Download as pptx, pdf, or txt
You might also like
- Activity 3.5 Feedback Mechanisms Involved in Regulating Processes in The Female Reproductive System (Menstrual Cycle) - 084506Document1 pageActivity 3.5 Feedback Mechanisms Involved in Regulating Processes in The Female Reproductive System (Menstrual Cycle) - 084506Megan WolvesNo ratings yet
- LECTURE 1 Introduction of InfectionDocument29 pagesLECTURE 1 Introduction of Infectiontari riyastiNo ratings yet
- Lec#17+18 Adrenal DisordersDocument101 pagesLec#17+18 Adrenal DisordersKhaldoun AlmomaniNo ratings yet
- Kuliah AdrenalDocument32 pagesKuliah AdrenalNindhyana Diwaratri R100% (1)
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Diabetes IdiDocument71 pagesDiabetes IdiAriyanaNo ratings yet
- The Hepatorenal SyndromeDocument26 pagesThe Hepatorenal SyndromeWaraBawanaNo ratings yet
- EMERGENCIES IN DM (KAD Dan HHS)Document26 pagesEMERGENCIES IN DM (KAD Dan HHS)ozNo ratings yet
- Adrenal DisordersDocument32 pagesAdrenal DisordersJyoti ChadhaNo ratings yet
- Interpretasi Urine RutinDocument118 pagesInterpretasi Urine Rutinboy jendri huluNo ratings yet
- Pseudomonad GroupDocument18 pagesPseudomonad GroupNikita MarieNo ratings yet
- 2 PneumoniaDocument53 pages2 PneumoniaLucyellowOttemoesoeNo ratings yet
- Aortic Regurgitation: Chief ComplaintDocument5 pagesAortic Regurgitation: Chief Complaintdrnareshkumar3281No ratings yet
- FINAL Management Update of Hyperuricemia & GoutDocument50 pagesFINAL Management Update of Hyperuricemia & GoutNeni Septria NingsihNo ratings yet
- Management of Ankylosis Spondylitis 1Document53 pagesManagement of Ankylosis Spondylitis 1ishaan kharbandaNo ratings yet
- Irritable Bowel Syndrome (Ibs)Document9 pagesIrritable Bowel Syndrome (Ibs)EmeraldyModyNo ratings yet
- Krisis AdrenalDocument18 pagesKrisis AdrenalListya NormalitaNo ratings yet
- Peace Corps Medical AdvisoryDocument2 pagesPeace Corps Medical Advisoryanon_767403No ratings yet
- Sarcopenia and Osteoporosis-Terkunci PDFDocument33 pagesSarcopenia and Osteoporosis-Terkunci PDFNur AisyahNo ratings yet
- Metabolic Syndrome Is Related Cardio-Cerebro Vascular DiseaseDocument40 pagesMetabolic Syndrome Is Related Cardio-Cerebro Vascular DiseaseSatya FitriansyahNo ratings yet
- National Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesDocument103 pagesNational Cholesterol Education Program: Adult Treatment Panel III (ATP III) GuidelinesAdil AhmedNo ratings yet
- Geriatric Medicine KuliahDocument38 pagesGeriatric Medicine KuliahLia pramitaNo ratings yet
- 5.soap Chest PainDocument19 pages5.soap Chest PainDesiana Kemala SariNo ratings yet
- Materi Krisis Tiroid PPDSDocument10 pagesMateri Krisis Tiroid PPDSRudy Arindra WijayaNo ratings yet
- Dr. Erlieza Roosdhania, SP - PD (CKD)Document38 pagesDr. Erlieza Roosdhania, SP - PD (CKD)Pon PondNo ratings yet
- Approach To HypertensionDocument16 pagesApproach To HypertensionShradha KhuranaNo ratings yet
- Pancreatic MalignancyDocument22 pagesPancreatic Malignancylovelots1234No ratings yet
- KARDIOMYOPATI - Kuliah DR - ErlinaDocument28 pagesKARDIOMYOPATI - Kuliah DR - ErlinaArif Zulfian MubarokNo ratings yet
- Hipertensi-Krisis Dr. HendroDocument35 pagesHipertensi-Krisis Dr. Hendroyudhagp100% (1)
- Naskah Publikasi LansiaDocument17 pagesNaskah Publikasi LansiaVhiny ChaNo ratings yet
- Comprehensive Geriatric AssessmentDocument87 pagesComprehensive Geriatric AssessmentNurrahmanita AzizaNo ratings yet
- Atherosclerosis & Trombosis Dr. FaturochmanDocument50 pagesAtherosclerosis & Trombosis Dr. FaturochmanPutry RizqiaNo ratings yet
- IPDIDocument30 pagesIPDIaris budionoNo ratings yet
