Download as ppt, pdf, or txt
You might also like
- All On 4Document50 pagesAll On 4Juan Jose Stuven RodriguezNo ratings yet
- Bitewing and Occlusal 2021Document47 pagesBitewing and Occlusal 2021Khadyjah RashidNo ratings yet
- Intraoral Radiographic ExaminationDocument79 pagesIntraoral Radiographic Examinationغلاها عبدوNo ratings yet
- Occlusal RadiografiDocument8 pagesOcclusal RadiografiFatma MahechiNo ratings yet
- Intraoral Radiographic TechniqueDocument29 pagesIntraoral Radiographic Techniqueabdullah aliNo ratings yet
- Periapical RadiographDocument4 pagesPeriapical RadiographAnggreta AuriadiniNo ratings yet
- Intraoral 20radiographic 20technique 20ii 140507115114 Phpapp02Document60 pagesIntraoral 20radiographic 20technique 20ii 140507115114 Phpapp02An AnNo ratings yet
- Intraoral Radiographic Technique IiDocument50 pagesIntraoral Radiographic Technique IiAn AnNo ratings yet
- Kashvee Vashishtha (BDS 3rd Year)Document15 pagesKashvee Vashishtha (BDS 3rd Year)pooja sharmaNo ratings yet
- Radiographic Technique of The BisectrizDocument72 pagesRadiographic Technique of The BisectrizScribdTranslationsNo ratings yet
- Intraoral Projection and Quality Evaluation - Kel 1Document35 pagesIntraoral Projection and Quality Evaluation - Kel 1alzayyanauroraNo ratings yet
- Intraoral Periapical Radiographic Techniques: Second Academic Year DENT214Document116 pagesIntraoral Periapical Radiographic Techniques: Second Academic Year DENT2143bdullah al3yuni100% (1)
- Radiography Bisecting AngleDocument17 pagesRadiography Bisecting Anglerabee_tomehNo ratings yet
- Need of Lntraoral Periapical Radiographs: 5. Post Extraction Radiographs For Root Fragments and Other Co-Lateral DamagesDocument6 pagesNeed of Lntraoral Periapical Radiographs: 5. Post Extraction Radiographs For Root Fragments and Other Co-Lateral DamagesRifky Al ThariqNo ratings yet
- Occlusal RadDocument3 pagesOcclusal RadAhmedFouadNo ratings yet
- Panoramic RadiographyDocument52 pagesPanoramic RadiographyPuspita Wulansari100% (1)
- Chapter 16 - Oral Radiography (Essentials of Dental Assisting)Document96 pagesChapter 16 - Oral Radiography (Essentials of Dental Assisting)mussanteNo ratings yet
- OcclusalDocument10 pagesOcclusalFATIHAH SYAFINAZ BINTI KAMARUL ZAMANNo ratings yet
- DA220 Ch1Document32 pagesDA220 Ch1Anne DavisNo ratings yet
- Successful Panoramic Radiography PDFDocument27 pagesSuccessful Panoramic Radiography PDFDivyanshBansalNo ratings yet
- Intraoral Radiographic Pararel and Bitewing 2015Document54 pagesIntraoral Radiographic Pararel and Bitewing 2015EuginiaNo ratings yet
- Cephalometric SrachaelDocument130 pagesCephalometric Srachaelابو العزNo ratings yet
- Intraoral Radiographic Techniques ǁ: by Dr. WajnaaDocument32 pagesIntraoral Radiographic Techniques ǁ: by Dr. WajnaaALI abd-alamamNo ratings yet
- Cieszynski' Rule of IsometryDocument5 pagesCieszynski' Rule of Isometrynishant_tewari_1No ratings yet
- Intra-Oral Radio Graphs For The Pediatric Dental Patient PedoDocument44 pagesIntra-Oral Radio Graphs For The Pediatric Dental Patient PedoFourthMolar.comNo ratings yet
- Radiology Practical PartDocument75 pagesRadiology Practical PartLisa FUzelieNo ratings yet
- Vertical and Horizontal AngulationDocument7 pagesVertical and Horizontal Angulationjoanadiasalves1234No ratings yet
- 4 Intraoral Radiographic TechniquesDocument35 pages4 Intraoral Radiographic TechniquesDan 04100% (1)
