Download as pptx, pdf, or txt
You might also like
- Online Rental System Project SynopsisDocument114 pagesOnline Rental System Project SynopsisMuzaFar64% (39)
- Dead Ever After EbookDocument2 pagesDead Ever After Ebookkjkorner530% (2)
- Biliary Tract Disease - Emmet AndrewsDocument52 pagesBiliary Tract Disease - Emmet AndrewsBoneyJalgarNo ratings yet
- Calculous Biliary DiseaseDocument71 pagesCalculous Biliary DiseaseMinnossNo ratings yet
- Chronic Liver DiseaseDocument30 pagesChronic Liver Diseaseprajwal86% (7)
- Disease of The Biliary TractDocument7 pagesDisease of The Biliary TractMae DoctoleroNo ratings yet
- Common Bile Duct (CBD) Stone (Choledocholithiasis)Document4 pagesCommon Bile Duct (CBD) Stone (Choledocholithiasis)Manurun Londong AlloNo ratings yet
- Surg 2Document58 pagesSurg 2api-3866881100% (1)
- Gallbladder DiseaseDocument67 pagesGallbladder DiseaseKhadira MohammedNo ratings yet
- Gall Stone Disease: DR M.farhad General SurgeonDocument56 pagesGall Stone Disease: DR M.farhad General SurgeondrelvNo ratings yet
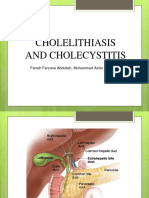
- Cholelithiasis and CholecystitisDocument19 pagesCholelithiasis and CholecystitisElokNo ratings yet
- Pathogenesis of Diseases of The Gallbladder and Biliary TractDocument28 pagesPathogenesis of Diseases of The Gallbladder and Biliary TractMuhammad MakkiNo ratings yet
- Biliary Tract Dis Pancreatitis 2015Document143 pagesBiliary Tract Dis Pancreatitis 2015eiad-mahmoudNo ratings yet
- Lecture On Conjugated HyperbilirubinaemiaDocument38 pagesLecture On Conjugated HyperbilirubinaemiaIgwe SolomonNo ratings yet
- Biliary Tree LectureDocument58 pagesBiliary Tree Lecturesgod34No ratings yet
- Chronic PancreatitisDocument27 pagesChronic Pancreatitismariyatony28No ratings yet
- Day 10. Choledocholitiasis, CholangitisDocument26 pagesDay 10. Choledocholitiasis, Cholangitisهنادي رازمNo ratings yet
- General Surgery A Revision Session For FinalsDocument69 pagesGeneral Surgery A Revision Session For Finalsimperiallight100% (2)
- CHOLECYSTITISDocument6 pagesCHOLECYSTITISAnar ChuluunNo ratings yet
- 8 28 12 R Schaffer MDDocument51 pages8 28 12 R Schaffer MDKay BristolNo ratings yet
- Billiary Diseases Lecture 2023-2024Document10 pagesBilliary Diseases Lecture 2023-2024Taha MuhammedNo ratings yet
- CHolelitiasis, CholesistitisDocument44 pagesCHolelitiasis, CholesistitistrianaamaliaNo ratings yet
- Liver, Biliary Tree and Pancreas Pathology Lecture Final by DRDocument94 pagesLiver, Biliary Tree and Pancreas Pathology Lecture Final by DRapi-3700579100% (5)
- Pancreaticobiliary Lesions: DR Rofanda BakeerDocument29 pagesPancreaticobiliary Lesions: DR Rofanda BakeerKareem DawoodNo ratings yet
- Surgery of The Biliary System KFS 2022Document100 pagesSurgery of The Biliary System KFS 2022ahmedelkaranshawy123456789No ratings yet
- CME - Dr. Amarchand Bajaj (Revised)Document19 pagesCME - Dr. Amarchand Bajaj (Revised)Rahul AryaNo ratings yet
- Curs 15v-2018Document96 pagesCurs 15v-2018Alice ChirilaNo ratings yet
- Biliary Tract DiseaseDocument40 pagesBiliary Tract DiseaseIsaac MwangiNo ratings yet
- Diseases of GallbladderDocument85 pagesDiseases of GallbladderFatima Marwa Teo MaghinayNo ratings yet
- Acute CholecystitisDocument12 pagesAcute CholecystitisDwi AstutyNo ratings yet
- Approach To Cholestatic Jaundice: DR - Ram Raut - JR III (Medicine) Guide - Dr.D.B. Kadam Seminar Teacher-Dr - NitinDocument68 pagesApproach To Cholestatic Jaundice: DR - Ram Raut - JR III (Medicine) Guide - Dr.D.B. Kadam Seminar Teacher-Dr - NitinAnan JaiswalNo ratings yet
- Kholesistis & Kholelitiasis 30-11-14Document67 pagesKholesistis & Kholelitiasis 30-11-14Dian AzhariaNo ratings yet
- Biliary Tract DiseaseDocument6 pagesBiliary Tract DiseaseRafael KameradNo ratings yet
- Biliary Tract DiseaseDocument52 pagesBiliary Tract DiseaseAna Cotoman100% (1)
