Download as pptx, pdf, or txt
You might also like
- Basic Airway ManagementDocument98 pagesBasic Airway ManagementRani Salsabilah100% (1)
- (Oxy) Med-Surg Checklist With RationaleDocument13 pages(Oxy) Med-Surg Checklist With RationaleUri Perez MontedeRamos100% (1)
- Advanced Airway Management PrintableDocument8 pagesAdvanced Airway Management PrintableMiranda PermatasariNo ratings yet
- Airway ManagementDocument13 pagesAirway ManagementAlaa DaoudNo ratings yet
- Airway Management Lecture-3Document28 pagesAirway Management Lecture-3maira ShahzadNo ratings yet
- Airway ManagementDocument33 pagesAirway Managementbrida.bluesNo ratings yet
- Airway EquipmentDocument47 pagesAirway Equipmentyoustiana dwi rusitaNo ratings yet
- Airway ManagementDocument29 pagesAirway Managementapi-142637023No ratings yet
- Airway Management - Supraglottic Airway PDFDocument4 pagesAirway Management - Supraglottic Airway PDFPiet Pogen PoelNo ratings yet
- Sedation Airway ManagementDocument5 pagesSedation Airway ManagementMilana AndrewNo ratings yet
- Airway Management-Dr RistiawanDocument75 pagesAirway Management-Dr RistiawanjavajavuNo ratings yet
- Airway Masterclass 2 TOTW 043 2007Document11 pagesAirway Masterclass 2 TOTW 043 2007eryxspNo ratings yet
- - اطلس جهاز التخدير-30-34Document5 pages- اطلس جهاز التخدير-30-34علي الاسديNo ratings yet
- AirwayDocument66 pagesAirwayMolina NaputriNo ratings yet
- Airway Management: Med 5: Anaesthesia ModuleDocument83 pagesAirway Management: Med 5: Anaesthesia Modulederek lauNo ratings yet
- Anaesthesia AIRWAYS, LARYNGOSCOPES, NRVS AND CONNECTORSDocument41 pagesAnaesthesia AIRWAYS, LARYNGOSCOPES, NRVS AND CONNECTORSabciximab100% (2)
- AirwaysDocument36 pagesAirwaysSaathifernandza ThothadiNo ratings yet
- LECTURE4-Airway Management and Equipment-Dr ManaaDocument68 pagesLECTURE4-Airway Management and Equipment-Dr ManaasnezaimNo ratings yet
- Airway ManagementDocument13 pagesAirway ManagementKandi IssayaNo ratings yet
- Airway Management VentilationDocument13 pagesAirway Management Ventilationmariafer99No ratings yet
- Management of AirwaysDocument12 pagesManagement of AirwaysdyahNo ratings yet
- AiwaryManagement 1Document72 pagesAiwaryManagement 1Giselle EstoquiaNo ratings yet
- Final-Intubation Extubation Plus (1) - 1Document112 pagesFinal-Intubation Extubation Plus (1) - 1Lylibette Anne CalimlimNo ratings yet
- Airway ManagementDocument49 pagesAirway ManagementusuisatimNo ratings yet
- Rapid Sequence Intubation: BY Budak KecikDocument25 pagesRapid Sequence Intubation: BY Budak KecikAqua ForceNo ratings yet
- Care of Patients Requiring Oxygen Therapy or TracheostomyDocument5 pagesCare of Patients Requiring Oxygen Therapy or TracheostomyAnnie Rose Dorothy MamingNo ratings yet
- Review of Respiratory ArrestDocument2 pagesReview of Respiratory ArrestsrimatsimhasaneshwarNo ratings yet
- List Atleast 15 Intubation Euipments With Images and Relate Their Functions or PurposesDocument6 pagesList Atleast 15 Intubation Euipments With Images and Relate Their Functions or Purposesclaudine padillonNo ratings yet
- SECTION 2 CHAPTER 4 Tracheal IntubationDocument46 pagesSECTION 2 CHAPTER 4 Tracheal IntubationRhea Andrea UyNo ratings yet
