Download as pptx, pdf, or txt
You might also like
- Unexpected Joy at Dawn - Docx AnalysisDocument8 pagesUnexpected Joy at Dawn - Docx AnalysisBasil Ekwenye100% (1)
- SKIN TYPES Roberts2009Document5 pagesSKIN TYPES Roberts2009Brigitte Elisa Vivanco CcahuanaNo ratings yet
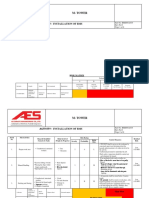
- Risk Assessment For Installation of BMS M Tower PDFDocument15 pagesRisk Assessment For Installation of BMS M Tower PDFAndrew HivNo ratings yet
- Thumb Rules For Civil Engineers PDFDocument4 pagesThumb Rules For Civil Engineers PDFA KNo ratings yet
- Lease Financing PDFDocument31 pagesLease Financing PDFreshma100% (5)
- Cosmetic Concerns Among Ethnic Men: Michelle HenryDocument6 pagesCosmetic Concerns Among Ethnic Men: Michelle HenryMaybelineNo ratings yet
- Considerations When Treating Cosmetic Concerns in Men Skin ColorDocument11 pagesConsiderations When Treating Cosmetic Concerns in Men Skin ColorElaine MedeirosNo ratings yet
- Peeling Pieles Oscuras PDFDocument21 pagesPeeling Pieles Oscuras PDFHugh MantaNo ratings yet
- Scar Treatment Variations by Skin TypeReview ArticleDocument10 pagesScar Treatment Variations by Skin TypeReview ArticledoctorbanNo ratings yet
- Top Six Health Issue in SingaporeDocument22 pagesTop Six Health Issue in SingaporeMatthewRumondorNo ratings yet
- Laser Skin Treatment in Non-Caucasian PatientsReview ArticleDocument8 pagesLaser Skin Treatment in Non-Caucasian PatientsReview ArticledoctorbanNo ratings yet
- Characteristics and Management of Asian SkinDocument13 pagesCharacteristics and Management of Asian SkinJeffrey HardingNo ratings yet
- 1 s2.0 S0015028216613523 MainDocument9 pages1 s2.0 S0015028216613523 MainelisaparedesNo ratings yet
- Arya. Skin Path LabDocument54 pagesArya. Skin Path LabMJO79No ratings yet
- Normal Skin Findings and Cultural Practices in Pediatric PatientsDocument9 pagesNormal Skin Findings and Cultural Practices in Pediatric PatientsMarice QCNo ratings yet
- A Comparative Study of Dermatoscopic Features of Acne-Related Postinfl Ammatory Hyperpigmentation in Facial and Nonfacial Areas in Asian PatientsDocument6 pagesA Comparative Study of Dermatoscopic Features of Acne-Related Postinfl Ammatory Hyperpigmentation in Facial and Nonfacial Areas in Asian Patientsdesi kumarayantiNo ratings yet
- Hicks 2003Document8 pagesHicks 2003Cristiane Leao dos SantosNo ratings yet
- brown2011Document4 pagesbrown2011z8hc2s6scpNo ratings yet
- Freckles and Solar Lentigines Have Different Risk Factors in Caucasian WomenDocument12 pagesFreckles and Solar Lentigines Have Different Risk Factors in Caucasian WomenagityaNo ratings yet
- Photoaging of The SkinDocument31 pagesPhotoaging of The SkinMarnie RoviraNo ratings yet
- Evaluating The Cosmetic PatientDocument71 pagesEvaluating The Cosmetic Patientdocrubes50No ratings yet
- An Update On Cosmetic Procedures in 2Document40 pagesAn Update On Cosmetic Procedures in 2Namrata PradhanNo ratings yet
- Bennett 2009Document37 pagesBennett 2009KosmetykiNo ratings yet
- Superficial and Medium-Depth Chemical PeelsDocument10 pagesSuperficial and Medium-Depth Chemical PeelsFenni Oktoberry100% (1)
- International Journal of Women's Dermatology: P.E. Grimes, MD, S. Ijaz, BA, MPH, R. Nashawati, BS, MSGM, D. KwakDocument7 pagesInternational Journal of Women's Dermatology: P.E. Grimes, MD, S. Ijaz, BA, MPH, R. Nashawati, BS, MSGM, D. KwakRiefka Ananda ZulfaNo ratings yet
- New Oral and Topical Approaches For The Treatment of MelasmaDocument7 pagesNew Oral and Topical Approaches For The Treatment of MelasmaSong JieunNo ratings yet
- Effect of Age, Gender, and Sun Exposure On Ethnic Skin Photoaging: Evidence Gathered Using A New Photonumeric ScaleDocument6 pagesEffect of Age, Gender, and Sun Exposure On Ethnic Skin Photoaging: Evidence Gathered Using A New Photonumeric ScaleRiefka Ananda ZulfaNo ratings yet