- Canine Dental Radiology - Radiographic Technic, Development, and Anatomy of The TeethDocument9 pagesCanine Dental Radiology - Radiographic Technic, Development, and Anatomy of The TeethFernanda PérezNo ratings yet
- Bitewing RadiographyDocument20 pagesBitewing Radiographyanon_66676758No ratings yet
- Schropp Et Al (2005) Immediate Vs Delayed IJOMI PDFDocument9 pagesSchropp Et Al (2005) Immediate Vs Delayed IJOMI PDFAlla MushkeyNo ratings yet
- Schropp Et Al (2005) Immediate Vs Delayed IJOMIDocument9 pagesSchropp Et Al (2005) Immediate Vs Delayed IJOMIAlla MushkeyNo ratings yet
- Intraoral ProjectionsDocument73 pagesIntraoral ProjectionsrespikNo ratings yet
- Tilted or Parallel Implant Placement inDocument7 pagesTilted or Parallel Implant Placement in朱嘉琪No ratings yet
- Mermigos 11 01Document4 pagesMermigos 11 01Sankurnia HariwijayadiNo ratings yet
- Radiology in Pediatric Dentistry 2Document44 pagesRadiology in Pediatric Dentistry 2Aima Cuba100% (1)
- Bitewing Radiography PDFDocument39 pagesBitewing Radiography PDFMarianaBsvNo ratings yet
- Partial Odontectomy 2007Document7 pagesPartial Odontectomy 2007Yoga ChrisnugrohoNo ratings yet
- Panoramic Imaging & Cone Beam Computed TomographyDocument54 pagesPanoramic Imaging & Cone Beam Computed TomographyMenna KhNo ratings yet
- Radio Graphic Techniques-Bisecting and OcclusalDocument66 pagesRadio Graphic Techniques-Bisecting and OcclusalFourthMolar.comNo ratings yet
- Cephalometric Radiography 101Document48 pagesCephalometric Radiography 101Rabeea KittaniNo ratings yet
- Self Study Bisecting Occlusal RX TechniqueDocument64 pagesSelf Study Bisecting Occlusal RX TechniqueMihnea BuiaNo ratings yet
- RadiologyDocument55 pagesRadiologySuganya MurugaiahNo ratings yet
- Management of Impacted Canine1Document88 pagesManagement of Impacted Canine1Saumya Singh100% (1)
- Lec 8 Cep Halo MetricDocument12 pagesLec 8 Cep Halo MetricHuda AljaderiNo ratings yet
- Endodontic Radiography Lec.18: Al-Mustansiriya University College of Dentistry Endodontics LecturesDocument9 pagesEndodontic Radiography Lec.18: Al-Mustansiriya University College of Dentistry Endodontics Lecturesmariamalobeidi53No ratings yet
- 2005 Laster Width Distraction OsteogenesisDocument7 pages2005 Laster Width Distraction Osteogenesislisal1saNo ratings yet
- Shetye 2017Document7 pagesShetye 2017Evgeniya KocherginaNo ratings yet
- Dental Radiology Related To Pedodontics: Dept. of Pediatric & Preventive DentistryDocument43 pagesDental Radiology Related To Pedodontics: Dept. of Pediatric & Preventive DentistryHebah NawafNo ratings yet
- Extraoral 2018Document14 pagesExtraoral 2018sanyengereNo ratings yet
- Lee2016 Usar EsseDocument9 pagesLee2016 Usar EsseMr OdontologiaNo ratings yet
- 10 1111@edt 12575Document44 pages10 1111@edt 12575gbaez.88No ratings yet
- Intraoral Tech عمليDocument28 pagesIntraoral Tech عمليAbdullah EmadNo ratings yet
- Bisecting and Parelling TechniqueDocument32 pagesBisecting and Parelling TechniqueArka Saha100% (1)
- X-Ray: Oral Radiographic Techniques: - IntraDocument21 pagesX-Ray: Oral Radiographic Techniques: - Intraمحمد عماد علي احمدNo ratings yet
- PanoramikDocument38 pagesPanoramikStephanie Victoria100% (1)
- CH 50Document19 pagesCH 502oclockNo ratings yet
- Impacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFDocument13 pagesImpacted Maxillary Canines-A Review. - American Journal of Orthodontics and Dentofacial Orthopedics, 101-159, 1992 PDFPia ContrerasNo ratings yet
- Fundamentals of Oral and Maxillofacial RadiologyFrom EverandFundamentals of Oral and Maxillofacial RadiologyRating: 4 out of 5 stars4/5 (1)
