugs For Anesthesia, Muscle RelaxationDocument265 pagesDrugs For Anesthesia, Muscle RelaxationTamara Heradwita GSNo ratings yet
- Epilepsy Class - DrdhritiDocument81 pagesEpilepsy Class - DrdhritidbrahmaNo ratings yet
- Cholinoceptor AgonistsDocument7 pagesCholinoceptor AgonistsAaron Lee100% (1)
- Pharmacology of AnaestheticsDocument70 pagesPharmacology of AnaestheticsAcho91 08No ratings yet
- Skeletal Muscle RelaxantDocument18 pagesSkeletal Muscle Relaxantswaroop ranjan nandaNo ratings yet
- Ans Pharmacology 01 For Pc-IDocument54 pagesAns Pharmacology 01 For Pc-ITsegaye HailuNo ratings yet
- Anticholinergic Drugs: Presented byDocument26 pagesAnticholinergic Drugs: Presented byHuzaifa KhaleeqNo ratings yet
- Local Anaesthetic Agents (3) 2Document38 pagesLocal Anaesthetic Agents (3) 2MaleehaNo ratings yet
- Drugs Acting On Bone and NMJDocument99 pagesDrugs Acting On Bone and NMJgostrider0093sNo ratings yet
- Intubating Trauma PatientsDocument36 pagesIntubating Trauma PatientsJeremy HamptonNo ratings yet
- Malignant HyperthermiaDocument57 pagesMalignant HyperthermiaSuvadeep SenNo ratings yet
- Cholinergic AgonistDocument34 pagesCholinergic AgonistRoma BeygNo ratings yet
- 4.muscle RelaxantsDocument23 pages4.muscle Relaxantskarim hassanNo ratings yet
- Cholinergic Systems and Cholimimetic Drugs PresentationDocument43 pagesCholinergic Systems and Cholimimetic Drugs PresentationShaRath KmNo ratings yet
- PHARM Ven IntroToAnesthesiaDocument22 pagesPHARM Ven IntroToAnesthesiaDhaif dhaifNo ratings yet
- General Anesthesia PDFDocument38 pagesGeneral Anesthesia PDFCabdiNo ratings yet
- Clinical Use of DexmedetomidineDocument29 pagesClinical Use of DexmedetomidineAnil SathyadasNo ratings yet
- SMR2Document33 pagesSMR2Ahmar HasanNo ratings yet
- Neuromuscular Blockers: Musculoskeletal System Dr. Nalamolu Koteswara RaoDocument14 pagesNeuromuscular Blockers: Musculoskeletal System Dr. Nalamolu Koteswara RaomaggieNo ratings yet
- Ray Phase 1Document4 pagesRay Phase 1raysklineNo ratings yet
- Skeletal Muscle Relaxants 3 Pha 2013Document37 pagesSkeletal Muscle Relaxants 3 Pha 2013r0ben1nNo ratings yet
- L2 Anes NL2Document85 pagesL2 Anes NL26210310123No ratings yet
- Length Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesFrom EverandLength Tension Testing Book 2, Upper Quadrant: A Workbook of Manual Therapy TechniquesRating: 1 out of 5 stars1/5 (1)
- Chapter 4Document10 pagesChapter 4Laxman KannaNo ratings yet
- Medicine Disorder of Respiratory System TuberculosisDocument3 pagesMedicine Disorder of Respiratory System TuberculosisLaxman KannaNo ratings yet
- Patient PositioningDocument76 pagesPatient PositioningLaxman KannaNo ratings yet
- Electronic Reservation Slip (ERS) : 4754664374 16093/mas LJN Express Sleeper Class (SL)Document2 pagesElectronic Reservation Slip (ERS) : 4754664374 16093/mas LJN Express Sleeper Class (SL)Laxman KannaNo ratings yet
- Haematopoiesis and Its DisordersDocument38 pagesHaematopoiesis and Its DisordersLaxman KannaNo ratings yet
- 1 Circular StudentsDocument2 pages1 Circular StudentsLaxman KannaNo ratings yet
- Sterptococci 1Document15 pagesSterptococci 1Laxman KannaNo ratings yet
- HivDocument24 pagesHivLaxman KannaNo ratings yet
- PPTDocument6 pagesPPTLaxman KannaNo ratings yet
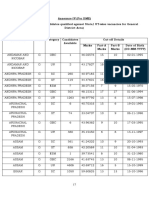
- SSC GD Male Cut Off General District AreaDocument7 pagesSSC GD Male Cut Off General District AreaLaxman KannaNo ratings yet
- Electronic Reservation Slip (ERS) : 4553608179 17652/Kcg CGL Express Sleeper Class (SL)Document2 pagesElectronic Reservation Slip (ERS) : 4553608179 17652/Kcg CGL Express Sleeper Class (SL)Laxman KannaNo ratings yet
- Hall Ticket No Name Grand Total Result/Grade: 2038114758 Eddu Laxman 415 ADocument1 pageHall Ticket No Name Grand Total Result/Grade: 2038114758 Eddu Laxman 415 ALaxman KannaNo ratings yet
