Download as ppt, pdf, or txt
You might also like
- BioWorkbook1A Ans eDocument38 pagesBioWorkbook1A Ans eCindy Cheung50% (2)
- Differential Diagnosis of JaundiceDocument4 pagesDifferential Diagnosis of JaundiceVirag PatilNo ratings yet
- Urine Examination New-1Document81 pagesUrine Examination New-1H GondaliyaNo ratings yet
- Urine AnalysisDocument69 pagesUrine Analysisvinay0717100% (3)
- 6 BodyDocument110 pages6 Bodysinte beyuNo ratings yet
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Analysis of Abnormal Urine NotesDocument6 pagesAnalysis of Abnormal Urine Notesahteshammirji575No ratings yet
- Urine Analysis and BiuretDocument30 pagesUrine Analysis and BiuretTom Anthony TonguiaNo ratings yet
- Urine Dipstick Testing + Common Renal Problem 2012Document52 pagesUrine Dipstick Testing + Common Renal Problem 2012Ainul ArinaNo ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
- Metab DisordersDocument36 pagesMetab DisordersDaena TimtimanNo ratings yet
- CM Lec Chemical Examination of UrineDocument50 pagesCM Lec Chemical Examination of UrineThea MallariNo ratings yet
- Renal Function Tests - Final VersionDocument80 pagesRenal Function Tests - Final Versionmikky8204No ratings yet
- Analysis of Abnormal UrineDocument12 pagesAnalysis of Abnormal Urinesingonstrings365No ratings yet
- Clin Path Trans 3.05 Urinalysis (2b)Document6 pagesClin Path Trans 3.05 Urinalysis (2b)Reymart FernandezNo ratings yet
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNo ratings yet
- Urine JSJ EoDocument9 pagesUrine JSJ EokeiNo ratings yet
- Rine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al MaqadmaDocument39 pagesRine Analysis: Dr. Ola Samir Ziara Modified by Dr. Amal Al Maqadmaiman zainuddin100% (1)
- UMY BLOK 12 LIVER RENAL FUNCTION TEST 30 Maret 2020 SENTDocument41 pagesUMY BLOK 12 LIVER RENAL FUNCTION TEST 30 Maret 2020 SENTellaNo ratings yet
- REVIEW 2023 AUBF Basics On Chemical Tests For UrineDocument84 pagesREVIEW 2023 AUBF Basics On Chemical Tests For UrineJheshari VinaNo ratings yet
- Abnormal Constituents of UrineDocument7 pagesAbnormal Constituents of UrineAnjuNo ratings yet
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarNo ratings yet
- Urinalysis PDFDocument56 pagesUrinalysis PDFTio AjhaNo ratings yet
- Term III Practical FileDocument31 pagesTerm III Practical FileShivam kumarNo ratings yet
- Urine AnalysisDocument42 pagesUrine AnalysisajaysomNo ratings yet
- Biochemistry of Urine: By: Jerome S. Montano, RMTDocument28 pagesBiochemistry of Urine: By: Jerome S. Montano, RMTAhuNo ratings yet
- Metabolic DisordersDocument59 pagesMetabolic DisordersKeannu Havana100% (1)
- 06 ABNORMAL CONSTITUENTS OF URINEDocument4 pages06 ABNORMAL CONSTITUENTS OF URINErohannmandela0987No ratings yet
- Routine Examination of Urine AND It'S InterpretationDocument64 pagesRoutine Examination of Urine AND It'S InterpretationmeherulafmcNo ratings yet
- Obstructive Jaundice Group 6Document33 pagesObstructive Jaundice Group 6Qurbon AliNo ratings yet
- Liver Function TestDocument17 pagesLiver Function TestKarthiyayini .S.JNo ratings yet
- Urine Screening For Metabolic DisordersDocument55 pagesUrine Screening For Metabolic DisordersGlormina Asprec AvenaNo ratings yet
- Chemical Examination of UrineDocument46 pagesChemical Examination of Urineubaidnaveed0323No ratings yet
- Mbbs 2k23 Aim - To Identify The Abnormal Constitutes of UrineDocument22 pagesMbbs 2k23 Aim - To Identify The Abnormal Constitutes of Urine8harshul8No ratings yet
- Urine ComponentsDocument31 pagesUrine ComponentsLarry MagwegweNo ratings yet
- Kidney Function Tests 2Document30 pagesKidney Function Tests 2kamalNo ratings yet
- Kidney Function Tests2012Document32 pagesKidney Function Tests2012Dratosh KatiyarNo ratings yet
- Urinalysis TableDocument9 pagesUrinalysis TableMegNo ratings yet
- FECALYSISDocument13 pagesFECALYSISXyleene Jency Bien IINo ratings yet
- Somaville University Faculty of Medicine Urology &nephrology Lecturer: DR - Osman Urine Analyze Presentation by Group ADocument49 pagesSomaville University Faculty of Medicine Urology &nephrology Lecturer: DR - Osman Urine Analyze Presentation by Group ALayla CabduqaadirNo ratings yet
- Introduction To UrinalysisDocument5 pagesIntroduction To UrinalysisseanleeqtNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- Urine Analysis: Dr. Janani MathialaganDocument67 pagesUrine Analysis: Dr. Janani MathialaganGunjan sahuNo ratings yet
- Characteristics of UrineDocument32 pagesCharacteristics of UrineMEGHANA GOSWAMINo ratings yet