- Manual 2 PDFDocument442 pagesManual 2 PDFSebastian CoraisacaNo ratings yet
- Presentation 2Document5 pagesPresentation 2TechLakeNo ratings yet
- Raising Permit: Office of The Building OfficialDocument2 pagesRaising Permit: Office of The Building OfficialJc JüsäyänNo ratings yet
- Seal Gas FlowDocument2 pagesSeal Gas FlowoluwasolNo ratings yet
- Learning & Teaching MethodologyDocument17 pagesLearning & Teaching MethodologyVaidya Gautham M33% (6)
- Embedded Controlled Drip Irrigation SystemDocument5 pagesEmbedded Controlled Drip Irrigation SystemInternational Journal of Application or Innovation in Engineering & ManagementNo ratings yet
- Missing Women of PartitionDocument30 pagesMissing Women of PartitionSaya Augustin100% (1)
- Coitus ReservatusDocument4 pagesCoitus ReservatusTrà Thanh NguyễnNo ratings yet
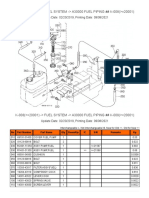
- K-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Document2 pagesK-008 ( 20001) - Fuel System - A30000 Fuel Piping ## K-008 ( 20001)Martin LindbergNo ratings yet
- Application FormDocument8 pagesApplication FormCrystal KleistNo ratings yet
- Ctu (Zuuu) PDFDocument45 pagesCtu (Zuuu) PDFchang woo yunNo ratings yet
- Combined Cellulitis - FinalDocument78 pagesCombined Cellulitis - Finalsaru_patel0% (1)
- What Are The Expected Tasks You Have Successfully AccomplishedDocument1 pageWhat Are The Expected Tasks You Have Successfully AccomplishedImmortality Realm67% (18)
- Basic Facts About ESOPs2Document20 pagesBasic Facts About ESOPs2Quant TradingNo ratings yet
- Transverse Lie : Predisposing Factors, Maternal and Perinatal OutcomeDocument4 pagesTransverse Lie : Predisposing Factors, Maternal and Perinatal OutcomeErlangga DayudNo ratings yet
- Exercise 4:: Organic Components: CarbohydratesDocument20 pagesExercise 4:: Organic Components: CarbohydratespikachuzingungaNo ratings yet
- Nursing Care PlanDocument8 pagesNursing Care Planalexander abasNo ratings yet
- LV Panel ReportDocument71 pagesLV Panel ReportMudassirNo ratings yet
- TirupathiDocument14 pagesTirupathiEkta Adlakha100% (1)
- Interactive Schematic: This Document Is Best Viewed at A Screen Resolution of 1024 X 768Document13 pagesInteractive Schematic: This Document Is Best Viewed at A Screen Resolution of 1024 X 768maquinariakypcon100% (2)
- نموذج ميزانية تدريبDocument2 pagesنموذج ميزانية تدريبعمولةNo ratings yet
- Beer & Wine Osd PresDocument18 pagesBeer & Wine Osd PresAnand100% (1)
- Chemistry Ibdp Exam Syle QuestionsDocument37 pagesChemistry Ibdp Exam Syle QuestionsGEORGE MATTHEWNo ratings yet
- Wastewater Characteristics: Table 7.1.5 Table 7.1.6Document4 pagesWastewater Characteristics: Table 7.1.5 Table 7.1.6Amin EnviroNo ratings yet
- Acquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingDocument3 pagesAcquaintance Games: Morning Games Team Building Activity: The Boat Is SinkingAnonymous iZJv305rNo ratings yet
- The Food Chain Consists of Four Main PartsDocument3 pagesThe Food Chain Consists of Four Main PartskoiaitraazNo ratings yet
- Chapter 2 Lesson 21 Animals That Live On LandDocument17 pagesChapter 2 Lesson 21 Animals That Live On LandRoxan S. Pumphrey0% (1)
- Acute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDocument15 pagesAcute Rheumatic Fever - Clinical Manifestations and Diagnosis - UpToDateDannyGutierrezNo ratings yet
- B 17Document15 pagesB 17Rochdi SahliNo ratings yet
- Focus Level 3 Table of Contents PDFDocument2 pagesFocus Level 3 Table of Contents PDFDaria KudosLamNo ratings yet