- Chemical Peeling With Trichloroacetic Acid and Lactic Acid For Infraorbital Dark CirclesDocument6 pagesChemical Peeling With Trichloroacetic Acid and Lactic Acid For Infraorbital Dark CirclesAna Claudia Kordelos DinizNo ratings yet
- Jablonski Skin Color 2000Document50 pagesJablonski Skin Color 2000Canario JuniorNo ratings yet
- Clinico Morphological Evaluation of Melasma and Other Hyperpigmentary Disorders of SkinDocument25 pagesClinico Morphological Evaluation of Melasma and Other Hyperpigmentary Disorders of SkinBaru Chandrasekhar RaoNo ratings yet
- Melanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Document53 pagesMelanoma: Edward Buckingham, M.D. Combined Plastics Conference September 6, 2000Kadek Ariarta MahartamaNo ratings yet
- Colour Homogeneity and Visual Perception of Age, Health and Attractiveness of Male Facial SkinDocument7 pagesColour Homogeneity and Visual Perception of Age, Health and Attractiveness of Male Facial Skinteste testeNo ratings yet
- Evaluation of A Retinol Containing Topical Treatment To Improve Signs of Neck AgingDocument10 pagesEvaluation of A Retinol Containing Topical Treatment To Improve Signs of Neck AgingLiz HaylettNo ratings yet
- Medsurg 7 Assessment: Integumentary System: Structures and FunctionsDocument7 pagesMedsurg 7 Assessment: Integumentary System: Structures and FunctionsjefrocNo ratings yet
- PD0319 Candela InsertDocument8 pagesPD0319 Candela InsertTrần Hồng MyNo ratings yet
- 2005-Pigmentary Mosaicism and MosaicDocument2 pages2005-Pigmentary Mosaicism and MosaicANo ratings yet
- Percutaneous Radiofrequency Technologiesforthelower FaceandneckDocument16 pagesPercutaneous Radiofrequency Technologiesforthelower FaceandnecksadraNo ratings yet
- Use of CO2 Laser For The Treatment of Acne and Burn Scars in Indian Skin...Document8 pagesUse of CO2 Laser For The Treatment of Acne and Burn Scars in Indian Skin...Phúc LâmNo ratings yet
- GenderMed2007!4!308 Gender Skin DifferencesDocument21 pagesGenderMed2007!4!308 Gender Skin DifferencesFitriLerianNo ratings yet
- Overview of Skin Aging and PhotoagingDocument7 pagesOverview of Skin Aging and PhotoagingtissanNo ratings yet
- Healthcare 11 02091Document15 pagesHealthcare 11 02091MartinoKhanzaniaNo ratings yet
- Geriatric Dermatoses: A Clinical Review of Skin Diseases in An Aging PopulationDocument14 pagesGeriatric Dermatoses: A Clinical Review of Skin Diseases in An Aging PopulationIPD Soewandie A-BNo ratings yet
- LEPROSYDocument27 pagesLEPROSYMohan SrinivasNo ratings yet
- Melasma A Prospective Study of Clinico Etiological and Dermoscopic Pattern in MenDocument4 pagesMelasma A Prospective Study of Clinico Etiological and Dermoscopic Pattern in MenInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- BSP 2D - Group 1 - Adaptation of Human Skin Color in Various PopulationsDocument8 pagesBSP 2D - Group 1 - Adaptation of Human Skin Color in Various Populationsbspsych.borromeokjpNo ratings yet
- Topic Treatment Acne Scars1Document3 pagesTopic Treatment Acne Scars1Stanca NicolaeNo ratings yet
- Disorders of Hyperpigmentation HandoutDocument34 pagesDisorders of Hyperpigmentation Handoutdaliabas73No ratings yet
- Oily Skin 1Document7 pagesOily Skin 1GligorpaulaNo ratings yet
- Ethnic Skin Types: Are There Differences in Skin Structure and Function?Document15 pagesEthnic Skin Types: Are There Differences in Skin Structure and Function?KosmetykiNo ratings yet
- Liken PlanusDocument6 pagesLiken PlanusAmirahShalehaNo ratings yet
- Subungual MelanomaDocument50 pagesSubungual Melanomastefani83No ratings yet
- M CAD Ermatol CtoberDocument1 pageM CAD Ermatol CtoberFerdie YuzonNo ratings yet
- Deka Upl Melasma Ipl Zoccali Et Al 2010Document9 pagesDeka Upl Melasma Ipl Zoccali Et Al 2010isma drNo ratings yet
- The Association Between Melasma and Postin Ammatory Hyperpigmenta-Tion in Acne PatientsDocument4 pagesThe Association Between Melasma and Postin Ammatory Hyperpigmenta-Tion in Acne PatientsRicoNo ratings yet
- Microneedling in Skin of ColorDocument8 pagesMicroneedling in Skin of ColorDiva Natasya KrismanitaNo ratings yet
