Download as pptx, pdf, or txt
You might also like
- PD22 Hap1 L03Document33 pagesPD22 Hap1 L03Ka Yan LAUNo ratings yet
- ENDOCRINE SYSTEM DISORDERS PROPER BestDocument370 pagesENDOCRINE SYSTEM DISORDERS PROPER BestronaronixstheboyNo ratings yet
- Endocine System Physiology 20-4-2020Document61 pagesEndocine System Physiology 20-4-2020Farah AljayyousiNo ratings yet
- Endocrinology Endocrinology: H. KibichoDocument370 pagesEndocrinology Endocrinology: H. KibichoMursal RashidNo ratings yet
- Endocrine PhysiologyDocument79 pagesEndocrine PhysiologyCHALIE MEQUNo ratings yet
- 5-17 Endocrine HandoutDocument10 pages5-17 Endocrine HandoutJohn Lawrence YbanezNo ratings yet
- Endocrine System in FinfishesDocument43 pagesEndocrine System in FinfishesMisbah SayyedNo ratings yet
- Endocrine SystemDocument133 pagesEndocrine SystemAudrey KenfacNo ratings yet
- HypothalamusDocument9 pagesHypothalamussnowNo ratings yet
- Endocrine System - MorphophysiologyDocument88 pagesEndocrine System - MorphophysiologyKarina Bustillo100% (1)
- Endocrine Physiology For Pharmacy Students-2023Document118 pagesEndocrine Physiology For Pharmacy Students-2023Alemnew YohannesNo ratings yet
- Chapter 7 - Endocrine SystemsDocument51 pagesChapter 7 - Endocrine Systemsnokate konkoorNo ratings yet
- Ila College of Health: Endocrine PhysiologyDocument40 pagesIla College of Health: Endocrine PhysiologyDaniel DendaNo ratings yet
- The Endocrine SystemDocument191 pagesThe Endocrine SystemRiska PriyaniNo ratings yet
- Endocrine System - HANDOUTSDocument20 pagesEndocrine System - HANDOUTSMeegs EstabilloNo ratings yet
- Hypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2018 Lectures 1-2 March 14 2018Document213 pagesHypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2018 Lectures 1-2 March 14 2018rachid09No ratings yet
- MED 2056 Exam #1 Content 2018Document33 pagesMED 2056 Exam #1 Content 2018Marcelyn Chupoco CataligNo ratings yet
- Anatomy and Physiology of The Endocrine System: Presenté ParDocument64 pagesAnatomy and Physiology of The Endocrine System: Presenté ParYackson Frank100% (1)
- Endocrine PhysiologyDocument76 pagesEndocrine Physiologykidusabeje7No ratings yet
- Endocrine System: Clarence L. Nuval, RMT, MDDocument66 pagesEndocrine System: Clarence L. Nuval, RMT, MDCla NuvalNo ratings yet
- Introduction Endocrine Physiology 2Document52 pagesIntroduction Endocrine Physiology 2IshaqNo ratings yet
- BBT221 Lecture 6Document41 pagesBBT221 Lecture 6Al Sabri Bhuiyan 1812098042No ratings yet
- ENDOCRINE SYSTEM - LABORATORY With Side NotesDocument68 pagesENDOCRINE SYSTEM - LABORATORY With Side Notesp2zspgtchjNo ratings yet
- EndocrineDocument70 pagesEndocrinehamidNo ratings yet
- Fundamentals in Nursing Practice ReviewerDocument1 pageFundamentals in Nursing Practice ReviewerXharen Joy BinondoNo ratings yet
- Endocrine Glands and HormonesDocument46 pagesEndocrine Glands and Hormonesfisherp1No ratings yet
- Estrutura e Função Do Sistema Hipófise-HipotálamoDocument49 pagesEstrutura e Função Do Sistema Hipófise-HipotálamoMicheli CastroNo ratings yet
- Feedback Mechanism of Endocrine System, Reproductive SystemDocument19 pagesFeedback Mechanism of Endocrine System, Reproductive Systemnhel gutierrezNo ratings yet
- Hormon AjarDocument62 pagesHormon AjarLiana Ika SuwandyNo ratings yet
- EndocrineDocument94 pagesEndocrineHira NawazNo ratings yet