- URINALYSISDocument63 pagesURINALYSISMedah Naserian100% (2)
- 1 - GueDocument24 pages1 - GueQasmNo ratings yet
- Renal Function Tests 2-25459Document40 pagesRenal Function Tests 2-25459nirajNo ratings yet
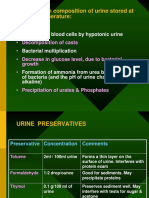
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Urineanalysis 1Document88 pagesUrineanalysis 1sohamdasofficial02No ratings yet
- Renal Function TestsDocument36 pagesRenal Function TestsLawal Bello DanchadiNo ratings yet
- Pathological Urine: Physical Examination of UrineDocument8 pagesPathological Urine: Physical Examination of UrineOLUWASEGUN K AfolabiNo ratings yet
- OUM Tutorial 1 SBNS3504 RenalDocument51 pagesOUM Tutorial 1 SBNS3504 RenalMashanimy HoneyNo ratings yet
- UrinalysisDocument3 pagesUrinalysisKim MoranoNo ratings yet
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomNo ratings yet
- Chemical Examination of UrineDocument32 pagesChemical Examination of UrineMarti DeaneNo ratings yet
- Abnormal UrineDocument28 pagesAbnormal UrinemujeebNo ratings yet
- Kidney Function TestsDocument50 pagesKidney Function TestsStephen Fritz OreNo ratings yet
- Examination of Body Fluids (Urinalysis)Document109 pagesExamination of Body Fluids (Urinalysis)kiedd_04100% (9)
- Diabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandDiabetic Nephropathy, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- Diabetic Recipes for One and TwoFrom EverandDiabetic Recipes for One and TwoRating: 3 out of 5 stars3/5 (1)
- Dairy Cattle NutritionDocument42 pagesDairy Cattle NutritionDrachir Crausus100% (3)
- Biology 11 BODY SYSTEMSDocument13 pagesBiology 11 BODY SYSTEMSkatwal09No ratings yet
- GIT Mcqs by DR Elsayed EmaraDocument13 pagesGIT Mcqs by DR Elsayed EmaraHasen umerNo ratings yet
- Test Questions Internal MedicineDocument13 pagesTest Questions Internal MedicineJo Anne86% (7)
- Signs and Symptoms of Pancreatic Cancer Fact Sheet Dec 2014Document6 pagesSigns and Symptoms of Pancreatic Cancer Fact Sheet Dec 2014Nus EuNo ratings yet
- Ghadi BCS 4 DrugsDocument25 pagesGhadi BCS 4 Drugsumamaheswararao4No ratings yet
- Digestive System of PoultryDocument6 pagesDigestive System of PoultryNirjonSarker100% (1)
- Table e - Liver Anatomy Biliary SystemDocument11 pagesTable e - Liver Anatomy Biliary Systemapi-371971600No ratings yet
- Case Presentation On CholelithiasisDocument24 pagesCase Presentation On CholelithiasisLouie Kem Anthony Babaran100% (1)
- Yellow Bellied Slider TurtleDocument6 pagesYellow Bellied Slider TurtleSky Kristen DrerupNo ratings yet
- Cirrhosis of The Liver Nursing Care Management Symptoms NCLEXDocument10 pagesCirrhosis of The Liver Nursing Care Management Symptoms NCLEXParallelNo ratings yet
- Chapter 3 NutritionDocument10 pagesChapter 3 NutritionCHONG KOK HINNo ratings yet
- Biliary AtresiaDocument13 pagesBiliary AtresiaGündüz AğayevNo ratings yet
- Cholelithiasis - 4th Class Binita DasDocument13 pagesCholelithiasis - 4th Class Binita DasRanjit SahNo ratings yet
- Digestive SystemDocument6 pagesDigestive SystemCeleste Atienza BawagNo ratings yet
- Bio Assessment 1 Term 1Document6 pagesBio Assessment 1 Term 1turirirNo ratings yet
- 1.1 - Life ProcesDocument26 pages1.1 - Life Procesvivek tripathiNo ratings yet
- Anatomy &physiology JaundiceDocument2 pagesAnatomy &physiology JaundiceHCX dghhqNo ratings yet
- Standard ProcessDocument10 pagesStandard ProcessWallace VargasNo ratings yet
- Sklera Sub IkterikDocument7 pagesSklera Sub IkterikFauziah_Hannum_SNo ratings yet
- Digestion Activity SheetDocument5 pagesDigestion Activity SheetMarvin CincoNo ratings yet
- Radiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDocument100 pagesRadiology Examination For Tractus Digestivus Chairunnisa, Dr. SP - RadDiana OCtavinaNo ratings yet
- Gallbladder, Liver, Pancreas and SpleenDocument19 pagesGallbladder, Liver, Pancreas and Spleensarguss14100% (3)
- 7-Bilirubin MetabolismDocument19 pages7-Bilirubin MetabolismMarie Bernadette Digo100% (1)
- Cardiovascular System BloodDocument85 pagesCardiovascular System BloodEbrahem ShaheinNo ratings yet
- Flattened 21Document52 pagesFlattened 21IMAFDNo ratings yet
- Veterinary Histology Lecture NotesDocument62 pagesVeterinary Histology Lecture NotesDEV3LLS100% (3)
- Class 7, CH 2 Nutrition in AnimalsDocument4 pagesClass 7, CH 2 Nutrition in AnimalsAkkshara Kashyap 7-HNo ratings yet
- Anatomy and Physiology - GallbladderDocument2 pagesAnatomy and Physiology - GallbladderCHi NAiNo ratings yet