- Cosmetics: What Makes Indian Women Look Older-An Exploratory Study On Facial Skin FeaturesDocument15 pagesCosmetics: What Makes Indian Women Look Older-An Exploratory Study On Facial Skin FeaturesKavirm35No ratings yet
- How To Write A Global Health Case ReportDocument5 pagesHow To Write A Global Health Case ReportpranabchatterjeeNo ratings yet
- Adamson2017 Critica Ao Termo Pele EtnicaDocument2 pagesAdamson2017 Critica Ao Termo Pele EtnicaCristiane Leao dos SantosNo ratings yet
- Skin of Color: A Practical Guide to Dermatologic Diagnosis and TreatmentFrom EverandSkin of Color: A Practical Guide to Dermatologic Diagnosis and TreatmentNo ratings yet
- Melanocytic Lesions: A Case Based ApproachFrom EverandMelanocytic Lesions: A Case Based ApproachMai P. HoangNo ratings yet
- Basal Cell Carcinoma: Advances in Treatment and ResearchFrom EverandBasal Cell Carcinoma: Advances in Treatment and ResearchMichael R. MigdenNo ratings yet
- The Evolution of Aesthetic Medicine: The Evolution of a New Field of Medicine by a Pioneer Voted the Top Aesthetic Doctor in the WorldFrom EverandThe Evolution of Aesthetic Medicine: The Evolution of a New Field of Medicine by a Pioneer Voted the Top Aesthetic Doctor in the WorldNo ratings yet
- Collection Review Men S Key Items A W 21 22 Cut SewDocument10 pagesCollection Review Men S Key Items A W 21 22 Cut SewRitu JainNo ratings yet
- Lab - Fossil EvidenceDocument3 pagesLab - Fossil Evidenceapi-223694170No ratings yet
- Infotech JS2 Eclass Computer VirusDocument2 pagesInfotech JS2 Eclass Computer VirusMaria ElizabethNo ratings yet
- Monitoring Tool For Functional School ClinicDocument5 pagesMonitoring Tool For Functional School ClinicYatts De La Cuesta100% (1)
- Addons Free Part 1Document2 pagesAddons Free Part 1Alfa RebornNo ratings yet
- JMC GeometryDocument3 pagesJMC GeometryV HNo ratings yet
- Glenda Gloria Media in The PhilippinesDocument6 pagesGlenda Gloria Media in The PhilippinesHappy Jayson Mondragon100% (1)
- MCQ On Rural MarketingDocument28 pagesMCQ On Rural Marketingjaitripathi26No ratings yet
- Die Bosch ABS The World's First System For Closed-Loop Control of Vehicle DynamicsDocument27 pagesDie Bosch ABS The World's First System For Closed-Loop Control of Vehicle DynamicsMamdouhAlhanafy100% (1)
- DVB RodmDocument2 pagesDVB RodmAnanda BhattacharyyaNo ratings yet
- 5 Irver Punhab & OdishaDocument19 pages5 Irver Punhab & OdishasanchitNo ratings yet
- Qualities of Good Measuring InstrumentsDocument4 pagesQualities of Good Measuring InstrumentsMaricar Dela Peña56% (9)
- OS8 Gap AnalysisDocument3 pagesOS8 Gap AnalysisMihaela MikaNo ratings yet
- GoogleDocument1 pageGooglegilbertoNo ratings yet
- Co2 04Document16 pagesCo2 04Poojitha BondalapatiNo ratings yet
- Dokumen 2Document1 pageDokumen 2Balamurugan HNo ratings yet
- Quantum Materials Science EngineeringDocument2 pagesQuantum Materials Science Engineeringvisheshp961No ratings yet
- A Study of Arthur HoneggerDocument6 pagesA Study of Arthur Honeggermmarriuss7100% (1)
- Lesson 2. The Tourist Market and SegmentationDocument13 pagesLesson 2. The Tourist Market and SegmentationDonna BanuagNo ratings yet
- GenMath 1st Exam 2018Document6 pagesGenMath 1st Exam 2018Dodong PantinopleNo ratings yet
- ECON198 Module 1Document4 pagesECON198 Module 1Kevin BelloNo ratings yet
- Big Radiant Pointed Siar AfghanDocument4 pagesBig Radiant Pointed Siar AfghanbyronNo ratings yet
- Wiley - Modern Thermodynamics - From Heat Engines To Dissipative Structures, 2nd Edition - 978-1-118-37181-7Document2 pagesWiley - Modern Thermodynamics - From Heat Engines To Dissipative Structures, 2nd Edition - 978-1-118-37181-7JubairAhmedNo ratings yet
- ScriptDocument1 pageScriptstar trendzNo ratings yet
- Part 1.2. Back PropagationDocument30 pagesPart 1.2. Back PropagationViệt HoàngNo ratings yet
- Econometrics QP CalicutDocument17 pagesEconometrics QP CalicutMadonaNo ratings yet