- Dyslipidemia Update by DR SarmaDocument96 pagesDyslipidemia Update by DR SarmaDewi NofiantiNo ratings yet
- Morning Report: August 28, 2013 Jessica Miller, MD, PGY2Document30 pagesMorning Report: August 28, 2013 Jessica Miller, MD, PGY2Emily EresumaNo ratings yet
- Diabetes Mellitus: DR Hiew Fu LiongDocument30 pagesDiabetes Mellitus: DR Hiew Fu LiongamminsaffriNo ratings yet
- Ada 2018Document174 pagesAda 2018CarlosChávezNo ratings yet
- Albumin Therapy in Clinical PracticeDocument8 pagesAlbumin Therapy in Clinical PracticeJessica AdvínculaNo ratings yet
- Renal Calculi & Renal FailureDocument17 pagesRenal Calculi & Renal Failureazlan100% (1)
- Hormon AdenohipofisisDocument44 pagesHormon AdenohipofisisIkaTriRahayuNo ratings yet
- Fluid Managementuntuk Mahasiswa SajaDocument56 pagesFluid Managementuntuk Mahasiswa SajaPratami Rieuwpassa IINo ratings yet
- Goiter and Malignant Thyroid DiseaseDocument24 pagesGoiter and Malignant Thyroid Diseaseshaza ewisNo ratings yet
- Palliative EnciesDocument96 pagesPalliative EnciesnandanNo ratings yet
- Blanko PX LAB BaruDocument2 pagesBlanko PX LAB Barupus purnamaNo ratings yet
- Advance Care Planning English VersionDocument9 pagesAdvance Care Planning English VersionAlma NurfitriaNo ratings yet
- Sign of Diseases PDFDocument5 pagesSign of Diseases PDFJagveer Chauhan100% (1)
- Protein C & S DeficiencyDocument20 pagesProtein C & S DeficiencyAhmad Ariff Azmer MunshiNo ratings yet
- TiroidDocument26 pagesTiroidJoni Riana MustaqimNo ratings yet
- Jurnal Reading Rome IVDocument31 pagesJurnal Reading Rome IVrizki febrianNo ratings yet
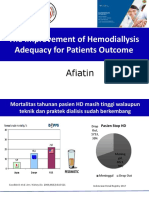
- 2.ADEKUASI KUNINGAN by DR Afiatin PDFDocument75 pages2.ADEKUASI KUNINGAN by DR Afiatin PDFrini purwantiNo ratings yet
- BPJS DMDocument28 pagesBPJS DMAdhi TjahyadiNo ratings yet
- Celiac DiseaseDocument25 pagesCeliac DiseaseMateen ShukriNo ratings yet
- INSULIN Dan Obat Hipoglikemik OralDocument35 pagesINSULIN Dan Obat Hipoglikemik OralSwietenia Rambu SabatiNo ratings yet
- Hurler Syndrome (Biochem Repot)Document5 pagesHurler Syndrome (Biochem Repot)Kristine Abegail CantillerNo ratings yet
- 03 Hiv 2012Document41 pages03 Hiv 2012Ardi SasongkoNo ratings yet
- Endo-2 Hyperprolactinemia DIDocument40 pagesEndo-2 Hyperprolactinemia DIalhusien.abd2000No ratings yet
- Addison's Disease-Dr. AM IyagbaDocument34 pagesAddison's Disease-Dr. AM IyagbaDr. Amb. Monday ZaccheausNo ratings yet
- Adrenal Disorders in ChildrenDocument50 pagesAdrenal Disorders in ChildrenadinayNo ratings yet
- 005 - Cushing SyndromeDocument51 pages005 - Cushing SyndromeLucas Victor AlmeidaNo ratings yet
- Hipotalamus-Pituitari-Sumbu Adrenal (Axis) Regulasi Sirkadian Korteks Adrenal CRH ACTHDocument9 pagesHipotalamus-Pituitari-Sumbu Adrenal (Axis) Regulasi Sirkadian Korteks Adrenal CRH ACTHAnastasia PinkyNo ratings yet
- hypothal-hypof disorders part1 - копияDocument176 pageshypothal-hypof disorders part1 - копияElena Borş MorariNo ratings yet
- DM ComplicationsDocument97 pagesDM ComplicationsElena Borş MorariNo ratings yet
- WJH 5 14Document15 pagesWJH 5 14Elena Borş MorariNo ratings yet
- DMJ 2020 0258Document17 pagesDMJ 2020 0258Elena Borş MorariNo ratings yet
- Dgaa 686Document11 pagesDgaa 686Elena Borş MorariNo ratings yet
- (26344793 - Endocrine Oncology) Dopamine Agonist Therapy For Prolactinomas - Do We Need To Rethink The Place of Surgery in Prolactinoma ManagementDocument20 pages(26344793 - Endocrine Oncology) Dopamine Agonist Therapy For Prolactinomas - Do We Need To Rethink The Place of Surgery in Prolactinoma ManagementElena Borş MorariNo ratings yet
