Download as pptx, pdf, or txt
You might also like
- Recall For Primary 2022Document200 pagesRecall For Primary 2022S G0% (1)
- CHFDocument24 pagesCHFTilahun TesemaNo ratings yet
- 5-Heart FailureDocument12 pages5-Heart FailureJericho De GuzmanNo ratings yet
- Congestive Cardiac FailureDocument27 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Asist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and ToxicologyDocument52 pagesAsist. Lecturer Hasan Adnan Hashim Msc. Pharmacology and Toxicologyمصطفى ابراهيم سعيدNo ratings yet
- Unit 05 (A) Cardiac Glycosides, Educational PlatformDocument41 pagesUnit 05 (A) Cardiac Glycosides, Educational PlatformSajid AhmadNo ratings yet
- Drugs in CHFDocument48 pagesDrugs in CHFBishnu BhandariNo ratings yet
- CHF and HTDocument120 pagesCHF and HTcreativejoburgNo ratings yet
- Obat Antiarritmia: M Fadhol RomdhoniDocument22 pagesObat Antiarritmia: M Fadhol RomdhoniOcie SatyoNo ratings yet
- Pharmacology of Antiarrhytmic DrugsDocument75 pagesPharmacology of Antiarrhytmic DrugsTeckfong MigrateNo ratings yet
- Drugs Used in HF IIDocument40 pagesDrugs Used in HF IIJamal LudinNo ratings yet
- Cardiovascular Drugs: by Dr. Md. Ruhul KuddusDocument56 pagesCardiovascular Drugs: by Dr. Md. Ruhul Kuddus53-Deepankar SutradharNo ratings yet
- Cardiac Medications:: What's With The Mixing & Matching?Document97 pagesCardiac Medications:: What's With The Mixing & Matching?TinaHoNo ratings yet
- Cardiac GlycosidesDocument8 pagesCardiac GlycosidesShan Sicat100% (1)
- Heart Failure: Zelalem T., MD Yr III Resident, PediatricsDocument65 pagesHeart Failure: Zelalem T., MD Yr III Resident, PediatricsChalie MequanentNo ratings yet
- Pathophysiology of Heart Failure: Prof. J. HanacekDocument48 pagesPathophysiology of Heart Failure: Prof. J. Hanaceksukarni84sgdNo ratings yet
- Digitalis ToxicityDocument55 pagesDigitalis ToxicityBahaa Shaaban100% (1)
- Updated Lecture July2023-AntiarrthymicsDocument54 pagesUpdated Lecture July2023-Antiarrthymicsg.4ssilaNo ratings yet
- Cardiac PharmacologyDocument23 pagesCardiac PharmacologyRavi Kant IyerNo ratings yet
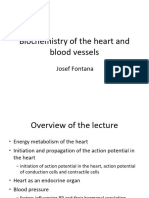
- Biochemistry of The Heart and Blood Vessels 2021 3 4Document44 pagesBiochemistry of The Heart and Blood Vessels 2021 3 4jakukNo ratings yet
- Congestive Cardiac FailureDocument21 pagesCongestive Cardiac FailureKrupasagar Pn PalegarNo ratings yet
- Antiarrhythmias Agents: By: Tirta Darmawan Susanto, Dr.,MkesDocument64 pagesAntiarrhythmias Agents: By: Tirta Darmawan Susanto, Dr.,MkesShally ChandraNo ratings yet
- 03heart FailureDocument37 pages03heart Failureyonem11615No ratings yet
- СердечнаяDocument70 pagesСердечнаяDaniel FunkNo ratings yet
- CONGESTIVE HEART FAILURE - New-1Document32 pagesCONGESTIVE HEART FAILURE - New-1Agus SuprionoNo ratings yet
- Pharma of Heart FailureDocument12 pagesPharma of Heart FailureBaqir BroNo ratings yet
- Antiarrhythmic Drugs by ZebDocument40 pagesAntiarrhythmic Drugs by ZebFazl UllahNo ratings yet
- Presented by Dr. Sannithi Nagarjuna: Coordinator ForDocument70 pagesPresented by Dr. Sannithi Nagarjuna: Coordinator ForMuhammad ZeeshanNo ratings yet
- End - HEART FAILURE NF4024Document23 pagesEnd - HEART FAILURE NF4024drugiztNo ratings yet
- 3 DrugsforHeartFailureDocument60 pages3 DrugsforHeartFailureJov CelNo ratings yet
- Cardiovascular Physiology 0 Anesthetic ImportanceDocument100 pagesCardiovascular Physiology 0 Anesthetic ImportanceSurya SuryaNo ratings yet
