Download as pptx, pdf, or txt
You might also like
- Defeating Dementia - Mnemonics and Lists From EMRCS PhysiologyDocument7 pagesDefeating Dementia - Mnemonics and Lists From EMRCS PhysiologymyscribeNo ratings yet
- Sample Civil ComplaintDocument5 pagesSample Civil ComplaintHazelmer Fernandez100% (3)
- SULPHUR CONTAINING AMINOACIDS-correctedDocument37 pagesSULPHUR CONTAINING AMINOACIDS-correctedPriyanka RaviNo ratings yet
- Inborn Errors of Protein MetabolismDocument48 pagesInborn Errors of Protein MetabolismChudasama DhruvrajsinhNo ratings yet
- Sulphur Amino AcidsDocument23 pagesSulphur Amino Acidsmadhuribiswal7700No ratings yet
- 47 - BMS305 - Biochemistry - Inherited Diseas of The Kidney and Amino Acids - Lect 3 - Spring 2024Document39 pages47 - BMS305 - Biochemistry - Inherited Diseas of The Kidney and Amino Acids - Lect 3 - Spring 2024kareemosama9916No ratings yet
- 4 Protein ReviewDocument87 pages4 Protein Reviewmika de guzmanNo ratings yet
- Methionine and CysteineDocument20 pagesMethionine and CysteineAshly MartinNo ratings yet
- DEGRADATION OF NON ESSENTIAL AMINO ACIDS Group 3Document50 pagesDEGRADATION OF NON ESSENTIAL AMINO ACIDS Group 3SandraNo ratings yet
- Amino Acid Metabolism Disorders Series 2Document5 pagesAmino Acid Metabolism Disorders Series 2kiedd_04No ratings yet
- Surgery II - Pancreas 2014Document20 pagesSurgery II - Pancreas 2014Medisina101No ratings yet
- Metabolism of Amino AcidsDocument77 pagesMetabolism of Amino Acidswhpzm6ttg8No ratings yet
- Containg Sulfer MetabolismDocument27 pagesContaing Sulfer MetabolismZoya MoraniNo ratings yet
- Abnormal Constituents of Urine Interpretation PracticalDocument42 pagesAbnormal Constituents of Urine Interpretation PracticalTEJASWI ModiNo ratings yet
- Urine AnalysisDocument41 pagesUrine AnalysisAjay SomeshwarNo ratings yet
- Fat MetabolismDocument21 pagesFat MetabolismDipak YogiNo ratings yet
- Urinalysis (Part-2) Constituents of Urine: AbnormalDocument49 pagesUrinalysis (Part-2) Constituents of Urine: AbnormalArnab GhoshNo ratings yet
- 27 - Hypo and Hypernatremia - and Hypo and Hyperkalieama PDFDocument48 pages27 - Hypo and Hypernatremia - and Hypo and Hyperkalieama PDFEITHAR OmarNo ratings yet
- Formation of Urine: NephronDocument44 pagesFormation of Urine: NephronajaysomNo ratings yet
- Urinalysis 2Document9 pagesUrinalysis 2Dawn GonzagaNo ratings yet
- Investigation of Amino Acids DisordersDocument4 pagesInvestigation of Amino Acids Disorderskiedd_04100% (1)
- Renal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesDocument44 pagesRenal Tubules Modify Glomerular Filtrate: Reabsorption of High Threshold SubstancesajaysomNo ratings yet
- Gall StonesDocument13 pagesGall StonesAdwaitha KrNo ratings yet
- Urine AnalysisDocument42 pagesUrine AnalysisajaysomNo ratings yet
- Urine AnalysisDocument69 pagesUrine Analysisvinay0717100% (3)
- Case Reports Gout Vitamins MineralsDocument23 pagesCase Reports Gout Vitamins MineralsNasreen SultanaNo ratings yet
- Proteins and Liver Function TestsDocument56 pagesProteins and Liver Function TestsjoanNo ratings yet
- Calcium, Phosphate, MagnesiumDocument55 pagesCalcium, Phosphate, MagnesiumUdochukwu EnebeNo ratings yet
- Chapter X - Mechanism of Protein MetabolismDocument30 pagesChapter X - Mechanism of Protein MetabolismAngelo AngelesNo ratings yet
- Uric Acid: XiaoliDocument17 pagesUric Acid: XiaoliRian WibowoNo ratings yet
- Kidney DiseasesDocument45 pagesKidney DiseasesSai ViswasNo ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument42 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- Uric AcidDocument28 pagesUric AcidAya100% (1)
