Download as pptx, pdf, or txt
You might also like
- Presence of Scabies As A Health DeficitDocument4 pagesPresence of Scabies As A Health DeficitLemuel Glenn Bautista100% (9)
- TMJ PPT 130516130311 Phpapp02Document120 pagesTMJ PPT 130516130311 Phpapp02Hoang Nhan100% (1)
- TMJ WordDocument21 pagesTMJ WordBharathi GudapatiNo ratings yet
- TMJ SeminarDocument100 pagesTMJ SeminarMithileshwari Patil100% (1)
- TMJ AnatomyDocument39 pagesTMJ AnatomyPravallika ManneNo ratings yet
- Temporo Mandibular JointDocument60 pagesTemporo Mandibular JointchaitreeNo ratings yet
- Biomechanics of Temporomandibular Joint and Cervical SpineDocument60 pagesBiomechanics of Temporomandibular Joint and Cervical SpineRitika SonyNo ratings yet
- TMJDocument40 pagesTMJARIF PUJI LAKSONONo ratings yet
- TMJ Anatomy - OrthoDocument85 pagesTMJ Anatomy - Orthosamar yousif mohamedNo ratings yet
- Biomechanics of Temporomandibular JointDocument87 pagesBiomechanics of Temporomandibular JointseemaNo ratings yet
- TMJ and Muscles of MasticatoryDocument9 pagesTMJ and Muscles of MasticatoryFatima MartinezNo ratings yet
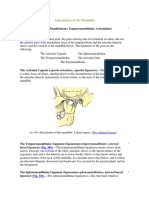
- The Articulation of The MandibleDocument4 pagesThe Articulation of The Mandibleviorel79No ratings yet
- TMJ Disorders 1Document7 pagesTMJ Disorders 1Negin HekmatjooNo ratings yet
- Temporomandibular Joint and Muscles of Mastication: ContentsDocument38 pagesTemporomandibular Joint and Muscles of Mastication: ContentsDan 04No ratings yet
- Tempromanndibular JointDocument10 pagesTempromanndibular Jointehab radmanNo ratings yet
- TMJ Seminar FinalDocument135 pagesTMJ Seminar FinalrayaimNo ratings yet
- TMJ Surgical Anatomy and ApproachesDocument165 pagesTMJ Surgical Anatomy and Approachesmohammad ghouseNo ratings yet
- Lec: TMJ DR - Nawres BahaaDocument13 pagesLec: TMJ DR - Nawres BahaaMarwa AlfuaadiNo ratings yet
- Lec 35Document10 pagesLec 35محمد جاسم محمد عجاجNo ratings yet
- Anatomy and Bio Mechanics of The TMJDocument41 pagesAnatomy and Bio Mechanics of The TMJUmair KhanNo ratings yet
- I.T.S Dental College, Greater Noida: FacultyDocument70 pagesI.T.S Dental College, Greater Noida: FacultyAMIT GUPTANo ratings yet
- Temporomandibular JointDocument86 pagesTemporomandibular Jointdrpankajaapaliya100% (2)
- s2 TMJDocument58 pagess2 TMJShilpa SomanNo ratings yet
- Makalah ModulDocument55 pagesMakalah ModulVirena GunawanNo ratings yet
- Functional Anatomy of Temporomandibular JointDocument44 pagesFunctional Anatomy of Temporomandibular JointRomzi Hanif0% (1)
- Temporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyDocument60 pagesTemporomandibular Joint: DR Bhaumik Thakkar MDS-Part 1. Dept. of Periodontology and ImplantologyJoseph Eduardo Villar CordovaNo ratings yet
- Temporo: MandibularDocument38 pagesTemporo: MandibularyomanNo ratings yet
- Anatomy of Temporomandibular Joint: Presented byDocument124 pagesAnatomy of Temporomandibular Joint: Presented bylkjhgfdsalkNo ratings yet
- TMJ AnatomiDocument53 pagesTMJ AnatomiNiTa DöéMy HarDianaNo ratings yet
- Tempero Mandibular JointDocument30 pagesTempero Mandibular JointAkash AmbhoreNo ratings yet
- 5 Relevant AnatomyDocument41 pages5 Relevant AnatomyKrupali JainNo ratings yet