- Mechanical IntubationDocument5 pagesMechanical IntubationBAILEN AYNNA PEARLNo ratings yet
- Artificial AirwaysDocument17 pagesArtificial AirwaysSri DarmayantiNo ratings yet
- Rapid Sequence Intubation ReportDocument55 pagesRapid Sequence Intubation Reportlorkan19100% (1)
- Skills Training Manual BookDocument19 pagesSkills Training Manual BookMuhammad SawalNo ratings yet
- Airway Management Topic 2Document8 pagesAirway Management Topic 2Lenard SakiliNo ratings yet
- Tabije, Arvie Jayselle PDocument8 pagesTabije, Arvie Jayselle PJaysellePuguonTabijeNo ratings yet
- Et IntubationDocument3 pagesEt IntubationCherry L. M. JaramilloNo ratings yet
- Oxygentherapy 170826044952Document47 pagesOxygentherapy 170826044952snezaimNo ratings yet
- Airway ManagementDocument11 pagesAirway Managementmegayani santosoNo ratings yet
- Oxygen TherapyDocument74 pagesOxygen TherapyMark Reynie Renz Silva100% (6)
- Drugs and Equipments RaceDocument236 pagesDrugs and Equipments RaceparuNo ratings yet
- Combitube: IndicationDocument3 pagesCombitube: IndicationV IdyaNo ratings yet
- BY: Mr. M. Shivanandha ReddyDocument74 pagesBY: Mr. M. Shivanandha Reddy3amabelle arevalo100% (2)
- Airway Management - IntubationDocument31 pagesAirway Management - IntubationRajaNo ratings yet
- Co Vi Acls - 0Document18 pagesCo Vi Acls - 0Amer ShihadeNo ratings yet
- Airway and The NurseDocument7 pagesAirway and The NursecarmenbuleandraNo ratings yet
- ETT IntubationDocument10 pagesETT IntubationPoova RagavanNo ratings yet
- Positive Expiratory PressureDocument21 pagesPositive Expiratory PressureVijayalaxmi KathareNo ratings yet
- Airway Adjuncts 2Document9 pagesAirway Adjuncts 2Paul ButlerNo ratings yet
- Administering Oxygen Therapy Powerpoint 3Document58 pagesAdministering Oxygen Therapy Powerpoint 3reema_rt75% (8)
- Assisting in Endotracheal SuctioningDocument38 pagesAssisting in Endotracheal SuctioningMargarita Limon BalunesNo ratings yet
- OxygenationDocument30 pagesOxygenationmelanie silvaNo ratings yet
- O2 Presentation2Document28 pagesO2 Presentation2Sangeetha KarunanithiNo ratings yet
- Nasal CannulaDocument3 pagesNasal CannulaVALENZUELA DELIESA E.No ratings yet
- 2 - Airway and Ventilatory ManagementDocument5 pages2 - Airway and Ventilatory ManagementJessie E. GeeNo ratings yet
- Airway IntubationDocument60 pagesAirway IntubationKeerthikumar Parvatha100% (1)
- Airway ManagementDocument38 pagesAirway ManagementyafetNo ratings yet
- Endotracheal Tube IntubationDocument5 pagesEndotracheal Tube IntubationKim Kristine D. GuillenNo ratings yet
- First Two Steps Are Discussed in This SectionDocument26 pagesFirst Two Steps Are Discussed in This SectionArchanaShenoyNo ratings yet
- Intubation and Artificial VentilationDocument83 pagesIntubation and Artificial VentilationKM KarthikNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- BOOKSTORE Pricelist Foreign Titles Books For COLLEGE As of OCTOBER 1. 2018Document108 pagesBOOKSTORE Pricelist Foreign Titles Books For COLLEGE As of OCTOBER 1. 2018Cey LeoncioNo ratings yet