- NM 22 Urate 2007Document35 pagesNM 22 Urate 2007api-26938624No ratings yet
- Abnormal Constituents of Urine - 1Document5 pagesAbnormal Constituents of Urine - 1kalpithareddynomulaNo ratings yet
- AUBF MidtermsDocument24 pagesAUBF MidtermsPrince SalvaNo ratings yet
- Parathyroid Gland AnatomyDocument27 pagesParathyroid Gland AnatomyABUBEKER BESHIRNo ratings yet
- Changes in Composition of Urine Stored at Room TemperatureDocument39 pagesChanges in Composition of Urine Stored at Room TemperatureAjay SomeshwarNo ratings yet
- Management Nephrolithiasis OtarraDocument22 pagesManagement Nephrolithiasis Otarrajlcocm-2022-00028No ratings yet
- Renal & Electrolyted Physiology FinalDocument21 pagesRenal & Electrolyted Physiology FinalVondNo ratings yet
- M5 3 HypokalemiaDocument6 pagesM5 3 HypokalemiaVishal KumarNo ratings yet
- Glomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsDocument45 pagesGlomerular Filtrate: - Water - Crystalloids - Uric Acid - Proteins With Low Mol. Wt. E.G. HB, Myohb, BJ ProteinsajaysomNo ratings yet
- Aminacid MetabolismDocument84 pagesAminacid MetabolismAaronJose100% (1)
- Lecture 3 - Uric Acid & GoutDocument31 pagesLecture 3 - Uric Acid & GoutAbdoulhaleem MoNo ratings yet
- Diabetic Ketoacidosis - PurnaDocument20 pagesDiabetic Ketoacidosis - PurnapurnaNo ratings yet
- 4 BodyDocument35 pages4 Bodysinte beyuNo ratings yet
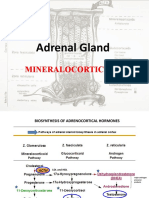
- 4.adrenal Gland & CorticosteroidsDocument65 pages4.adrenal Gland & CorticosteroidsZahidKhanNo ratings yet
- Classical HomocystinuriaDocument34 pagesClassical Homocystinuriapriyanshu mathurNo ratings yet
- Urine Screening For Metabolic DisordersDocument55 pagesUrine Screening For Metabolic DisordersGlormina Asprec AvenaNo ratings yet
- Urinary LithiasisDocument35 pagesUrinary Lithiasishussain AltaherNo ratings yet
- Lect 9 Parathyroid Gland-1Document30 pagesLect 9 Parathyroid Gland-1warda farooqNo ratings yet
- Adrenal Gland by Dr. Rajnee IInd PartDocument30 pagesAdrenal Gland by Dr. Rajnee IInd Part9460106212No ratings yet
- Hypocalcemia: Dept of Nephrology PsriDocument40 pagesHypocalcemia: Dept of Nephrology Psriind78No ratings yet
- Analysis of Abnormal Urine NotesDocument6 pagesAnalysis of Abnormal Urine Notesahteshammirji575No ratings yet
- Urine AnalysisDocument31 pagesUrine AnalysisajaysomNo ratings yet
- Approach To Malabsorption (SANJAY)Document58 pagesApproach To Malabsorption (SANJAY)Sanjay KumarNo ratings yet
- Electrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesDocument44 pagesElectrolyte Imbalances and Their Management.: by Nabawanda Saluwa Facilitator: DR - Ssebuliba MosesNinaNo ratings yet
- Liver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesFrom EverandLiver Cirrhosis, A Simple Guide To The Condition, Treatment And Related DiseasesNo ratings yet
- The Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionFrom EverandThe Renal Diet Kitchen: 60+ Quick and Delicious Renal Diet Recipes to Improve Kidney FunctionNo ratings yet
- A Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesFrom EverandA Simple Guide to Hyperparathyroidism, Treatment and Related DiseasesNo ratings yet
- Low Oxalate Cookbook: Low Oxalate Diet Cookbook With Nutritional Guide To Prevent Kidney StonesFrom EverandLow Oxalate Cookbook: Low Oxalate Diet Cookbook With Nutritional Guide To Prevent Kidney StonesNo ratings yet
- Chapter 133Document16 pagesChapter 133Saloni SaloniNo ratings yet
- AA Digestion, Absorption, Urea CycleDocument62 pagesAA Digestion, Absorption, Urea CycleSaloni SaloniNo ratings yet
