Download as pptx, pdf, or txt
You might also like
- Informatica Cloud Real Time Service Technology and Security OverviewDocument16 pagesInformatica Cloud Real Time Service Technology and Security OverviewLakshminarayana SamaNo ratings yet
- 501 Must-See MoviesDocument9 pages501 Must-See MoviesBranislavZivanovNo ratings yet
- نسخة Blood 1Document29 pagesنسخة Blood 1KyunaNo ratings yet
- Circulatory Disturbance 2Document38 pagesCirculatory Disturbance 2امينو عبدوNo ratings yet
- Ischemia, Infarction, Shock and EdemaDocument44 pagesIschemia, Infarction, Shock and Edemakiran kcNo ratings yet
- Pathology LectureDocument3 pagesPathology LectureAbdullahayad farouqNo ratings yet
- 6 - Ischemic Heart DiseaseDocument38 pages6 - Ischemic Heart DiseaseHamzehNo ratings yet
- Mass Effect, Menyebabkan Gangguan Fisik Dari Arsitektur Parenkim Otak. Peningkatan TekananDocument4 pagesMass Effect, Menyebabkan Gangguan Fisik Dari Arsitektur Parenkim Otak. Peningkatan TekananJoko SantosoNo ratings yet
- 2 Embolism, Infarction and ShockDocument57 pages2 Embolism, Infarction and ShockSuman MahmoodNo ratings yet
- Hemodynamic Disorder PC1Document227 pagesHemodynamic Disorder PC1Bereket weybaNo ratings yet
- Week 10 - Hypertension, Atherosclerosis, ArrhythmiaDocument14 pagesWeek 10 - Hypertension, Atherosclerosis, Arrhythmiashivani patel100% (1)
- Defense Againts Infectious Diseases ClassworkDocument2 pagesDefense Againts Infectious Diseases ClassworkSofia OrtizNo ratings yet
- Acute Myocardia L Infarction: Subtit LEDocument33 pagesAcute Myocardia L Infarction: Subtit LEGabiiGabriiela100% (1)
- Hemodynamic Disorders, Thromboembolic Disease, and ShockDocument87 pagesHemodynamic Disorders, Thromboembolic Disease, and Shockgifty100% (1)
- Hemodynamic Disorders-RevisedDocument118 pagesHemodynamic Disorders-Revisedspringding0% (1)
- Patho Activity-2Document12 pagesPatho Activity-2uvgcmbsstudyNo ratings yet
- Vascular Pathology - Lesson - 10Document81 pagesVascular Pathology - Lesson - 10Aya AhmedNo ratings yet
- Pathanatomy Lecture - 17 Arterial Hyper Tent IonDocument53 pagesPathanatomy Lecture - 17 Arterial Hyper Tent IonChris QueiklinNo ratings yet
- Acute Myocardial InfarctionDocument14 pagesAcute Myocardial InfarctionJardee DatsimaNo ratings yet
- Hemodynamic DisorderDocument7 pagesHemodynamic DisorderYana MilyushinaNo ratings yet
- Haemodyanamics Flash PointsDocument3 pagesHaemodyanamics Flash PointsHassan AhmadNo ratings yet
- Stroke MsDocument57 pagesStroke MsAishwarya ShahNo ratings yet
- Bab 2 Tinjauan Pustaka 2.1 Acute Limb IschemiaDocument14 pagesBab 2 Tinjauan Pustaka 2.1 Acute Limb IschemiabayuaaNo ratings yet
- StrokeDocument17 pagesStrokeJo CanensNo ratings yet
- Pathology of Acute Myocardial InfarctionDocument13 pagesPathology of Acute Myocardial InfarctionNaily Nuzulur RohmahNo ratings yet
- Pathology For Dentistry Lect 10Document9 pagesPathology For Dentistry Lect 10Mohamad AladdinNo ratings yet
- 1.old Posterior-WPS OfficeDocument6 pages1.old Posterior-WPS Officeashokyd1411No ratings yet
- Cardiovascular Pathology 2024Document132 pagesCardiovascular Pathology 2024Chen HouyuNo ratings yet
- Lecture13 & 14aDocument5 pagesLecture13 & 14aIsak ShatikaNo ratings yet
- Lecture 5Document5 pagesLecture 5Isak ShatikaNo ratings yet
- Chapter 9: BLOOD VESSELSDocument18 pagesChapter 9: BLOOD VESSELSangelina buenaNo ratings yet
- Hemodynamic Disorders, Thromoboembolism and ShockDocument10 pagesHemodynamic Disorders, Thromoboembolism and ShockMarinelle TumanguilNo ratings yet