- Cvs 1Document37 pagesCvs 1atefmoussaNo ratings yet
- Drugs Acting On The Cardiovascular System-1Document28 pagesDrugs Acting On The Cardiovascular System-1gregorydonald315No ratings yet
- Cardio Tonic DrugDocument25 pagesCardio Tonic DrugNistha MudgilNo ratings yet
- AntiarrhythmicsDocument31 pagesAntiarrhythmicstum chrisNo ratings yet
- Lecture13-Congestive Heart Failure DrugsDocument48 pagesLecture13-Congestive Heart Failure Drugsharis.18No ratings yet
- Lecture2 3Document44 pagesLecture2 3Amanda HizerNo ratings yet
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Heart Failure: Scott Kaba MatafwaliDocument25 pagesHeart Failure: Scott Kaba MatafwaliAngetile KasangaNo ratings yet
- Properties of Cardiac Muscle PDFDocument38 pagesProperties of Cardiac Muscle PDFZaid RazaliNo ratings yet
- 04 Cardiotonic, AntharrythmicDocument125 pages04 Cardiotonic, Antharrythmic2nnfpjy5yvNo ratings yet
- LOW Cardiac Output: Use of Inotropes in Critical CareDocument5 pagesLOW Cardiac Output: Use of Inotropes in Critical CareRiimsha AaymNo ratings yet
- Antiarrhythmic Drugs FinalDocument31 pagesAntiarrhythmic Drugs FinalAmanuel Maru50% (2)
- 6 CVS Lecture 5 - Drugs For Heart FailureDocument55 pages6 CVS Lecture 5 - Drugs For Heart FailureCraig DuHaneyNo ratings yet
- Cardaic Arryhmia1Document36 pagesCardaic Arryhmia1Meththananda Herath100% (1)
- Drugs Used in The Management of Heart Failure: DR Sindwa KanyimbaDocument29 pagesDrugs Used in The Management of Heart Failure: DR Sindwa Kanyimbaedward kaumbaNo ratings yet
- Pathophysiology of Heart FailureDocument51 pagesPathophysiology of Heart FailureJoshua ObrienNo ratings yet
- PharmacologyDocument69 pagesPharmacologyvinkviantNo ratings yet
- Pharmacotherapy of Heart FailureDocument23 pagesPharmacotherapy of Heart Failure88AKKNo ratings yet
- Human Physiology Urinary SystemDocument51 pagesHuman Physiology Urinary Systemmohamedsaithaf2000No ratings yet
- Questions From Exam 08.09.22Document12 pagesQuestions From Exam 08.09.22Ismo SNo ratings yet
- Cardiotonic Drugs Revised DheryanDocument16 pagesCardiotonic Drugs Revised Dheryanlinnet17No ratings yet
- Shock in Children Lecture NewDocument41 pagesShock in Children Lecture NewDky HartonoNo ratings yet
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- Pcol MidtermsDocument25 pagesPcol MidtermsnoyaNo ratings yet
- Cardiovasular SystemDocument26 pagesCardiovasular SystemPhai KoemhienNo ratings yet
- Case Study of Atherosclerosis 1. Risk Factors of AtherosclerosisDocument5 pagesCase Study of Atherosclerosis 1. Risk Factors of AtherosclerosisCarly Beth Caparida LangerasNo ratings yet
- Revised AntiarrhythmicsDocument29 pagesRevised AntiarrhythmicsDang CuevasNo ratings yet
- Concepts in Medicine: The Low Energy StateDocument10 pagesConcepts in Medicine: The Low Energy StatebbbyjmsNo ratings yet
- Lecture FMS 3 2015-2016 (Nata) - Pathophysiology and Pathogenesis of Shock (Restored)Document52 pagesLecture FMS 3 2015-2016 (Nata) - Pathophysiology and Pathogenesis of Shock (Restored)BritneyNo ratings yet
- Critical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsFrom EverandCritical Care Medications: Vasopressors, Inotropes and Anti-Hypertensives Study Guide: Critical Care EssentialsNo ratings yet
- Cme On TuberclosisDocument12 pagesCme On TuberclosisOdulusi DanielNo ratings yet