- GlycineDocument22 pagesGlycineSaloni SaloniNo ratings yet
- Dr.r.jambhulkar Latest NotesDocument402 pagesDr.r.jambhulkar Latest NotesSaloni Saloni100% (1)
- Carbohydrate Metabolism 08-02-24Document113 pagesCarbohydrate Metabolism 08-02-24Saloni SaloniNo ratings yet
- Quiz On Income TaxationDocument4 pagesQuiz On Income TaxationLenard Josh Ingalla100% (1)
- S No. Category of TSR JR College No. of CollegesDocument8 pagesS No. Category of TSR JR College No. of CollegesLokeshwar VarmaNo ratings yet
- KEEPER of The LOST CITIES Book 9.5's Cover Puts The Spotlight On Keefe - NerdistDocument1 pageKEEPER of The LOST CITIES Book 9.5's Cover Puts The Spotlight On Keefe - Nerdistbyms.2419No ratings yet
- Algebra 2 Ans PDFDocument2 pagesAlgebra 2 Ans PDFPuja AgarwalNo ratings yet
- 21st Century Lesson Module 9 10Document29 pages21st Century Lesson Module 9 10Sky BantingNo ratings yet
- Applause Philippines October 2013Document17 pagesApplause Philippines October 2013mitzi_03No ratings yet
- Conectores y DiagramasDocument6 pagesConectores y Diagramasrodrigo michelNo ratings yet
- Key Events in Europian IntegrationionDocument1 pageKey Events in Europian IntegrationionAdriatik MetaNo ratings yet
- Consti 2 Bill of Rights First 52 CasesDocument1 pageConsti 2 Bill of Rights First 52 CasesRolly Herida100% (1)
- Environmental Term Paper TopicsDocument8 pagesEnvironmental Term Paper Topicsea6p1e99100% (1)
- Simple StressDocument4 pagesSimple StressZachary Via Adag AñascoNo ratings yet
- Khurram Baig: Professional Experience (ISLAM ENGINEERING (PVT) LTD. (Feb-19 To Date) Designation (Chief Accountant)Document2 pagesKhurram Baig: Professional Experience (ISLAM ENGINEERING (PVT) LTD. (Feb-19 To Date) Designation (Chief Accountant)Wazeeer AhmadNo ratings yet
- L2 - ABFA1163 FA II (Student)Document4 pagesL2 - ABFA1163 FA II (Student)Xue YikNo ratings yet
- The Secret Behind The SecretDocument17 pagesThe Secret Behind The SecretCarissa NicholsNo ratings yet
- Siemens-BT300 VFDDocument6 pagesSiemens-BT300 VFDdiansulaemanNo ratings yet
- The Concept of Cohesion and Coherence in Modern Linguistics With Reference To English and KurdishDocument11 pagesThe Concept of Cohesion and Coherence in Modern Linguistics With Reference To English and Kurdishنورا عبد النبي خليفNo ratings yet
- Case Study: Beverage Man Takes The PlungeDocument13 pagesCase Study: Beverage Man Takes The PlungeIkko100% (1)
- Chocolate Cake RecipeTin EatsDocument2 pagesChocolate Cake RecipeTin Eatsantoniapatsalou1No ratings yet
- Sneaky Hypnosis PhrasesDocument4 pagesSneaky Hypnosis PhrasesRaiyanq67% (3)
- CLIC Catalogue PDFDocument28 pagesCLIC Catalogue PDFsangram patilNo ratings yet
- M.Pharm PharmaceuticsDocument13 pagesM.Pharm PharmaceuticsBilla NNo ratings yet
- Online Mca SRMDocument10 pagesOnline Mca SRMGeeky GeekyNo ratings yet
- Evidence OutlineDocument119 pagesEvidence OutlinePaulMarie100% (1)
- Concrete Wall Formwork LOGO.3 - PASCHALDocument3 pagesConcrete Wall Formwork LOGO.3 - PASCHALPartha GorainNo ratings yet
- Job Description GRIDDocument2 pagesJob Description GRIDSwapnil ShethNo ratings yet
- Writing Level 1 International School (Vol. 2) ENG 127: Mã môn họcDocument72 pagesWriting Level 1 International School (Vol. 2) ENG 127: Mã môn họcHồng TheNo ratings yet
- 1111Document9 pages1111trungtroangNo ratings yet
- Grammar Practice 8B - Sofía Sendín B1ADocument1 pageGrammar Practice 8B - Sofía Sendín B1ASofia SendinNo ratings yet
- Business Startup CostsDocument11 pagesBusiness Startup CostsRaul CollazziNo ratings yet