- Exocrine Pancreatic and Biliary Disorders and ManagementDocument77 pagesExocrine Pancreatic and Biliary Disorders and ManagementAnthon Kyle TropezadoNo ratings yet
- Progesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichDocument9 pagesProgesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichFerreze AnnNo ratings yet
- Progesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichDocument9 pagesProgesterone Has Been Shown To Decrease Gall-Bladder Motility, WhichFerreze AnnNo ratings yet
- Acute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Document63 pagesAcute Abdomen: Part I: Intestinal Obstruction/Bowel Infarction/ Constipation (And How To Assess and Initiate Management)Rumana IslamNo ratings yet
- Jaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Document46 pagesJaundice: Presented by Dr. Pollock Prepared by Christopher Edwards Tintanalli Chapter 84, Pgs. 560-561 October 2005Edwin Jose SNo ratings yet
- Curs 15v-2018hDocument96 pagesCurs 15v-2018hMirceaDraghiciNo ratings yet
- Biliary Diseases (Salman)Document21 pagesBiliary Diseases (Salman)Batool AldaherNo ratings yet
- PRAVEENDocument33 pagesPRAVEENNaviNo ratings yet
- Recent Management of Calculous Biliary DiseaseDocument35 pagesRecent Management of Calculous Biliary DiseaseAbhishek SarafNo ratings yet
- Acute Abdomen: Medic Curses A MopDocument50 pagesAcute Abdomen: Medic Curses A MopSharaz AhmedNo ratings yet
- The Diseases of GallbladderDocument27 pagesThe Diseases of GallbladderAroosha IbrahimNo ratings yet
- Gall Bladder & Pancreas 2010Document61 pagesGall Bladder & Pancreas 2010Ali_Hussain_Bo_3755No ratings yet
- Gastro POMDocument63 pagesGastro POMLionell Castillo100% (1)
- Gallstone Diseases: Chea Chan Hooi Surgeon Department of Surgery Sibu HospitalDocument47 pagesGallstone Diseases: Chea Chan Hooi Surgeon Department of Surgery Sibu HospitalIULIAN LUPUNo ratings yet
- Approach To Patient With Gastrointestinal SystemDocument23 pagesApproach To Patient With Gastrointestinal SystemMarshell TendeanNo ratings yet
- CholecystitisDocument5 pagesCholecystitisdhanya jayanNo ratings yet
- Liver CirrohosisDocument157 pagesLiver CirrohosisSeema SachdevaNo ratings yet
- Learn From The Mistakes of Others. You Can't Live Long Enough To Make Them All Yourself !Document29 pagesLearn From The Mistakes of Others. You Can't Live Long Enough To Make Them All Yourself !DrHassan AbdirahmanNo ratings yet
- Post HepaticDocument6 pagesPost HepaticBilla NabillaNo ratings yet
- Chole Lithia SisDocument35 pagesChole Lithia SisKrismadhaNo ratings yet
- Cholelithiasis and Choledocholithiasis Infos ..Document5 pagesCholelithiasis and Choledocholithiasis Infos ..Franzia Izandra Alkuino MojicaNo ratings yet
- CirrhosisDocument55 pagesCirrhosisFUTURE DOCTORNo ratings yet
- Acute Intestinal ObstructionDocument50 pagesAcute Intestinal ObstructionDin LukbanNo ratings yet
- Pancreatitis, CholecystitisDocument25 pagesPancreatitis, Cholecystitismariyatony28No ratings yet
- Ntroduction: (1) (2) (3) Go ToDocument6 pagesNtroduction: (1) (2) (3) Go ToretnaNo ratings yet
- 1 GallbladderDocument36 pages1 Gallbladdercephas chinkoliNo ratings yet
- Current and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryFrom EverandCurrent and Future Developments in Surgery: Volume 2: Oesophago-gastric SurgeryNo ratings yet
- Pharmacology of The Autonomic Nervous SystemDocument44 pagesPharmacology of The Autonomic Nervous SystemBinkisa BilloNo ratings yet
- Nebiyu Proposal HIV AND NUTRTIONDocument28 pagesNebiyu Proposal HIV AND NUTRTIONBinkisa BilloNo ratings yet
- Animal Production Chapter1Document10 pagesAnimal Production Chapter1Binkisa BilloNo ratings yet
- Microeconomics By: Zemach Lemecha (M.SC, Asst. Prof.) : Semester I, 2015Document251 pagesMicroeconomics By: Zemach Lemecha (M.SC, Asst. Prof.) : Semester I, 2015Binkisa Billo0% (1)