- Drug Study Cefazolin Module 13Document1 pageDrug Study Cefazolin Module 13Daryl Joy Cortez100% (1)
- AnestesiaDocument18 pagesAnestesiaGündüz AğayevNo ratings yet
- Psychiatric and Behavioral Aspects of Epilepsy Current Perspectives and MechanismsDocument484 pagesPsychiatric and Behavioral Aspects of Epilepsy Current Perspectives and MechanismsTanvi GuptaNo ratings yet
- Individual Medical Policy For Dependents - Dmed: Table of BenefitsDocument6 pagesIndividual Medical Policy For Dependents - Dmed: Table of Benefitsrahul sNo ratings yet
- Cystic HygromaDocument2 pagesCystic HygromaAmal Alahmari100% (1)
- NG & Gastrostomy: Insertion & Tube FeedingDocument28 pagesNG & Gastrostomy: Insertion & Tube Feedingche2x_85No ratings yet
- Pediatrics Dose PDFDocument41 pagesPediatrics Dose PDFsv2036006No ratings yet
- Olfactory Loss in The Era of COVID-19Document11 pagesOlfactory Loss in The Era of COVID-19Mariel TellezNo ratings yet
- DRUG STUDY CefuroximeDocument2 pagesDRUG STUDY CefuroximeLyana Stark92% (39)
- 12 Steps of Alcoholics Anonymous by Mike DiazDocument11 pages12 Steps of Alcoholics Anonymous by Mike Diazmike9diaz-689513No ratings yet
- The Role of Mini Bronchoalveolar Lavage Fluid in The Diagnosis ofDocument7 pagesThe Role of Mini Bronchoalveolar Lavage Fluid in The Diagnosis ofKessi VikaneswariNo ratings yet
- Pharmacotherapy of Urinary Tract InfectionDocument75 pagesPharmacotherapy of Urinary Tract InfectionMariana CreciunNo ratings yet
- AFLUNOV LeafletDocument30 pagesAFLUNOV LeafletEllaNo ratings yet
- Poliomyelitis: Dr. Eiman Sumayyah DPT (Kmu), Ms Neuro (Kmu)Document14 pagesPoliomyelitis: Dr. Eiman Sumayyah DPT (Kmu), Ms Neuro (Kmu)Haniya KhanNo ratings yet
- Pathology Intro Part 1 PDFDocument13 pagesPathology Intro Part 1 PDFAmy LalringhluaniNo ratings yet
- Health VocabularyDocument1 pageHealth VocabularyMary WollstonecraftNo ratings yet
- Phenotypes and Personalized Medicine in The Acute Respiratory Distress SyndromeDocument17 pagesPhenotypes and Personalized Medicine in The Acute Respiratory Distress SyndromeminiypuntoNo ratings yet
- What Need Know About Wild OreganoDocument21 pagesWhat Need Know About Wild OreganoMatt PintoNo ratings yet
- Epstein-Barr Virus - Associated Lymphomas: Ewelina Grywalska and Jacek RolinskiDocument13 pagesEpstein-Barr Virus - Associated Lymphomas: Ewelina Grywalska and Jacek RolinskiR. FortalNo ratings yet
- Schizophrenia Spectrum and Other Psychotic DisordersDocument84 pagesSchizophrenia Spectrum and Other Psychotic DisordersJara YumiNo ratings yet
- School RefusalDocument46 pagesSchool RefusalF. HammoudNo ratings yet
- ADN3-1 Digestive HP - 200 - Yang, Myung SookDocument37 pagesADN3-1 Digestive HP - 200 - Yang, Myung SookNorPhea - នភាNo ratings yet
- Medical History Form 10Document3 pagesMedical History Form 10star WaseemNo ratings yet
- Covid Vaccine May Sterilise Only 70% of Global PolpulationDocument11 pagesCovid Vaccine May Sterilise Only 70% of Global PolpulationSY LodhiNo ratings yet
- Lesson Plan On Cerebro Vascular Accident 1Document13 pagesLesson Plan On Cerebro Vascular Accident 1simonjosan67% (3)
- Group 5 Final - 064830Document8 pagesGroup 5 Final - 064830Stephen EwusiNo ratings yet
- No Vaccine, No ClassesDocument2 pagesNo Vaccine, No ClassesPrences AlegriaNo ratings yet
- Application Cover Form - Portable Skills 2024Document2 pagesApplication Cover Form - Portable Skills 2024LENCELORDNo ratings yet