- Temporomandibular JointDocument78 pagesTemporomandibular JointJoachimNo ratings yet
- Interchondral LigamentsDocument8 pagesInterchondral LigamentsAlina MoiseNo ratings yet
- Classification of JointsDocument13 pagesClassification of JointsRajat NangiaNo ratings yet
- Temporomandibular JointDocument15 pagesTemporomandibular Jointwasim hussainNo ratings yet
- TMJOH محولDocument8 pagesTMJOH محولSafura IjazNo ratings yet
- Surgical Anatomy of TMJDocument79 pagesSurgical Anatomy of TMJAditi RapriyaNo ratings yet
- Mandibular MovementsDocument36 pagesMandibular MovementsRagini ShravanNo ratings yet
- Functional Anatomy of TMJDocument20 pagesFunctional Anatomy of TMJKathrina FelicianoNo ratings yet
- Femerotibial JointDocument58 pagesFemerotibial JointGalaxyNo ratings yet
- TMJ PrintDocument135 pagesTMJ PrintAsmaa RagabNo ratings yet
- Mandibular MovementDocument56 pagesMandibular MovementSahana RangarajanNo ratings yet
- Temporomandibular Joint-Anatomy and Movement Disorders: ISSN: 2278 - 0211 (Online)Document12 pagesTemporomandibular Joint-Anatomy and Movement Disorders: ISSN: 2278 - 0211 (Online)Krupali JainNo ratings yet
- TMJ & Its MovementsDocument26 pagesTMJ & Its Movementsdeepinder27100% (1)
- TMJ CompleteDocument54 pagesTMJ CompleteNeal Torwane100% (3)
- Temporomandibular Joint: Joan S. SantosDocument9 pagesTemporomandibular Joint: Joan S. SantosVarenLagartoNo ratings yet
- TMJ Part 2Document31 pagesTMJ Part 2api-324160601No ratings yet
- Section I #18 The Temporomandibular JointDocument3 pagesSection I #18 The Temporomandibular JointInnocent L NdambakuwaNo ratings yet
- JOINTS of Neck and TMJ BdsDocument17 pagesJOINTS of Neck and TMJ BdsGanapathyGaneshNo ratings yet
- Dr. Dinesh Kumar Yadav, KDCHDocument56 pagesDr. Dinesh Kumar Yadav, KDCHDinesh Kr. YadavNo ratings yet
- TMJ Part 1Document25 pagesTMJ Part 1api-324160601No ratings yet
- Knee 05102018Document24 pagesKnee 05102018Dk KNo ratings yet
- Functional Anatomy and TMJ PathologyDocument15 pagesFunctional Anatomy and TMJ PathologyJASPREETKAUR0410100% (1)
- Anatomy of Temporomandibular JointDocument36 pagesAnatomy of Temporomandibular JointMELYANA_WANTINo ratings yet
- Functional Anatomy of Temporomandibular JointDocument46 pagesFunctional Anatomy of Temporomandibular JointSiddharth Sharma100% (2)
- Temperomandibular JointDocument17 pagesTemperomandibular JointBlack QueenNo ratings yet
- TMJ - Lec8Document10 pagesTMJ - Lec8A.A. HusseinNo ratings yet
- CFF II: Exam 1 GuideDocument25 pagesCFF II: Exam 1 GuideHilary MelloNo ratings yet
- TMJ Anatomy and DisorderDocument163 pagesTMJ Anatomy and DisorderArshdeep KaurNo ratings yet
- Di̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2Document67 pagesDi̇z Eklemi̇ni̇n Anatomi̇si̇ Ve Bi̇yomekani̇ği̇ - Bau (1) - 2erfan mohammadiNo ratings yet
- Encyclopaedia Britannica, 11th Edition, Volume 15, Slice 5 "Joints" to "Justinian I."From EverandEncyclopaedia Britannica, 11th Edition, Volume 15, Slice 5 "Joints" to "Justinian I."No ratings yet
- DLL Mapeh-1 Q1 W3Document5 pagesDLL Mapeh-1 Q1 W3Melody FullerNo ratings yet
- Tower Crane SketchDocument20 pagesTower Crane SketchShafiqNo ratings yet
- BC-2800 Operation Maunal (2.0) PDFDocument286 pagesBC-2800 Operation Maunal (2.0) PDFdanaydayi100% (3)