- Animal Production Chapter2Document57 pagesAnimal Production Chapter2Binkisa BilloNo ratings yet
- Definition and Scope of SociologyDocument91 pagesDefinition and Scope of SociologyBinkisa BilloNo ratings yet
- Socialwelfareconcepts 2Document36 pagesSocialwelfareconcepts 2Debabrata SutradharNo ratings yet
- The Pain of Procrastination British English TeacherDocument13 pagesThe Pain of Procrastination British English TeacherMartina KačurováNo ratings yet
- The Cellulite Solution: How To Build Firm, Healthy Hips and ThighsDocument4 pagesThe Cellulite Solution: How To Build Firm, Healthy Hips and ThighsNicoleNo ratings yet
- Brain ImagingDocument14 pagesBrain ImagingSenal Malaka PremarathnaNo ratings yet
- Prefinal Lesson2 Literary - DevicesDocument18 pagesPrefinal Lesson2 Literary - DevicesCarina Margallo CelajeNo ratings yet
- Anxiety: A Self Help GuideDocument32 pagesAnxiety: A Self Help Guideabraham.gallegos100% (1)
- Implementing Smart FactoryDocument10 pagesImplementing Smart FactoryUcup VespaNo ratings yet
- Reading ComprehensionDocument76 pagesReading ComprehensionmeimeingynNo ratings yet
- Introduction To Simulation Analysis: FunctionsDocument7 pagesIntroduction To Simulation Analysis: Functionsmittalsakshi020692No ratings yet
- 76.122 Cultural Anthropology: Module I Introductory Overview: Concepts, Methods, and TheoriesDocument26 pages76.122 Cultural Anthropology: Module I Introductory Overview: Concepts, Methods, and TheoriesMerima Jasarevic0% (1)
- Colpitts Oscillator Using Op Amp PDFDocument2 pagesColpitts Oscillator Using Op Amp PDFStewartNo ratings yet
- Silo - Tips Table of Contents Author 03 Introduction 05 Why Do We Gamble 08 Alan Tripp 12 Zeljko Ranogajec 19 Matt Tripp 57Document111 pagesSilo - Tips Table of Contents Author 03 Introduction 05 Why Do We Gamble 08 Alan Tripp 12 Zeljko Ranogajec 19 Matt Tripp 57MattNo ratings yet
- Chapter 03 Communications and DocumentationDocument53 pagesChapter 03 Communications and DocumentationNephNo ratings yet
- AMS Suite - Machinery Health Manager Manual PDFDocument15 pagesAMS Suite - Machinery Health Manager Manual PDFsebastianNo ratings yet
- AAST-CC312-Fall 21-Lec 10Document21 pagesAAST-CC312-Fall 21-Lec 10youssef hossamNo ratings yet
- The Problem and Review of Related Literature and StudiesDocument11 pagesThe Problem and Review of Related Literature and StudiesVincent TayagNo ratings yet
- Mathematics in The Modern World-Module7Document8 pagesMathematics in The Modern World-Module7erickson hernanNo ratings yet
- IYCF Counselling Cards ChildFundPCADocument34 pagesIYCF Counselling Cards ChildFundPCAChris-Goldie LorezoNo ratings yet
- Model Curriculumn GuideDocument48 pagesModel Curriculumn Guidesabashsabash80% (5)
- Risk Assessment Dan HAccpDocument27 pagesRisk Assessment Dan HAccpNurjana Sigiro100% (1)
- Repaso Bachillerato - EjerciciosDocument5 pagesRepaso Bachillerato - EjerciciosAnonymous qmwoKAfNo ratings yet
- 04 Case # 3 Uy v. Estate of Vipa FernandezDocument3 pages04 Case # 3 Uy v. Estate of Vipa FernandezDee WhyNo ratings yet
- 8 Icebreakers For TeensDocument17 pages8 Icebreakers For TeensJoseph StatonNo ratings yet
- Griffiths Introduction To Genetic Analysis 12th EditionDocument3,002 pagesGriffiths Introduction To Genetic Analysis 12th Editionmartin.kv4No ratings yet
- Lokal Na Pag Aaral ThesisDocument5 pagesLokal Na Pag Aaral Thesisgladyscepparulonewark100% (2)
- Speech Writing and Delivery RubricDocument2 pagesSpeech Writing and Delivery RubricKrezia Erica CorpinNo ratings yet
- Lecture 6: The Greeks and Basic Hedging: Sources Avellaneda and Laurence J HullDocument20 pagesLecture 6: The Greeks and Basic Hedging: Sources Avellaneda and Laurence J HullJNo ratings yet
- ExerciseDocument9 pagesExercisegundadanNo ratings yet