- Chapter 9: BLOOD VESSELSDocument19 pagesChapter 9: BLOOD VESSELSangelina buenaNo ratings yet
- Sirkulasi Koroner: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraDocument36 pagesSirkulasi Koroner: Departemen Fisiologi Fakultas Kedokteran Universitas Sumatera UtaraYohanna SinuhajiNo ratings yet
- Cerebral Blood Flow and Pathophysiology: The Vascular SystemDocument3 pagesCerebral Blood Flow and Pathophysiology: The Vascular SystemJerome ReyNo ratings yet
- Acute Limb Ischemia (Ali) An Overview of Clinical DiagnosisDocument13 pagesAcute Limb Ischemia (Ali) An Overview of Clinical DiagnosisShaastieNo ratings yet
- Acute Limb Ischemia 2017 - OKDocument21 pagesAcute Limb Ischemia 2017 - OKDiego RodriguesNo ratings yet
- Chap4 Hemodynamics F2Document12 pagesChap4 Hemodynamics F2Twinkle Salonga100% (3)
- Cardiovascular Diseases (CVD) : AtherosclerosisDocument4 pagesCardiovascular Diseases (CVD) : Atherosclerosisnan doeNo ratings yet
- Disorders of Vascular Flow Yiran Ni M.DDocument42 pagesDisorders of Vascular Flow Yiran Ni M.DMohsin TanmoyNo ratings yet
- 5 - Pathology of CADDocument58 pages5 - Pathology of CADregeti bhargavNo ratings yet
- 2024 - Blood VesselsDocument35 pages2024 - Blood Vesselsmanasep89No ratings yet
- Ischaemic Heart Disease (IHD) Is Defined As Acute or Chronic Form of Cardiac Disability Arising FromDocument5 pagesIschaemic Heart Disease (IHD) Is Defined As Acute or Chronic Form of Cardiac Disability Arising FromIsak ShatikaNo ratings yet
- Kuliah Blok 2 Gangguan Hemodinamik Trombosis Dan ShockDocument37 pagesKuliah Blok 2 Gangguan Hemodinamik Trombosis Dan ShockAnonymous N2PHMnTIYLNo ratings yet
- DB50 - Pa Tho Physiology and Pathology of ShockDocument4 pagesDB50 - Pa Tho Physiology and Pathology of ShockChelsea RoseNo ratings yet
- (5+6) PATH - Cerebrovascular AccidentsDocument16 pages(5+6) PATH - Cerebrovascular AccidentsNader NURESNo ratings yet
- Acute StrokeDocument13 pagesAcute StrokeJoel CanenciaNo ratings yet
- Coronary Arteritis DDDocument6 pagesCoronary Arteritis DDvam buddhaNo ratings yet
- Systemic PathologyDocument21 pagesSystemic PathologyAijan MurzalievaNo ratings yet
- Myocardial Infarction Unstable Angina PericarditisDocument15 pagesMyocardial Infarction Unstable Angina PericarditisironNo ratings yet
- Class 17Document46 pagesClass 17Nishani SatiyaseelanNo ratings yet
- Ischemic Heart DiseaseDocument6 pagesIschemic Heart DiseaseApril Joy Villacorta PonceNo ratings yet
- Acute Limb IschemiaDocument21 pagesAcute Limb IschemiajuanpbagurNo ratings yet
- AneurysmDocument40 pagesAneurysmRichardNo ratings yet
- Hemodynamic DisoderDocument4 pagesHemodynamic DisodermutimuthiNo ratings yet
- Book Cardio ConceptDocument29 pagesBook Cardio ConceptJulia Rae Delos SantosNo ratings yet
- Coronary Artery AtherosclerosisDocument25 pagesCoronary Artery AtherosclerosisShahrizal Che JamelNo ratings yet
- Practical Notes 1 - MajdiDocument8 pagesPractical Notes 1 - MajdiMagdy AlnassrallahNo ratings yet
- ARTERIOSCLEROSISDocument4 pagesARTERIOSCLEROSISmitiku aberaNo ratings yet
- Arteriosclerosis & Atherosclerosis: Arteriosclerosis or "Hardening of The Arteries.Document29 pagesArteriosclerosis & Atherosclerosis: Arteriosclerosis or "Hardening of The Arteries.blossomkdcNo ratings yet
- Ischemic Heart DiseaseDocument13 pagesIschemic Heart Diseasegyspsunshine girlNo ratings yet
- Lecture 3 - IHDDocument29 pagesLecture 3 - IHDقاسم اليوسفيNo ratings yet
- Histotechniques For Medical Laboratory (Lab 1)Document15 pagesHistotechniques For Medical Laboratory (Lab 1)قاسم اليوسفيNo ratings yet