- 439 en Intro 1Document74 pages439 en Intro 1Omotosho DavidNo ratings yet
- Introduction To EndocrinologyDocument22 pagesIntroduction To EndocrinologyUrwah KhanNo ratings yet
- Care of Clients With Problem On EndocrineDocument48 pagesCare of Clients With Problem On EndocrineAngel CauilanNo ratings yet
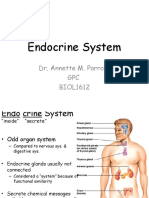
- Endocrine System: Dr. Annette M. Parrott GPC BIOL1612Document34 pagesEndocrine System: Dr. Annette M. Parrott GPC BIOL1612Nathan TaylorNo ratings yet
- Hypothalamus & Pituitary GlandDocument39 pagesHypothalamus & Pituitary GlandVishal DodejaNo ratings yet
- Hormonal Regulation of ExerciseDocument11 pagesHormonal Regulation of ExerciseMozil Fadzil KamarudinNo ratings yet
- Lecture 9 - Humoral RegulationDocument74 pagesLecture 9 - Humoral Regulationbadarbhai222No ratings yet
- Lecture 1.Document27 pagesLecture 1.abdelrazeq zarourNo ratings yet
- EndocrinologyDocument74 pagesEndocrinologysyedahaleemajunaidsNo ratings yet
- Endocrine System: 1. DefinationDocument11 pagesEndocrine System: 1. DefinationMaleeha Ayub100% (1)
- Nervous Vs HormoneDocument106 pagesNervous Vs HormoneakupunadaNo ratings yet
- Anaphy EndocrinesystemDocument143 pagesAnaphy EndocrinesystemSCARLETH GACIASNo ratings yet
- Structure and Function of The Endocrine SystemDocument53 pagesStructure and Function of The Endocrine Systemwalt65No ratings yet
- Endocrine System Group 9Document77 pagesEndocrine System Group 9Jei SanNo ratings yet
- Hormones:: Signaling MoleculesDocument20 pagesHormones:: Signaling MoleculesSangeeta DwivediNo ratings yet
- Regulasi Endokrin 22 IntensifDocument25 pagesRegulasi Endokrin 22 IntensifWignes WarenNo ratings yet
- Hypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2017 Lectures 1-2 March 20 2018Document197 pagesHypothlamic-Pituitary Physiology: Mona Abou Chebl MD. METABOLISM-2017 Lectures 1-2 March 20 2018rachid09No ratings yet
- The Endocrine System: HormonesDocument948 pagesThe Endocrine System: HormonesMahaaaNo ratings yet
- What Is Human Endocrine SystemDocument38 pagesWhat Is Human Endocrine SystemNatukunda DianahNo ratings yet
- Form 5 Note Chapter 3Document54 pagesForm 5 Note Chapter 3Balan MuthuNo ratings yet
- Endocrine System Endocrine System: "The Body Regulator"Document31 pagesEndocrine System Endocrine System: "The Body Regulator"angelus008No ratings yet
- The Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1Document12 pagesThe Endocrine System The Endocrine System: © 2018 Pearson Education, Ltd. 1lourd nabNo ratings yet
- Endocrine System-1Document90 pagesEndocrine System-1markmuiruri581No ratings yet
- 3.3 The Role of Hormones in HumansDocument35 pages3.3 The Role of Hormones in HumansIMELDANo ratings yet
- ReportDocument18 pagesReportrtvb77smjhNo ratings yet
- Endocrine SystemDocument69 pagesEndocrine SystemDivya JaiswalNo ratings yet
- Activity 16 HormonesDocument16 pagesActivity 16 HormonesKendrix Aguiluz FlorendoNo ratings yet
- Glandular SystemDocument18 pagesGlandular SystemAashishNo ratings yet
- Endocrine System: A Tutorial Study GuideFrom EverandEndocrine System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (1)
- 2023 MID - Mental Illness - Drug List - 010323Document29 pages2023 MID - Mental Illness - Drug List - 010323Harrison Dela CruzNo ratings yet
- DocumentDocument3 pagesDocumentHarrison Dela CruzNo ratings yet
- EseDocument6 pagesEseHarrison Dela CruzNo ratings yet