- Dr. Pedro Dennis Cereno, and Dr. Santos Zafe, Petitioners, vs. Court of Appeals, Spouses Diogenes S. Olavere and Fe R. Serrano, RespondentsDocument11 pagesDr. Pedro Dennis Cereno, and Dr. Santos Zafe, Petitioners, vs. Court of Appeals, Spouses Diogenes S. Olavere and Fe R. Serrano, Respondentssophia100% (1)
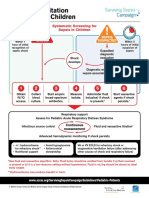
- PED Surviving Sepsis AlgorithmDocument2 pagesPED Surviving Sepsis AlgorithmDaniel Cruz de AbreuNo ratings yet
- A Quick Guide On How To Achieve Gold / Silver Quality CertificateDocument101 pagesA Quick Guide On How To Achieve Gold / Silver Quality CertificateAnonymous 4WAq7tlNo ratings yet
- Malamed 22 04Document5 pagesMalamed 22 04Chintya JessicaNo ratings yet
- INISS Prospectus Part A JULY-2023Document37 pagesINISS Prospectus Part A JULY-2023Vaibhav TrivediNo ratings yet
- Postanesthesia Care: Muhamad Chairul FadhilDocument28 pagesPostanesthesia Care: Muhamad Chairul FadhilMuhammad Chairul Fadhil100% (1)
- Prometric-MOH PageDocument22 pagesPrometric-MOH Pageprabha.s198784No ratings yet
- 148-Article Text-565-1-10-20211005Document11 pages148-Article Text-565-1-10-20211005sri wahyundari manikNo ratings yet
- Test Bank For Building A Medical Vocabulary 7th Edition Leonard DownloadDocument20 pagesTest Bank For Building A Medical Vocabulary 7th Edition Leonard DownloadMarquis Dixon100% (39)
- Dental SpecialtiesDocument6 pagesDental SpecialtiesAn 1. Nguyễn Ngọc PhươngNo ratings yet
- JANUARY 2016: Ob-Gyn ProceduresDocument4 pagesJANUARY 2016: Ob-Gyn ProceduresaringkinkingNo ratings yet
- List of Medical Facilities in India: WWW - Gov.ukDocument81 pagesList of Medical Facilities in India: WWW - Gov.ukShah PratikNo ratings yet
- Expanded RolesDocument99 pagesExpanded RolesIvan Derek Villena WycocoNo ratings yet
- Competition RatiosDocument4 pagesCompetition RatiosAkshit SharmaNo ratings yet
- 1 - ESR ChecklistDocument6 pages1 - ESR Checklistlala khalilNo ratings yet
- Fee Benchmarks Advisory Committee ReportDocument50 pagesFee Benchmarks Advisory Committee ReportArie PurwantoNo ratings yet
- Answer Key 1Document10 pagesAnswer Key 1mohammadatikuzzamanNo ratings yet
- Operation Theater TechnicianDocument26 pagesOperation Theater TechnicianMohammadSaqibMinhasNo ratings yet
- Guia Tiva 2018Document14 pagesGuia Tiva 2018John Bryan Herrera DelgadoNo ratings yet
- Dental Anestesi Jurnal 2Document2 pagesDental Anestesi Jurnal 2Indira NoormaliyaNo ratings yet
- List of Anesthetic, Analgesic and Tranquilizer Drugs Veterinary)Document25 pagesList of Anesthetic, Analgesic and Tranquilizer Drugs Veterinary)drbadman77100% (2)
- Holden Healthcare ProfileDocument42 pagesHolden Healthcare ProfileEdwin BennyNo ratings yet
- Epidural AnaesthesiaDocument18 pagesEpidural Anaesthesiarainbow rainNo ratings yet
- Analgesic ClassificationDocument4 pagesAnalgesic Classificationvie_apt6299No ratings yet
- Care of Ventilator PatientDocument39 pagesCare of Ventilator Patientsandhya100% (1)
- Staffing in Ot and Members of Surgical TeamDocument4 pagesStaffing in Ot and Members of Surgical Teamvinnu kalyan50% (2)
- Journal Homepage: - : Manuscript HistoryDocument7 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- BLS-1Document24 pagesBLS-1Fajar ShahidNo ratings yet
- E000539 FullDocument7 pagesE000539 FullmatmirceaNo ratings yet