- HipertiroidismDocument131 pagesHipertiroidismElena Borş MorariNo ratings yet
- Ijms 22 08217 v3Document18 pagesIjms 22 08217 v3Elena Borş MorariNo ratings yet
- Endocrine SystemDocument10 pagesEndocrine SystemPeej Reyes100% (1)
- Endocrine System G10Document27 pagesEndocrine System G10Cyril CauilanNo ratings yet
- BIO 282 Male Reproductive System - FINALDocument46 pagesBIO 282 Male Reproductive System - FINALLira PagaraNo ratings yet
- Role of Hormons in PregnancyDocument8 pagesRole of Hormons in PregnancyMabila apriyaniNo ratings yet
- IGCSE Bio Lesson Plan 7 Chemical CoordinationDocument2 pagesIGCSE Bio Lesson Plan 7 Chemical CoordinationHisokagenNo ratings yet
- ENG CL 900i 210285X6P 20180614 SmallDocument2 pagesENG CL 900i 210285X6P 20180614 SmallFayssal BenfoddaNo ratings yet
- Science 10 - Reproductive SystemDocument32 pagesScience 10 - Reproductive SystemHanabi Scarlet ShadowNo ratings yet
- B SRAVANI-Female16 Years-2090Document1 pageB SRAVANI-Female16 Years-2090vijaykumarNo ratings yet
- Lec 8-Endocrine SystemDocument30 pagesLec 8-Endocrine SystemHarahap DarwisNo ratings yet
- TCM Treatment of Polycystic Ovary and PCOS: Case ReportDocument5 pagesTCM Treatment of Polycystic Ovary and PCOS: Case ReportMarcin SowNo ratings yet
- NURS 406 Concept Map HyperparathyroidismDocument1 pageNURS 406 Concept Map HyperparathyroidismshyannNo ratings yet
- Addison's Disease 1Document6 pagesAddison's Disease 1Yang YangNo ratings yet
- Endoc, Pancreas, ThyroidDocument9 pagesEndoc, Pancreas, ThyroidKatrina Vianca DecapiaNo ratings yet
- BHSAgriculture - The Role of Hormones in The Regulation of Animal Reproduction and BehaviourDocument2 pagesBHSAgriculture - The Role of Hormones in The Regulation of Animal Reproduction and BehaviourzuhaibNo ratings yet
- SEP Enabling Assessment 3 Integumentary System of Vertebrates (1) - 1Document5 pagesSEP Enabling Assessment 3 Integumentary System of Vertebrates (1) - 1Francesca Nicole0% (1)
- PHYSIOLOGICAL CHANGES DURING PREGNANCY1may 20222Document12 pagesPHYSIOLOGICAL CHANGES DURING PREGNANCY1may 20222Pragati BholeNo ratings yet
- Menstrual CycleDocument15 pagesMenstrual CycleNazkie Alganion100% (2)
- Anatomy of The Endocrine System IIDocument129 pagesAnatomy of The Endocrine System IIShauie CayabyabNo ratings yet
- CHAPTER 6 - Integumentary SystemDocument2 pagesCHAPTER 6 - Integumentary SystemLaraib HabibNo ratings yet
- EndocrinologyDocument50 pagesEndocrinologyCut TirayaNo ratings yet
- Pancreas Function MazenDocument15 pagesPancreas Function MazenAhmed GaberNo ratings yet
- Endocrine Physiology) 21. Female Reproductive Cycle - Ovulation - KeyDocument1 pageEndocrine Physiology) 21. Female Reproductive Cycle - Ovulation - Keyhasanatiya41No ratings yet
- The Skin (Anaphy)Document2 pagesThe Skin (Anaphy)ALEXANDRA COLLEEN ALEGRENo ratings yet
- Thyroidectomy - : An Operation To Remove All or Part of The Thyroid GlandDocument20 pagesThyroidectomy - : An Operation To Remove All or Part of The Thyroid GlandCindy Babsa-ay MaslagNo ratings yet
- Siklus EstrusDocument55 pagesSiklus EstrusGada AnggoroNo ratings yet
- Thyroid ExaminationDocument44 pagesThyroid ExaminationAbdurehman AyeleNo ratings yet
- Fisiologi Siklus Haid (DR - Kanadi SumaprajaDocument70 pagesFisiologi Siklus Haid (DR - Kanadi SumaprajaIntan DhyaksariNo ratings yet
- Basic Jeopardy Template 2003Document52 pagesBasic Jeopardy Template 2003api-236914749No ratings yet
- Uterine Involution and Postpartum Ovarian ActivityDocument8 pagesUterine Involution and Postpartum Ovarian Activityjerry smatt dumtoNo ratings yet