- 3 3Document2 pages3 3Harrison Dela CruzNo ratings yet
- Psychopharmacology: New Frontiers in Treating Mental Health DisordersDocument13 pagesPsychopharmacology: New Frontiers in Treating Mental Health DisordersHarrison Dela CruzNo ratings yet
- AbstrDocument1 pageAbstrHarrison Dela CruzNo ratings yet
- NMM Gold TutorialDocument7 pagesNMM Gold TutorialTane67No ratings yet
- Just For Fun (Unit 4) : Page 1 of 2Document2 pagesJust For Fun (Unit 4) : Page 1 of 2Wilmer BalonNo ratings yet
- A The TempestDocument10 pagesA The TempestBouchra BouchraNo ratings yet
- Lesson 2 - Duties of A Painting (Coatings) InspectorDocument55 pagesLesson 2 - Duties of A Painting (Coatings) InspectorFarhad AsadulovNo ratings yet
- Contengency PlanDocument10 pagesContengency PlanFernando Dumar Mannod Jr.No ratings yet
- Enerpac WMC Series CatalogDocument1 pageEnerpac WMC Series CatalogTitanplyNo ratings yet
- VaricoceleDocument4 pagesVaricoceleRahajeng Ainiken PutririmasariNo ratings yet
- Advanced Clinical Naturopathic Medicine Leah Hechtman 2 Full Chapter PDFDocument69 pagesAdvanced Clinical Naturopathic Medicine Leah Hechtman 2 Full Chapter PDFsapitonuk100% (8)
- Regina D Perry CV 2015Document8 pagesRegina D Perry CV 2015api-284587833No ratings yet
- IAS 36 Impairment of Assets (2021)Document12 pagesIAS 36 Impairment of Assets (2021)Tawanda Tatenda HerbertNo ratings yet
- NadiahBamadhaj DescentDocument24 pagesNadiahBamadhaj DescentAbu WafaNo ratings yet
- Pipe's Minor LossesDocument95 pagesPipe's Minor LossesJosept RevueltaNo ratings yet
- Network Automation 7 0 5 ReleaseNotes PDFDocument23 pagesNetwork Automation 7 0 5 ReleaseNotes PDFSebastian ChaconNo ratings yet
- 111 F21 Research Paper ProposalDocument2 pages111 F21 Research Paper ProposalKim LaceyNo ratings yet
- Fantasy Foundry (10032611)Document8 pagesFantasy Foundry (10032611)Oscar Chacon100% (1)
- S.No Acc No Title of The BookDocument12 pagesS.No Acc No Title of The BookmechhodNo ratings yet
- IronDocument27 pagesIronAyman LatifNo ratings yet
- CG Report ADocument8 pagesCG Report AsachinNo ratings yet
- SGP TR 012Document276 pagesSGP TR 012Kevin Devalentino Versi IINo ratings yet
- Presented By: Ujjwal Jaryal RF17E1A05Document9 pagesPresented By: Ujjwal Jaryal RF17E1A05Ujjwal JaryalNo ratings yet
- Ex Rates 19 03 19Document9 pagesEx Rates 19 03 19Anonymous jTY4ExMNo ratings yet
- High Lift Hydraulic Transmission Jacks "AF25082" "AF50080" "AF100080"Document6 pagesHigh Lift Hydraulic Transmission Jacks "AF25082" "AF50080" "AF100080"Alain DefoeNo ratings yet
- Nair Rodriguez-Hornedo PDFDocument34 pagesNair Rodriguez-Hornedo PDFAenhiequrra AlthafunnisaNo ratings yet
- Working Paper No. 561 PDFDocument34 pagesWorking Paper No. 561 PDFdilipkumar boinwadNo ratings yet
- Project Report "Solidworks" Six Months Software Training Project ReportDocument56 pagesProject Report "Solidworks" Six Months Software Training Project ReportakashNo ratings yet
- Crim 1 BDocument1 pageCrim 1 BJose Antonio Peralta Achaval Jr.No ratings yet
- Classification of Imbalanced Malaria Disease UsingDocument5 pagesClassification of Imbalanced Malaria Disease Usinglubna gemaaNo ratings yet
- Students CircularDocument2 pagesStudents CirculargeraltNo ratings yet
- Circular Flow LessonDocument13 pagesCircular Flow LessonKimball SarmientoNo ratings yet
- Arch232 HW 3Document3 pagesArch232 HW 3Carl Justin PantaleonNo ratings yet