- Alpaflor Edeleweiss A4 6pp 2021Document6 pagesAlpaflor Edeleweiss A4 6pp 2021Joatan de SousaNo ratings yet
- Self-Assessment Questions Chapter 1 IntroductionDocument8 pagesSelf-Assessment Questions Chapter 1 IntroductionHASSET SHIFERAWNo ratings yet
- DiGeorge SyndromeDocument18 pagesDiGeorge SyndromeRupesh MohandasNo ratings yet
- Operating Procedure1Document2 pagesOperating Procedure1Ege AeeNo ratings yet
- Diagnosis, and Therapeutic Management of Alcoholic Liver Disease. Int J Mol SciDocument5 pagesDiagnosis, and Therapeutic Management of Alcoholic Liver Disease. Int J Mol SciHasna Dhea SyafieraNo ratings yet
- Anindra Nallapat (33Y/M) Diabetc Profle - Advanced New: Report For Tests AskedDocument28 pagesAnindra Nallapat (33Y/M) Diabetc Profle - Advanced New: Report For Tests AskedAnindra NallapatiNo ratings yet
- Alfa ResultClinicalGroup 2Document2 pagesAlfa ResultClinicalGroup 2Abdulrahman DiabNo ratings yet
- Drug AnalysisDocument18 pagesDrug AnalysisArt Christian RamosNo ratings yet
- Mohammed H. Eid - The Intensivist-Middle East & ElMarwa For Publishing & Distribution, GN (2019)Document372 pagesMohammed H. Eid - The Intensivist-Middle East & ElMarwa For Publishing & Distribution, GN (2019)Mohamed Moussa100% (1)
- SteroidsDocument56 pagesSteroidsPhantomNo ratings yet
- Full Download PDF of (Ebook PDF) Biology Today and Tomorrow With Physiology 5th Edition All ChapterDocument43 pagesFull Download PDF of (Ebook PDF) Biology Today and Tomorrow With Physiology 5th Edition All Chapterpeaznurtai100% (5)
- ObesityDocument50 pagesObesityKetan JainNo ratings yet
- Drug Clearance: Dr. Rajib Bhattacharjee Asstt. Professor Dept of Pharmacy, NSUDocument11 pagesDrug Clearance: Dr. Rajib Bhattacharjee Asstt. Professor Dept of Pharmacy, NSUMohannad AlfadhalNo ratings yet
- Mszoubi@yu - Edu.jo Z.altaany@yu - Edu.jo: Yarmouk University Faculty of Medicine Biochemistry (M 113) Summer 2022Document3 pagesMszoubi@yu - Edu.jo Z.altaany@yu - Edu.jo: Yarmouk University Faculty of Medicine Biochemistry (M 113) Summer 2022رهف مالك محمود برهوشNo ratings yet
- Interpretation: A06 - Raj Hospital - Cash (Cghs - 20) Main Road Ranchi Jharkhand 834001Document4 pagesInterpretation: A06 - Raj Hospital - Cash (Cghs - 20) Main Road Ranchi Jharkhand 834001AlokNo ratings yet
- Contraceptive Patch - BetchosoDocument18 pagesContraceptive Patch - BetchosoCharlotte BetchosoNo ratings yet
- HY USMLE Review Part IVDocument31 pagesHY USMLE Review Part IVDr.2020100% (1)
- Is The ABG Valid?Document16 pagesIs The ABG Valid?alexNo ratings yet
- Cambridge International AS & A Level: Biology 9700/22 March 2021Document15 pagesCambridge International AS & A Level: Biology 9700/22 March 2021Pom GNo ratings yet
- Grade 10 12 Biology Notes NutritionDocument50 pagesGrade 10 12 Biology Notes NutritionMapalo ChirwaNo ratings yet
- GalactosemiaDocument11 pagesGalactosemiahajiaewenlaNo ratings yet
- Medical Technology ReviewerDocument57 pagesMedical Technology ReviewerOng Christopher100% (2)
- Comprehensive Sexuality Education Integrartion Lesson Plan in Science 10Document7 pagesComprehensive Sexuality Education Integrartion Lesson Plan in Science 10Louina Fernandez Atlas100% (1)
- Mit Syllabus 1Document76 pagesMit Syllabus 1Gouspeer MNo ratings yet
- Aspartate Aminotransferase Ifcc Manual RX Monza Intended UseDocument4 pagesAspartate Aminotransferase Ifcc Manual RX Monza Intended UseBenedicta OjoNo ratings yet
- General Medicine SEQs SolvedDocument33 pagesGeneral Medicine SEQs SolvedMajid Ahmed FareaNo ratings yet
- Gynae T and D Expl - 1Document44 pagesGynae T and D Expl - 1vivekanurag97No ratings yet
- Malignant LymphomaDocument10 pagesMalignant LymphomaJamela Mer AlbertoNo ratings yet
- Spect Art. 1Document11 pagesSpect Art. 1AxelSesT MtzNo ratings yet