- Lecture One of Analytical Chemistry 1Document15 pagesLecture One of Analytical Chemistry 1قاسم اليوسفيNo ratings yet
- Dehydration: Acetone DioxaneDocument15 pagesDehydration: Acetone Dioxaneقاسم اليوسفيNo ratings yet
- TreponemaDocument13 pagesTreponemaقاسم اليوسفيNo ratings yet
- Intermediate I. Lesson Plan Submittal. 2019Document56 pagesIntermediate I. Lesson Plan Submittal. 2019juan vNo ratings yet
- First Day of School ScheduleDocument3 pagesFirst Day of School Scheduleapi-381872653No ratings yet
- Chua vs. Comelec - 2016Document15 pagesChua vs. Comelec - 2016Yaki RelevoNo ratings yet
- OGL 481 Pro-Seminar I: PCA-Symbolic Frame WorksheetDocument4 pagesOGL 481 Pro-Seminar I: PCA-Symbolic Frame Worksheetapi-538926640No ratings yet
- San Luis V San LuisDocument10 pagesSan Luis V San LuisruslanmanagoNo ratings yet
- Communication Skills 2Document62 pagesCommunication Skills 2Maria Romelyn Montajes0% (1)
- Configuracion Oscam - ConfDocument19 pagesConfiguracion Oscam - ConfJuanMi AndradaNo ratings yet
- Microsoft Dynamics 365 Business Central Prospect Engagement GuideDocument9 pagesMicrosoft Dynamics 365 Business Central Prospect Engagement GuideRobinNo ratings yet
- Young Stars 5Document7 pagesYoung Stars 5Elva CabelloNo ratings yet
- Sex, Gender, Sexuality and Reproductive HealthDocument26 pagesSex, Gender, Sexuality and Reproductive HealthKaycee Daya-Magos100% (1)
- Surrogacy Term PaperDocument12 pagesSurrogacy Term PaperRotsen Kho YuteNo ratings yet
- Week 11 Poli Rev Uber DiegestsDocument26 pagesWeek 11 Poli Rev Uber DiegestsAndrew LastrolloNo ratings yet
- End Compulsory SchoolingDocument18 pagesEnd Compulsory SchoolingIndependence Institute100% (1)
- Company Profile-UPDATEDDocument4 pagesCompany Profile-UPDATEDJanet SilvanoNo ratings yet
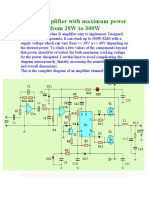
- Class D Amplifier With Maximum Power Adjustable From 20W To 300WDocument13 pagesClass D Amplifier With Maximum Power Adjustable From 20W To 300Wramontv032428No ratings yet
- 10 Reasons Why You Need Social Science Audrey Ostler PDFDocument5 pages10 Reasons Why You Need Social Science Audrey Ostler PDFSadique PK MampadNo ratings yet
- Package Arulesviz': R Topics DocumentedDocument8 pagesPackage Arulesviz': R Topics Documentedarclite123No ratings yet
- 19 - Dabu v. KapunanDocument2 pages19 - Dabu v. KapunanClaire RoxasNo ratings yet
- Learning Activity Sheet (Las) No. 1Document4 pagesLearning Activity Sheet (Las) No. 1warren bascon100% (1)
- Rousseau As A NaturalistDocument12 pagesRousseau As A NaturalistLalit JoshiNo ratings yet
- Che692-Process Modelling and Simulation - Assignment: TopicDocument6 pagesChe692-Process Modelling and Simulation - Assignment: TopicEclatgridNo ratings yet
- Implementation of MTBMLE in Pangasinan IDocument63 pagesImplementation of MTBMLE in Pangasinan Isaro jerwayneNo ratings yet
- Chapter 2c - EEDocument32 pagesChapter 2c - EEHarithZakariaNo ratings yet
- Mcguire eDocument1 pageMcguire efranjuranNo ratings yet
- Consider The Following: Advanced Database ProjectDocument1 pageConsider The Following: Advanced Database Projectteshu wodesa0% (1)
- Commercial Analysis-PetrajDocument4 pagesCommercial Analysis-Petrajapi-548034835No ratings yet
- Cavendish University Zambia School of LawDocument21 pagesCavendish University Zambia School of LawAngel MoongaNo ratings yet
- Republic of The PhilippinesdwwwwDocument13 pagesRepublic of The PhilippinesdwwwwGo IdeasNo ratings yet