- Introduction To Understanding The SelfDocument44 pagesIntroduction To Understanding The SelfraffyNo ratings yet
- Interview For DomRAC TechnicianDocument5 pagesInterview For DomRAC TechnicianAldrine LatorreNo ratings yet
- Workshop Block: Section B B'Document1 pageWorkshop Block: Section B B'Aditya KapoorNo ratings yet
- Factsheet The Later Stages of DementiaDocument20 pagesFactsheet The Later Stages of DementiaMspamNo ratings yet
- R17 RoboticsDocument346 pagesR17 Roboticskiran babuNo ratings yet
- Video and Imaging Solutions GuideDocument61 pagesVideo and Imaging Solutions GuideHemantkumar100% (1)
- Jeppview For Windows: List of Pages in This Trip KitDocument100 pagesJeppview For Windows: List of Pages in This Trip KitSantiagoPalmaBenitez0% (1)
- Aviation Security Assignment 3Document5 pagesAviation Security Assignment 3Yousef Al HashemiNo ratings yet
- Disaster Management in Indian Railways: (Para 1.10.1)Document33 pagesDisaster Management in Indian Railways: (Para 1.10.1)lvsaruNo ratings yet
- DFT Study of CO2 and H2O Co-Adsorption On CarbonDocument17 pagesDFT Study of CO2 and H2O Co-Adsorption On CarbonRafael Ricardo Celin ManceraNo ratings yet
- MFC-151 Manual enDocument11 pagesMFC-151 Manual enathanasiosNo ratings yet
- Diagnosis and Screening of Brugada SyndromeDocument11 pagesDiagnosis and Screening of Brugada SyndromeWinardi NursyidahNo ratings yet
- Timothy Morton - Ecology Without Nature - Rethinking Environmental Aesthetics (2009)Document131 pagesTimothy Morton - Ecology Without Nature - Rethinking Environmental Aesthetics (2009)ilduNo ratings yet
- Cooling Load Calculation Through Transmission and ProductDocument4 pagesCooling Load Calculation Through Transmission and ProductKenneth CariñoNo ratings yet
- AQUASILVICULTUREDocument2 pagesAQUASILVICULTUREjun rey tingcangNo ratings yet
- RP 30 2 Selection and Use of Measurement InstrumentDocument212 pagesRP 30 2 Selection and Use of Measurement Instrumentmohammed el erianNo ratings yet
- Style Guidelines - Powered by GameSparks PDFDocument20 pagesStyle Guidelines - Powered by GameSparks PDFJosé María RomeroNo ratings yet
- Operator's Manual - 6'' Echo Sounder - LS-6100Document47 pagesOperator's Manual - 6'' Echo Sounder - LS-6100Adeilson AlmoaiaNo ratings yet
- Receiver Mounted Motorcycle Carrier: Set Up and Operating InstructionsDocument8 pagesReceiver Mounted Motorcycle Carrier: Set Up and Operating InstructionsVeljko KercevicNo ratings yet
- Girimananda SuttaDocument22 pagesGirimananda SuttaBuddhist Publication SocietyNo ratings yet
- Data Sheet: DEGALAN® LP 64/12Document2 pagesData Sheet: DEGALAN® LP 64/12Akhtar aliNo ratings yet
- 2017 Fall ME501 06 VectorCalculusDocument95 pages2017 Fall ME501 06 VectorCalculusAfaq AhmedNo ratings yet
- JACM - Volume 1 - Issue 1 - Pages 10-16Document7 pagesJACM - Volume 1 - Issue 1 - Pages 10-16Raksha AroraNo ratings yet
- Development StudiesDocument28 pagesDevelopment Studiesaegis0667% (3)
- (SOSC1960) (2012) (S) Quiz - jqj28 97890Document3 pages(SOSC1960) (2012) (S) Quiz - jqj28 97890alex61937No ratings yet
- All Days Are Sacred (Fakayode)Document63 pagesAll Days Are Sacred (Fakayode)Lucas Rachid100% (10)